You might also like
- Clinical Approach To A Patient With Dysphagia: Medicine UpdateDocument3 pagesClinical Approach To A Patient With Dysphagia: Medicine UpdateAnonymous XFDJfsGviNo ratings yet
- DysphagiaDocument38 pagesDysphagiaحميد حيدرNo ratings yet
- Esophageal DysphagiaDocument3 pagesEsophageal Dysphagianevelle4667No ratings yet
- 1 Esophagus SG 2021 After Class FinalDocument28 pages1 Esophagus SG 2021 After Class FinalTyler YounNo ratings yet
- GIT Disorders Guide Covers Esophageal and Gastric Motility IssuesDocument11 pagesGIT Disorders Guide Covers Esophageal and Gastric Motility IssuesSara JosephNo ratings yet
- Gastroenterology:: Motility Disorders of Esophagus, GERDDocument46 pagesGastroenterology:: Motility Disorders of Esophagus, GERDPatricia May CruzNo ratings yet
- Dysphagia DiseaseDocument212 pagesDysphagia DiseaseAprita NurkarimaNo ratings yet
- Esophagus Symptoms and InvestigationDocument7 pagesEsophagus Symptoms and InvestigationJinNo ratings yet
- Examination and Superficial Palpation of The AbdomenDocument38 pagesExamination and Superficial Palpation of The AbdomenРопннпгпNo ratings yet
- Intestinal Obstruction in Paediatrics - James GathogoDocument21 pagesIntestinal Obstruction in Paediatrics - James GathogoMalueth Angui100% (1)
- Radiology of Gastrointestinal Congenital and Inflammatory DiseasesDocument5 pagesRadiology of Gastrointestinal Congenital and Inflammatory DiseasesAlvin Karl ValenciaNo ratings yet
- AchalaciaDocument2 pagesAchalaciaticolorjNo ratings yet
- 3 - Esophageal Function and Achalasia SlaytDocument20 pages3 - Esophageal Function and Achalasia SlaytZeynep ArasNo ratings yet
- ND RDDocument22 pagesND RDKatie Marie Wilson100% (1)
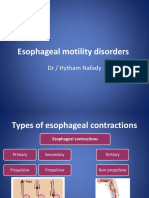
- Esophageal Motility Disorders: DR / Hytham NafadyDocument31 pagesEsophageal Motility Disorders: DR / Hytham NafadyRabie MeramNo ratings yet
- Esophagial DiseasDocument83 pagesEsophagial Diseasnajib.atif17No ratings yet
- NCM 116N - TransDocument9 pagesNCM 116N - TransNEIL NETTE S. REYNALDONo ratings yet
- Dysphagia Lesson 2Document40 pagesDysphagia Lesson 2Raina FujiyoshiNo ratings yet
- Benign Disease of The Esophagus PDFDocument4 pagesBenign Disease of The Esophagus PDFSpecialNameNo ratings yet
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocument84 pagesTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimNo ratings yet
- Diseases of Esophagus.Document3 pagesDiseases of Esophagus.Isabel Castillo100% (1)
- 1 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionDocument6 pages1 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionKylle AlimosaNo ratings yet
- Achalasia: A Review of Etiology, Pathophysiology, and TreatmentDocument6 pagesAchalasia: A Review of Etiology, Pathophysiology, and TreatmentAprita NurkarimaNo ratings yet
- Achalasia Review: Causes, Mechanisms, TreatmentsDocument6 pagesAchalasia Review: Causes, Mechanisms, TreatmentsNona HenNo ratings yet
- Achalasia: A Review of Etiology, Pathophysiology, and TreatmentDocument6 pagesAchalasia: A Review of Etiology, Pathophysiology, and TreatmentNona HenNo ratings yet
- Bowel ObstructionsDocument24 pagesBowel ObstructionsArchie ZhangNo ratings yet
- Obstetrics - GastrointestinalDocument6 pagesObstetrics - GastrointestinalJonathanNo ratings yet
- Gastrolat 2014 S 100005Document5 pagesGastrolat 2014 S 100005Dalia CastroNo ratings yet
