You might also like
- Laryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandLaryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 3.5 out of 5 stars3.5/5 (2)
- Barretts EsophagusDocument21 pagesBarretts EsophagusLyka DimayacyacNo ratings yet
- Theodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDocument7 pagesTheodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDaniel AdityaNo ratings yet
- GerdDocument8 pagesGerdLoms KotopNo ratings yet
- Gastroesophageal Reflux Disease: L. V. Borisova Docent., Ph. DDocument32 pagesGastroesophageal Reflux Disease: L. V. Borisova Docent., Ph. DSalma Mohamed RezkNo ratings yet
- Gastroesophageal Reflux Disease - RepairedDocument40 pagesGastroesophageal Reflux Disease - RepairedSowndharyaNo ratings yet
- 1 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionDocument6 pages1 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionKylle AlimosaNo ratings yet
- 1 GerdDocument10 pages1 GerdRana EL-BakryNo ratings yet
- GI Disorders - GERD and PUDDocument5 pagesGI Disorders - GERD and PUDmollymaheshwari00No ratings yet
- OesophagusDocument15 pagesOesophagusIBRAHEM JUMAHNo ratings yet
- GerdDocument37 pagesGerdAyesha ShafiqNo ratings yet
- GERD Definition, Patho and TreatmentDocument7 pagesGERD Definition, Patho and TreatmentGeethika GummadiNo ratings yet
- NCM 116N - TransDocument9 pagesNCM 116N - TransNEIL NETTE S. REYNALDONo ratings yet
- GERDDocument20 pagesGERDSINDHOOR S MNo ratings yet
- Gastro-Oesophageal Reflux Disease (GORD) : Anish DhakalDocument31 pagesGastro-Oesophageal Reflux Disease (GORD) : Anish DhakalnrauliaprtwNo ratings yet
- Esophageal Disorder Part IIDocument27 pagesEsophageal Disorder Part IIJuma AwarNo ratings yet
- GerdDocument28 pagesGerdEbraheam HadiNo ratings yet
- Gastro Surgery PptsDocument627 pagesGastro Surgery Pptszein0217zienNo ratings yet
- GERD - PPT 11Document30 pagesGERD - PPT 11pharmaguy111No ratings yet
- Esophageal PathologyDocument8 pagesEsophageal PathologyAndra BauerNo ratings yet
- Gastrointestinal Surgery 2021Document80 pagesGastrointestinal Surgery 2021Esraa SalemNo ratings yet
- L28 - Esophageal DiseasesDocument16 pagesL28 - Esophageal DiseasesNimer Abdelhadi AliNo ratings yet
- Gastroenterology:: Motility Disorders of Esophagus, GERDDocument46 pagesGastroenterology:: Motility Disorders of Esophagus, GERDPatricia May CruzNo ratings yet
- Text Book Reading CacaDocument23 pagesText Book Reading Cacapramuliansyah haqNo ratings yet
- DysphagiaDocument38 pagesDysphagiaحميد حيدرNo ratings yet
- 2019 AGA DDSEP 9 Chapter 1 1557871635169Document28 pages2019 AGA DDSEP 9 Chapter 1 1557871635169Emilia GarciaNo ratings yet
- K11 Bedah EsofagusDocument37 pagesK11 Bedah EsofagusenriNo ratings yet
- Kuliah Upper Gi Tract DiseaseDocument78 pagesKuliah Upper Gi Tract DiseaseAnggun Pulihana WNo ratings yet
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- Brede No Ord 2013Document10 pagesBrede No Ord 2013Jonathan ArifputraNo ratings yet
- Disturbances in Digestion and AbsorptionDocument115 pagesDisturbances in Digestion and AbsorptionGabrielle PamaNo ratings yet
- Vaagdevi Phamacy CollegeDocument27 pagesVaagdevi Phamacy CollegeLalith VarmaNo ratings yet
- Gerd and Hiatal HerniaDocument4 pagesGerd and Hiatal HerniaAmoroso, Marian Corneth D.No ratings yet
