You might also like
- GerdDocument37 pagesGerdAyesha ShafiqNo ratings yet
- GerdDocument8 pagesGerdLoms KotopNo ratings yet
- Gastroesophageal Reflux Disease PharmacotherapyDocument22 pagesGastroesophageal Reflux Disease PharmacotherapyrinirhynNo ratings yet
- Gastroesophageal Reflux Disease: Heba Mohammed Abdella Professor of Tropical Medicine, Ain Shams UniversityDocument67 pagesGastroesophageal Reflux Disease: Heba Mohammed Abdella Professor of Tropical Medicine, Ain Shams Universityأحمد الجزارNo ratings yet
- 2019 AGA DDSEP 9 Chapter 1 1557871635169Document28 pages2019 AGA DDSEP 9 Chapter 1 1557871635169Emilia GarciaNo ratings yet
- OesophagusDocument15 pagesOesophagusIBRAHEM JUMAHNo ratings yet
- Case ReportDocument6 pagesCase ReportMae GandaNo ratings yet
- GERD Pathophysiology Cleveland ClinicDocument17 pagesGERD Pathophysiology Cleveland ClinicMavisNo ratings yet
- Non-Neoplastic Disorders of the EsophagusDocument32 pagesNon-Neoplastic Disorders of the EsophagusSindhu BabuNo ratings yet
- GerdDocument28 pagesGerdEbraheam HadiNo ratings yet
- Laryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandLaryngopharyngeal Reflux, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 3.5 out of 5 stars3.5/5 (2)
- Chris L. Place, MD January 27, 2005Document56 pagesChris L. Place, MD January 27, 2005Satrasala AshokkumarNo ratings yet
- Management of Gastroesophagea L Reflux in ElderlyDocument40 pagesManagement of Gastroesophagea L Reflux in ElderlyPrimarini RiatiNo ratings yet
- Gerd by Iyas AlakielDocument23 pagesGerd by Iyas Alakielraph faithNo ratings yet
- Gastro-Oesophageal Reflux Disease (GORD) : Anish DhakalDocument31 pagesGastro-Oesophageal Reflux Disease (GORD) : Anish DhakalnrauliaprtwNo ratings yet
- Esophagial DiseasDocument83 pagesEsophagial Diseasnajib.atif17No ratings yet
- Diseases of OesophagusDocument46 pagesDiseases of OesophagusBrother GeorgeNo ratings yet
- PPI Role in Gastroesophageal Reflux Disease Management Focus on EsomeprazoleDocument26 pagesPPI Role in Gastroesophageal Reflux Disease Management Focus on Esomeprazoledwi nugroho prastowoNo ratings yet
- GERD - PPT 11Document30 pagesGERD - PPT 11pharmaguy111No ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- Gastrointestinal Surgery 2021Document80 pagesGastrointestinal Surgery 2021Esraa SalemNo ratings yet
- Pemicu 1 GITDocument13 pagesPemicu 1 GITEric RicardoNo ratings yet
- Acid Reflux Disease: Causes, Symptoms and TreatmentDocument37 pagesAcid Reflux Disease: Causes, Symptoms and TreatmentMahad Maxamed AxmedNo ratings yet
- K-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUDocument38 pagesK-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUChristian Lumban GaolNo ratings yet
- GERD Definition, Patho and TreatmentDocument7 pagesGERD Definition, Patho and TreatmentGeethika GummadiNo ratings yet
- GERDDocument24 pagesGERDBEVERLY JANE COPADANo ratings yet
- Centers of GastroenterologyDocument8 pagesCenters of GastroenterologyLia Mbag LiaNo ratings yet
- Gastro-Esophageal Reflux Disease ( GERD)Document31 pagesGastro-Esophageal Reflux Disease ( GERD)Malueth AnguiNo ratings yet
- Pediatric Gastroesophageal RefluxDocument31 pagesPediatric Gastroesophageal RefluxAbdallahMousaNo ratings yet
