You might also like
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19From EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19Rating: 3 out of 5 stars3/5 (1)
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory PerspectiveFrom EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory PerspectiveNo ratings yet
- Jurnal 2Document7 pagesJurnal 2zarazobellaNo ratings yet
- VAP Incidence, Risk Factors and Bacteria in PICUDocument6 pagesVAP Incidence, Risk Factors and Bacteria in PICURabiatul 'raney' AdawiyahNo ratings yet
- Intensified Short Symptom Screening Program For Dengue Infection During Pregnancy, IndiaDocument6 pagesIntensified Short Symptom Screening Program For Dengue Infection During Pregnancy, IndiaJose Luis RChNo ratings yet
- 90532100Document5 pages90532100Devi PuspasariNo ratings yet
- Ppe 14Document11 pagesPpe 14Sajin AlexanderNo ratings yet
- Incidence of Community Acquired Pneumonia in Children Aged 2-59 Months of Age in Uttar Pradesh and Bihar, India, in 2016: An Indirect EstimationDocument12 pagesIncidence of Community Acquired Pneumonia in Children Aged 2-59 Months of Age in Uttar Pradesh and Bihar, India, in 2016: An Indirect Estimationamenamalik484No ratings yet
- Breakthrough Infection After Covishield COVID-19 Vaccine Among Health Care Workers at Patan Academy of Health Sciences, NepalDocument8 pagesBreakthrough Infection After Covishield COVID-19 Vaccine Among Health Care Workers at Patan Academy of Health Sciences, Nepaljay n shahNo ratings yet
- Role of Procalcitonin in Diagnosis of Community Acquired Pneumonia in ChildrenDocument9 pagesRole of Procalcitonin in Diagnosis of Community Acquired Pneumonia in ChildrenYasminNo ratings yet
- Impact of Rotavirus Vaccine Introduction in Abidjan Côte D'ivoireDocument4 pagesImpact of Rotavirus Vaccine Introduction in Abidjan Côte D'ivoireArmel BheratNo ratings yet
- 2174 8646 1 PBDocument5 pages2174 8646 1 PBKiran PantheeNo ratings yet
- Predicting Outcome in Neonates With Possible Clinical Sepsis by Estimating An Early Score For Neonatal Acute Physiology-II (SNAP-II)Document8 pagesPredicting Outcome in Neonates With Possible Clinical Sepsis by Estimating An Early Score For Neonatal Acute Physiology-II (SNAP-II)ida ayu agung WijayantiNo ratings yet
- The Examination of Sleep Quality For FroDocument9 pagesThe Examination of Sleep Quality For FrowalkensiocsNo ratings yet
- Irv 12867Document10 pagesIrv 12867Ihsan fahrojiNo ratings yet
- Contoh Tesis NMJ 56 287Document5 pagesContoh Tesis NMJ 56 287Lidwina ElisabethNo ratings yet
- 2022 Risk Assessment Tool To Identify Children Aged 2-59 Months Risk For Death From CAPDocument12 pages2022 Risk Assessment Tool To Identify Children Aged 2-59 Months Risk For Death From CAPOlga CîrsteaNo ratings yet
- Prevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalDocument6 pagesPrevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalnabilahbilqisNo ratings yet
- Ugandan Pregnant and New Mothers' Perceptions, Knowledge, and Information Sources On COVID-19 at Jinja Regional Referral HospitalDocument11 pagesUgandan Pregnant and New Mothers' Perceptions, Knowledge, and Information Sources On COVID-19 at Jinja Regional Referral HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- 34030Document6 pages34030KabirNo ratings yet
- Application of Different Scoring Systems and Their Value in Pediatric Intensive Care UnitDocument6 pagesApplication of Different Scoring Systems and Their Value in Pediatric Intensive Care UnitPreksha AdeNo ratings yet
- Perinatal COVID-19: Review of Current Evidence and Practical Approach Towards Prevention and ManagementDocument23 pagesPerinatal COVID-19: Review of Current Evidence and Practical Approach Towards Prevention and ManagementDra Sandra VèlezNo ratings yet
- 1921 7826 3 PBDocument9 pages1921 7826 3 PBLeilybadryaNo ratings yet
- Paediatrica Indonesiana: Muhammad Aulia, Silvia Triratna, Yulia Iriani, Achirul Bakri, Indra SaputraDocument7 pagesPaediatrica Indonesiana: Muhammad Aulia, Silvia Triratna, Yulia Iriani, Achirul Bakri, Indra Saputrachartreuse avonleaNo ratings yet
- A Sham Case-Control Study of Effectiveness of DTP-Hib-hepatitis B Vaccine Against Rotavirus Acute Gastroenteritis in KenyaDocument10 pagesA Sham Case-Control Study of Effectiveness of DTP-Hib-hepatitis B Vaccine Against Rotavirus Acute Gastroenteritis in KenyaWinny AndarillaNo ratings yet