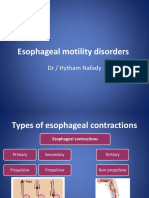
- Esophageal Motility Disorders: DR / Hytham NafadyDocument31 pagesEsophageal Motility Disorders: DR / Hytham NafadyRabie MeramNo ratings yet
- Problem 2 Gastrointestinal System: Ryan Juliansyah 405130048 University of TarumanagaraDocument76 pagesProblem 2 Gastrointestinal System: Ryan Juliansyah 405130048 University of TarumanagaraRyan Juliansyah ZeinNo ratings yet
- Gastroesophageal Reflux DiseaseDocument37 pagesGastroesophageal Reflux DiseaseMahad Maxamed AxmedNo ratings yet
- GIT - GAstric Phys PaperDocument5 pagesGIT - GAstric Phys PaperAnosDocNo ratings yet
- Dispepsia 1Document29 pagesDispepsia 1industrial health2019No ratings yet
- Medical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersDocument34 pagesMedical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersRomelyn Ordillas100% (2)
- Class 7 (G1) - GI TractDocument112 pagesClass 7 (G1) - GI TractAdel mohammadNo ratings yet
- Clinical Approach To A Patient With Dysphagia: Medicine UpdateDocument3 pagesClinical Approach To A Patient With Dysphagia: Medicine UpdateAnonymous XFDJfsGviNo ratings yet
- Gastro Esophageal Reflux DiseaseDocument45 pagesGastro Esophageal Reflux DiseaseHarry FaisalNo ratings yet
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocument84 pagesTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimNo ratings yet
- Gerd Blok 2 6Document43 pagesGerd Blok 2 6Mus TofaNo ratings yet
- K-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUDocument38 pagesK-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUChristian Lumban GaolNo ratings yet
- Textbook Discussion GerdDocument3 pagesTextbook Discussion GerdgranmatadorNo ratings yet
- Gastro-Esophageal Reflux Disease ( GERD)Document31 pagesGastro-Esophageal Reflux Disease ( GERD)Malueth AnguiNo ratings yet
- 6-7 - Medical Nursing - GIS DisordersDocument108 pages6-7 - Medical Nursing - GIS DisordersmichaelNo ratings yet
- Esophageal DiseasesDocument9 pagesEsophageal DiseasesRashed ShatnawiNo ratings yet
- GerdDocument51 pagesGerdHoney LaxNo ratings yet
- GERDDocument24 pagesGERDBEVERLY JANE COPADANo ratings yet
- Dyspepsia FinalDocument52 pagesDyspepsia FinalAfifah SelamatNo ratings yet
- Martamala2001 (Bile Reflux)Document7 pagesMartamala2001 (Bile Reflux)askhaeraniNo ratings yet
- 2 CARE OF CLIENTS GERD HIATAL HERNIA ACHALASIA PUD GI BLEEDING FinalDocument114 pages2 CARE OF CLIENTS GERD HIATAL HERNIA ACHALASIA PUD GI BLEEDING Finalevren yilmazNo ratings yet
- Disease of Esophagus and Hiatal HerniaDocument76 pagesDisease of Esophagus and Hiatal HerniaSiriporn PongpattarapakNo ratings yet
- GASTROPARESISDocument92 pagesGASTROPARESISGlobe MedicareNo ratings yet
- Barium SwallowDocument24 pagesBarium SwallowFaria KhanNo ratings yet
- Pemicu 1 GITDocument13 pagesPemicu 1 GITEric RicardoNo ratings yet
- 10-02-20. Deed of Donation SSF Equipment - SSF On Vermicomposting (Formerly Large Scale Vermi Composting Production)Document3 pages10-02-20. Deed of Donation SSF Equipment - SSF On Vermicomposting (Formerly Large Scale Vermi Composting Production)Catherine BenbanNo ratings yet
- Manuel Vs AlfecheDocument2 pagesManuel Vs AlfecheGrace0% (1)
- Principles of Marketing: Quarter 1 - Module 6: Marketing ResearchDocument17 pagesPrinciples of Marketing: Quarter 1 - Module 6: Marketing ResearchAmber Dela Cruz100% (1)