- Chapter 13. Heartburn and DyspepsiaDocument22 pagesChapter 13. Heartburn and DyspepsiaMonica CiorneiNo ratings yet
- Gastroesophageal Reflux (GERD) : Prepared By/ Eman Abdelmobdy AliDocument12 pagesGastroesophageal Reflux (GERD) : Prepared By/ Eman Abdelmobdy AliMahmoud Abdel MoneimNo ratings yet
- Dysphagia: Dr. Sangeeta Aggarwal Assistant Professor, E.N.T Deptt GMCH, PatialaDocument29 pagesDysphagia: Dr. Sangeeta Aggarwal Assistant Professor, E.N.T Deptt GMCH, PatialaVishalNo ratings yet
- Gastroesophageal Reflux Disease: L. V. Borisova Docent., Ph. DDocument32 pagesGastroesophageal Reflux Disease: L. V. Borisova Docent., Ph. DSalma Mohamed RezkNo ratings yet
- GerdDocument51 pagesGerdHoney LaxNo ratings yet
- Hrkansh NotesDocument424 pagesHrkansh NotesAhmed RagabNo ratings yet
- Esophageal Disorder Part IIDocument27 pagesEsophageal Disorder Part IIJuma AwarNo ratings yet
- 4 U1.0 B978 1 4160 6189 2..00012 3..DOCPDFDocument9 pages4 U1.0 B978 1 4160 6189 2..00012 3..DOCPDFJuan HernandezNo ratings yet
- Signs and Symptoms: AdultsDocument15 pagesSigns and Symptoms: AdultsHelen McClintock100% (1)
- Alterations in Nutrition and GastrointestinalDocument7 pagesAlterations in Nutrition and GastrointestinalChriszanie CruzNo ratings yet
- Esophagitis Symptoms, Causes and TreatmentDocument26 pagesEsophagitis Symptoms, Causes and TreatmentBiway RegalaNo ratings yet
- Esophageal StrictureDocument6 pagesEsophageal StrictureŽäíñäb ÄljaÑabìNo ratings yet
- Gerd PDFDocument51 pagesGerd PDFmonir61No ratings yet
- GERD and Hiatal Hernia GuideDocument4 pagesGERD and Hiatal Hernia GuideAmoroso, Marian Corneth D.No ratings yet
- GERD SchwartzDocument10 pagesGERD SchwartzMina Tharwat AzerNo ratings yet
- 5a.ESOPHAGEAL DISORDERSDocument16 pages5a.ESOPHAGEAL DISORDERSHayat AL AKOUMNo ratings yet
- EsophagusDocument49 pagesEsophagusVivek ChauhanNo ratings yet
- Acid Peptic Disorder and GerdDocument52 pagesAcid Peptic Disorder and GerdEbuka AniNo ratings yet
- 5-Esophageal Diseases: Hugh K. Duckworth M.DDocument5 pages5-Esophageal Diseases: Hugh K. Duckworth M.DJames FlanneryNo ratings yet
- Esophagous Stomach Small Intestine PathologyDocument58 pagesEsophagous Stomach Small Intestine PathologytahaNo ratings yet
- Esophagitis Causes, Stages, TreatmentsDocument17 pagesEsophagitis Causes, Stages, Treatmentssafia ahmedNo ratings yet
- 1 Manuscript GerdDocument5 pages1 Manuscript Gerdkint manlangitNo ratings yet
- Theodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDocument7 pagesTheodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDaniel AdityaNo ratings yet
- Gastroesophageal Reflux DiseaseDocument15 pagesGastroesophageal Reflux DiseaseKenneth UbaldeNo ratings yet
- K11 Bedah EsofagusDocument37 pagesK11 Bedah EsofagusenriNo ratings yet
- Gastroesophageal RefluxDocument20 pagesGastroesophageal Refluxtofan widyaNo ratings yet
- Disease of Esophagus and Hiatal HerniaDocument76 pagesDisease of Esophagus and Hiatal HerniaSiriporn PongpattarapakNo ratings yet
- Acid Peptic Disease: Causes, Symptoms and TreatmentDocument14 pagesAcid Peptic Disease: Causes, Symptoms and TreatmentsalmanhabeebekNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Sterotex SheetDocument2 pagesSterotex SheetHemant DangarNo ratings yet