- AchalasiaDocument12 pagesAchalasianaveen kashyapNo ratings yet
- Diverticular Disease and Intestinal ObstructionDocument31 pagesDiverticular Disease and Intestinal ObstructionPauLa Cheneree Peña ÜNo ratings yet
- Esophageal Motility DisordersDocument44 pagesEsophageal Motility DisordersMarc Michael Dela CruzNo ratings yet
- A UGI (blue keyword pyq)Document3 pagesA UGI (blue keyword pyq)Irsyad SiddeeqNo ratings yet
- Approach To The Patient With Dysphagia PDFDocument7 pagesApproach To The Patient With Dysphagia PDFHo Yong Wai100% (1)
- Written Report GERDDocument11 pagesWritten Report GERDAlthea AlbaniaNo ratings yet
- Mechanical Causes of Intestinal ObstructionDocument5 pagesMechanical Causes of Intestinal ObstructionKimberly Subade MandilagNo ratings yet
- L28 - Esophageal DiseasesDocument16 pagesL28 - Esophageal DiseasesNimer Abdelhadi AliNo ratings yet
- RLQ PainDocument20 pagesRLQ PainBEATRICE SOPHIA PARMANo ratings yet
- SummerTerm TopicOutline1Document20 pagesSummerTerm TopicOutline1Rachelle DelantarNo ratings yet
- Ms Prelim NotesDocument6 pagesMs Prelim NotesJane LaquihonNo ratings yet
- Test 2 NotesDocument38 pagesTest 2 Notesbjpalmer100% (2)
- Intestinal Obstruction PDFDocument4 pagesIntestinal Obstruction PDFKiiza AloysiusNo ratings yet
- Gastrointestinal System: Symptomatology of TheDocument85 pagesGastrointestinal System: Symptomatology of TheAbdelrahman MokhtarNo ratings yet
- Esophageal DiverticulaDocument18 pagesEsophageal DiverticulaAbigail BascoNo ratings yet
- Differential Diagnosis of Gastrointestinal DiseasesDocument5 pagesDifferential Diagnosis of Gastrointestinal DiseasesSean Dominique Cruz MaghinayNo ratings yet
- OesophagusDocument15 pagesOesophagusIBRAHEM JUMAHNo ratings yet
- Medical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersDocument34 pagesMedical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersRomelyn Ordillas100% (2)
- Esophageal Cancer Diagnosis and ManagementDocument6 pagesEsophageal Cancer Diagnosis and Managementhtt.pNo ratings yet
- SURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Document13 pagesSURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Medisina101No ratings yet
- Physical AssessmentDocument14 pagesPhysical AssessmentMaria ThereseNo ratings yet
- Dr. Rami Radilology LecDocument25 pagesDr. Rami Radilology LecmarwaalgheilaniNo ratings yet
- Gi SurgDocument42 pagesGi Surgbob marleyNo ratings yet
- 4 U1.0 B978 1 4160 6189 2..00012 3..DOCPDFDocument9 pages4 U1.0 B978 1 4160 6189 2..00012 3..DOCPDFJuan HernandezNo ratings yet
- 4 PDFDocument6 pages4 PDFYigit İskurtNo ratings yet
- GERD and Hiatal Hernia GuideDocument4 pagesGERD and Hiatal Hernia GuideAmoroso, Marian Corneth D.No ratings yet
- Intestinal Obstruction Guide: Causes, Symptoms and TreatmentDocument87 pagesIntestinal Obstruction Guide: Causes, Symptoms and TreatmentJoher MendezNo ratings yet
- Symptoms and causes of esophageal diseaseDocument33 pagesSymptoms and causes of esophageal diseaseRakesh PathrabeNo ratings yet
- Ileus Pada Pediatrik: Syifa Sari Siregar 170100090Document39 pagesIleus Pada Pediatrik: Syifa Sari Siregar 170100090AmardiasNo ratings yet
- Paralytic Ileus: Prepared By: Laurence A. Adena, ManDocument43 pagesParalytic Ileus: Prepared By: Laurence A. Adena, ManJanah Beado PagayNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Achalasia, (Swallowing Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAchalasia, (Swallowing Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- FentonTech Wastewater Ghernaout 2020Document29 pagesFentonTech Wastewater Ghernaout 2020BrankNo ratings yet