- Management of febrile children in Bangladesh using WHO/UNICEF IMCI guidelinesDocument10 pagesManagement of febrile children in Bangladesh using WHO/UNICEF IMCI guidelinesAung_Pyae_Phyo_4766No ratings yet
- Research Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal SepsisDocument7 pagesResearch Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal Sepsisflorentina lulutNo ratings yet
- Bordetella Pertussis in Sporadic and Outbreak Settings in Alberta, Canada, July 2004 - December 2012Document9 pagesBordetella Pertussis in Sporadic and Outbreak Settings in Alberta, Canada, July 2004 - December 2012Kambang SariadjiNo ratings yet
- Jurnal 1Document8 pagesJurnal 1aziskarnNo ratings yet
- Serological Testing Prior To Dengue Vaccine AdministrationDocument8 pagesSerological Testing Prior To Dengue Vaccine AdministrationJemimah BureresNo ratings yet
- 2016 Article 1849 PDFDocument8 pages2016 Article 1849 PDFdydy_7193No ratings yet
- Tazinya 2018Document8 pagesTazinya 2018Risnawati PurbaNo ratings yet
- Multicentric surveillance of pertussis among hospitalised infants in IndiaDocument11 pagesMulticentric surveillance of pertussis among hospitalised infants in IndiaOleOhhNo ratings yet
- Covid MortalityDocument9 pagesCovid MortalityRessa Novita AfandiNo ratings yet
- Neonatal Pneumonia Incidence and Outcomes in BangladeshDocument6 pagesNeonatal Pneumonia Incidence and Outcomes in BangladeshAnonymous Us5v7C6QhNo ratings yet
- Adverse Events Following Immunization With Pentavalent Vaccine: Experiences of Newly Introduced Vaccine in IranDocument7 pagesAdverse Events Following Immunization With Pentavalent Vaccine: Experiences of Newly Introduced Vaccine in IranAnis PurbaningrumNo ratings yet
- Infants Hospitalized For Bordetella Pertussis Infection Commonly Have Respiratory Viral CoinfectionsDocument6 pagesInfants Hospitalized For Bordetella Pertussis Infection Commonly Have Respiratory Viral CoinfectionsYuscha AnindyaNo ratings yet
- PDFDocument9 pagesPDFsatriobudi_wicaksonoNo ratings yet
- Epidemiology and Clinical Profile of PIMS-TS. Dhanalakshmi Ind Pediatr Aug 2020Document10 pagesEpidemiology and Clinical Profile of PIMS-TS. Dhanalakshmi Ind Pediatr Aug 2020Bala RamachandranNo ratings yet
- 307 974 1 PBDocument8 pages307 974 1 PBRifdah AmalinaNo ratings yet
- Apid 8 2 98735Document5 pagesApid 8 2 98735ko naythweNo ratings yet
- Development of A Scale For Early Prediction of Refractory Mycoplasma Pneumoniae Pneumonia in Hospitalized ChildrenDocument8 pagesDevelopment of A Scale For Early Prediction of Refractory Mycoplasma Pneumoniae Pneumonia in Hospitalized Childrenthanhhien900No ratings yet
- Review ArticleDocument8 pagesReview ArticleIdmNo ratings yet
- Prognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyDocument6 pagesPrognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2854-Article Text-13072-1-10-20230428Document8 pages2854-Article Text-13072-1-10-20230428jdjhdNo ratings yet
- Ultrasound Predicts Severe Dengue in ChildrenDocument5 pagesUltrasound Predicts Severe Dengue in Childrenhappy gummyNo ratings yet
- A Study To Estimate The Coverage of Measles Rubella Vaccination Campaign and Various Reasons For Non-Immunization: An Observational StudyDocument3 pagesA Study To Estimate The Coverage of Measles Rubella Vaccination Campaign and Various Reasons For Non-Immunization: An Observational StudyAVINASH NNo ratings yet
- 2017 Debnath Improved Timeliness For Reporting of Acute Diarrhoeal Disease Under SurveillanceDocument5 pages2017 Debnath Improved Timeliness For Reporting of Acute Diarrhoeal Disease Under SurveillanceKiran KumbharNo ratings yet
- LSWKQDocument9 pagesLSWKQSoniJfreeNo ratings yet
- PSSJN - Volume 1 - Issue 2 - Pages 265-280Document16 pagesPSSJN - Volume 1 - Issue 2 - Pages 265-280Praveen YadavNo ratings yet
- A Comparative-Descriptive Analysis of Clinical Characteristics in 2019-Coronavirus-Infected Children and AdultsDocument28 pagesA Comparative-Descriptive Analysis of Clinical Characteristics in 2019-Coronavirus-Infected Children and AdultsPatrick NunsioNo ratings yet
- Journal Pone 0254580Document10 pagesJournal Pone 0254580tifanny carolinaNo ratings yet
- Dokumen PDFDocument5 pagesDokumen PDFMacchiatoNo ratings yet