- Optex Vibro DatasheetDocument2 pagesOptex Vibro DatasheetGabriel ChiriacNo ratings yet
- Auto DFDocument14 pagesAuto DFLutfi Akun1No ratings yet
- AICTE NoticeDocument1 pageAICTE NoticeThe WireNo ratings yet
- UI UX Research DesignDocument7 pagesUI UX Research DesignSomya ShrivastavaNo ratings yet
- Ivent201 - Manual de Usuario (220-290)Document71 pagesIvent201 - Manual de Usuario (220-290)Wilber AleluyaNo ratings yet
- 2016 Students ch04 - Lovelock - Developing Service Products - 6e - STUDENTDocument36 pages2016 Students ch04 - Lovelock - Developing Service Products - 6e - STUDENTbold onyxNo ratings yet
- Input Tax Credit (TC)Document128 pagesInput Tax Credit (TC)Sidhant GoyalNo ratings yet
- IPUMS CPS Exercise 2 For RDocument7 pagesIPUMS CPS Exercise 2 For RKateO838No ratings yet
- Ha16 18PXDocument2 pagesHa16 18PXStefce PetrovNo ratings yet
- Esp Module 4Document34 pagesEsp Module 4ELLEN B.SINAHONNo ratings yet
- Ryanair Strategic AnalysisDocument36 pagesRyanair Strategic AnalysisAlmas Uddin100% (1)
- Evolution of Arbitration in IndiaDocument8 pagesEvolution of Arbitration in IndiaPururaj AggarwalNo ratings yet
- PPM Advance Android Application - User ManualDocument22 pagesPPM Advance Android Application - User ManualmayckerNo ratings yet
- Tekla - DocumentDocument2,005 pagesTekla - DocumentTranタオNo ratings yet
- PDF Vertical Axis Wind Turbines DDDocument38 pagesPDF Vertical Axis Wind Turbines DDKunal AhiwaleNo ratings yet
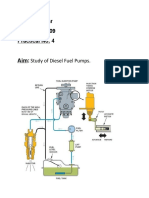
- Study of Diesel Fuel Pumps ComponentsDocument6 pagesStudy of Diesel Fuel Pumps ComponentsPro GamerssNo ratings yet
- Stolle Cupping Systems: ConnectingDocument2 pagesStolle Cupping Systems: ConnectingHieu NguyenNo ratings yet
- Token Economics BookDocument81 pagesToken Economics BookNara E Aí100% (3)
- Magnetic Particle TestDocument4 pagesMagnetic Particle TestHarry Doble100% (1)
- Plaintiff's Original Petition: Uber Ridesharing DefendantDocument8 pagesPlaintiff's Original Petition: Uber Ridesharing DefendantWigingtonRumleyDunnBlairLLPNo ratings yet
- Remote Environment: - Concern The Nature and Direction of Economy in Which A Firm Operates - Types of FactorsDocument27 pagesRemote Environment: - Concern The Nature and Direction of Economy in Which A Firm Operates - Types of FactorsmikiyingNo ratings yet
- Plan Test Strategy for Flight Search WebsiteDocument13 pagesPlan Test Strategy for Flight Search WebsiteНаталья ПримаNo ratings yet
- +1 TM Slow Learner Material For Reduced Portion 2021-22Document55 pages+1 TM Slow Learner Material For Reduced Portion 2021-22Prasanth Prasanth100% (2)
- Modeling Drop Structures in HEC-RAS 3.1Document29 pagesModeling Drop Structures in HEC-RAS 3.1reluNo ratings yet
- Tall VarietiesDocument23 pagesTall VarietiessakthivelNo ratings yet
- Bulk PricesDocument2 pagesBulk PricesMega Byte0% (1)
- Discover Haxeflixel FullDocument182 pagesDiscover Haxeflixel FullKristian Macanga100% (3)
- PFRS SGV PDFDocument18 pagesPFRS SGV PDFJonathan Javier GajeNo ratings yet
- Intelligent Platform Management Bus Communications Protocol Specification v1.0Document43 pagesIntelligent Platform Management Bus Communications Protocol Specification v1.0alexchuahNo ratings yet