- Healthy Chicken Pasta Recipes From EatingWell MagazineDocument10 pagesHealthy Chicken Pasta Recipes From EatingWell MagazineAlice GiffordNo ratings yet
- Russell Vs Vestil 304 SCRA 738Document2 pagesRussell Vs Vestil 304 SCRA 738Joshua L. De JesusNo ratings yet
- Individual Learning Monitoring PlanDocument2 pagesIndividual Learning Monitoring PlanJohnArgielLaurenteVictorNo ratings yet
- Lipid ChemistryDocument93 pagesLipid ChemistrySanreet RandhawaNo ratings yet
- Lesson Plan 1Document9 pagesLesson Plan 1Dama Grace Casabuena100% (1)
- Women in PoliticsDocument13 pagesWomen in PoliticsMusa M. KamaraNo ratings yet
- Human Rights DefinitionDocument2 pagesHuman Rights DefinitionFathiah MhNo ratings yet
- Document PDFDocument16 pagesDocument PDFnelson_herreraNo ratings yet
- ĐỀ THI THỬ ĐH - Mã 129 (Smartie)Document6 pagesĐỀ THI THỬ ĐH - Mã 129 (Smartie)Hoang Huy NguyenNo ratings yet
- Can or Can't Esl Worksheet With Animals Vocabulary For Kids PDFDocument2 pagesCan or Can't Esl Worksheet With Animals Vocabulary For Kids PDFופאאכאלד50% (4)
- Quiz Microeconomics BECO201 Date 30/10/2017 Name: IDDocument5 pagesQuiz Microeconomics BECO201 Date 30/10/2017 Name: IDAA BB MMNo ratings yet
- Consumer BehaviourDocument30 pagesConsumer BehaviourManoj BaghelNo ratings yet
- Cyber Crime and Law ClassDocument99 pagesCyber Crime and Law ClassMohd ShifanNo ratings yet
- 2013 Typhoon YolandaDocument7 pages2013 Typhoon YolandaDieanne MaeNo ratings yet
- The Complete Motown CatalogueDocument10 pagesThe Complete Motown Cataloguehermeto0% (1)
- The Paul Sellers Router PlaneDocument6 pagesThe Paul Sellers Router PlaneAjay Vishwanath100% (1)
- 7 Tips For A Tidy Desk - ExercisesDocument4 pages7 Tips For A Tidy Desk - Exercisesjosh acNo ratings yet
- Hitachi - AssignmentDocument6 pagesHitachi - AssignmentPraveena IvanaNo ratings yet
- Calculating parameters for a basic modern transistor amplifierDocument189 pagesCalculating parameters for a basic modern transistor amplifierionioni2000No ratings yet
- Encounters 3Document4 pagesEncounters 3lgwqmsiaNo ratings yet
- 47 Syeda Nida Batool Zaidi-1Document10 pages47 Syeda Nida Batool Zaidi-1Eiman ShahzadNo ratings yet
- A. Music G8 Fourth QuarterDocument7 pagesA. Music G8 Fourth Quarterjason bernalNo ratings yet
- CPSC5125 - Assignment 3 - Fall 2014 Drawing Polygons: DescriptionDocument2 pagesCPSC5125 - Assignment 3 - Fall 2014 Drawing Polygons: DescriptionJo KingNo ratings yet
- 9331 DCCBDocument5 pages9331 DCCBgopimodalavalasaNo ratings yet
- Human, AGV or AIV? An Integrated Framework For Material Handling System Selection With Real-World Application in An Injection Molding FacilityDocument10 pagesHuman, AGV or AIV? An Integrated Framework For Material Handling System Selection With Real-World Application in An Injection Molding FacilitymertikNo ratings yet
- Muster Roll 24Document2 pagesMuster Roll 24Admirable AntoNo ratings yet
- Resume AmarDocument3 pagesResume AmarAshraf YusofNo ratings yet
- LTC exemption and tax on retrenchment compensationDocument2 pagesLTC exemption and tax on retrenchment compensationhanumanthaiahgowdaNo ratings yet
- The Carb Cycling Codex ThibaudeuDocument30 pagesThe Carb Cycling Codex ThibaudeuOrlando Paez Cortazar100% (1)