- Summer Anniversary: by Chas AdlardDocument3 pagesSummer Anniversary: by Chas AdlardAntonette LavisoresNo ratings yet
- Machiavelli's Political Philosophy and Jamaican PoliticsDocument2 pagesMachiavelli's Political Philosophy and Jamaican PoliticsAndre RobinsonNo ratings yet
- FAR09 Biological Assets - With AnswerDocument9 pagesFAR09 Biological Assets - With AnswerAJ Cresmundo50% (4)
- Marina AbramovićDocument2 pagesMarina AbramovićTatiana AlbuNo ratings yet
- Khenpo Tsultrim Gyamtso Rinpoche - Meditation On EmptinessDocument206 pagesKhenpo Tsultrim Gyamtso Rinpoche - Meditation On Emptinessdorje@blueyonder.co.uk100% (1)
- Multiple ChoiceDocument3 pagesMultiple ChoiceEfrelyn CasumpangNo ratings yet
- Jeoparty Fraud Week 2022 EditableDocument65 pagesJeoparty Fraud Week 2022 EditableRhea SimoneNo ratings yet
- Aar604 Lecture 3Document55 pagesAar604 Lecture 3Azizul100% (1)
- Network Monitoring & Forensics: Jim IrvingDocument102 pagesNetwork Monitoring & Forensics: Jim IrvingKarel GoldmannNo ratings yet
- Derichebourg - Universal Registration Document 2020-2021Document256 pagesDerichebourg - Universal Registration Document 2020-2021Abhijeet ShindeNo ratings yet
- Agreement of PurchaseDocument8 pagesAgreement of PurchaseAdv. Govind S. TehareNo ratings yet
- KCET MOCK TEST PHY Mock 2Document8 pagesKCET MOCK TEST PHY Mock 2VikashNo ratings yet
- Back WagesDocument24 pagesBack WagesfaisalfarizNo ratings yet
- McEwan Pacific Student Scholarship 1374 RegulationsDocument2 pagesMcEwan Pacific Student Scholarship 1374 RegulationsHaitelenisia Hei'ululua KAMANo ratings yet
- Historical Background of Land Ownership in The PhilippinesDocument2 pagesHistorical Background of Land Ownership in The Philippinesjohn100% (1)
- 2beloved Lizzo PDFDocument1 page2beloved Lizzo PDFAntwerpQueerChoir AQCNo ratings yet
- Temple ManualDocument21 pagesTemple Manualapi-298785516No ratings yet
- Grill Restaurant Business Plan TemplateDocument11 pagesGrill Restaurant Business Plan TemplateSemira SimonNo ratings yet
- Ppivspiandpi G.R. No. 167715 November 17, 2010 Petitioner Respondents: Pfizer, Inc. and Pfizer (Phil.) Inc., TopicDocument26 pagesPpivspiandpi G.R. No. 167715 November 17, 2010 Petitioner Respondents: Pfizer, Inc. and Pfizer (Phil.) Inc., TopicMc Whin CobainNo ratings yet
- Discuss The Following Questions With Your Family Members Casually and Write The AnswersDocument2 pagesDiscuss The Following Questions With Your Family Members Casually and Write The AnswersVincent Stephen AmalrajNo ratings yet
- Order of Nine Angles: RealityDocument20 pagesOrder of Nine Angles: RealityBrett StevensNo ratings yet
- Bacanie 2400 Articole Cu Cod de BareDocument12 pagesBacanie 2400 Articole Cu Cod de BareGina ManolacheNo ratings yet
- Transport System in Living ThingsDocument40 pagesTransport System in Living ThingsHarijani SoekarNo ratings yet
- Developmental PsychologyDocument2 pagesDevelopmental PsychologyPatricia Xandra AurelioNo ratings yet
- Diffusion Osmosis Enzymes Maths and Write Up Exam QuestionsDocument9 pagesDiffusion Osmosis Enzymes Maths and Write Up Exam QuestionsArooj AbidNo ratings yet
- How To Play Casino - Card Game RulesDocument1 pageHow To Play Casino - Card Game RulesNouka VENo ratings yet
- Case Study GingerDocument2 pagesCase Study Gingersohagdas0% (1)