- Jurnal 2Document10 pagesJurnal 2GFORCE .ID.No ratings yet
- Relationship Between High Sensitivity-C Reactive PDocument7 pagesRelationship Between High Sensitivity-C Reactive PsucremeNo ratings yet
- Pneumonia Severity Index in Viral Community Acquired Pneumonia in AdultsDocument12 pagesPneumonia Severity Index in Viral Community Acquired Pneumonia in Adultsmuhammad_ariefNo ratings yet
- Hooli 2016Document13 pagesHooli 2016Arya Prajna WicaksonoNo ratings yet
- 00006565-900000000-97323Document5 pages00006565-900000000-97323aldo saadot garcia ortizNo ratings yet
- JCP 10 3 85983Document6 pagesJCP 10 3 85983Davit SoesantoNo ratings yet
- Real Issues for COVID-19 Vaccine Immunization & Pregnancy, Breastfeeding MothersFrom EverandReal Issues for COVID-19 Vaccine Immunization & Pregnancy, Breastfeeding MothersNo ratings yet
- 2023 EAACI - Guidelines - Diagnosis - IgE-mediated - Food - AllergyDocument56 pages2023 EAACI - Guidelines - Diagnosis - IgE-mediated - Food - AllergyOlga CîrsteaNo ratings yet
- 2022 Risk Assessment Tool To Identify Children Aged 2-59 Months Risk For Death From CAPDocument12 pages2022 Risk Assessment Tool To Identify Children Aged 2-59 Months Risk For Death From CAPOlga CîrsteaNo ratings yet
- 1.2c UNICEF Health and Nutrition StrategyDocument23 pages1.2c UNICEF Health and Nutrition StrategyOlga CîrsteaNo ratings yet
- 2020 Assessment of Missed Opportunities For Vaccination in Burkina Faso Using The WHO Revised MOV StrategyDocument21 pages2020 Assessment of Missed Opportunities For Vaccination in Burkina Faso Using The WHO Revised MOV StrategyOlga CîrsteaNo ratings yet
- 2022 A Retrospective Chart Review of Pediatric Complicated Community-Acquired PneumoniaDocument20 pages2022 A Retrospective Chart Review of Pediatric Complicated Community-Acquired PneumoniaOlga CîrsteaNo ratings yet
- How To Get Help For Your Child Tip Sheet FINAL 2 2020Document1 pageHow To Get Help For Your Child Tip Sheet FINAL 2 2020Olga CîrsteaNo ratings yet
- Necrotizing Pneumonia - An Emerging Problem in ChildrenDocument19 pagesNecrotizing Pneumonia - An Emerging Problem in ChildrenOlga CîrsteaNo ratings yet
- CommonCold101713 PDFDocument4 pagesCommonCold101713 PDFMohsinRazaNo ratings yet
- Rome III Diagnostic Criteria FGIDsDocument14 pagesRome III Diagnostic Criteria FGIDsPutu Reza Sandhya PratamaNo ratings yet
- Domestic-Abuse - What Health Workers Need To Know About Gender-Based ViolenceDocument28 pagesDomestic-Abuse - What Health Workers Need To Know About Gender-Based ViolenceOlga CîrsteaNo ratings yet
- Getting Children to Take Their MedicineDocument2 pagesGetting Children to Take Their MedicineOlga CîrsteaNo ratings yet
- Stein R Et Al Paediatric Infections EUR UROL 67 2015 546 558 14826Document13 pagesStein R Et Al Paediatric Infections EUR UROL 67 2015 546 558 14826Olga CîrsteaNo ratings yet
- Connecting Home Visiting and The Medical Home SlidesDocument60 pagesConnecting Home Visiting and The Medical Home SlidesOlga CîrsteaNo ratings yet
- Сhronic pancreatitis: Lykhatska G.VDocument42 pagesСhronic pancreatitis: Lykhatska G.VOlga CîrsteaNo ratings yet
- European-Core-Curriculum-for-Emergecy Medicine-Version-1.2-April-2017-final-version-1 PDFDocument41 pagesEuropean-Core-Curriculum-for-Emergecy Medicine-Version-1.2-April-2017-final-version-1 PDFOlga CîrsteaNo ratings yet
- Alimentatia Copilului - OMSDocument112 pagesAlimentatia Copilului - OMSshugyosha77No ratings yet
- Clinical Pearls in Respiratory DiseasesDocument7 pagesClinical Pearls in Respiratory DiseasesOlga CîrsteaNo ratings yet
- Risk AssessmentDocument90 pagesRisk AssessmentGinaAlexaCîmpianuNo ratings yet
- A Guide For Monitoring Child Development in Low - and Middle-Income Countries 2008Document11 pagesA Guide For Monitoring Child Development in Low - and Middle-Income Countries 2008Olga CîrsteaNo ratings yet
- Children and Young People - Scotland - Act 2014Document84 pagesChildren and Young People - Scotland - Act 2014Olga CîrsteaNo ratings yet
- 27 30 Month Visit ReportDocument2 pages27 30 Month Visit ReportOlga CîrsteaNo ratings yet
- Conversations in The Postnatal Period - Key Points - Postnatal - Signature - SheetDocument1 pageConversations in The Postnatal Period - Key Points - Postnatal - Signature - SheetOlga CîrsteaNo ratings yet
- 6-8 week assessment formDocument2 pages6-8 week assessment formOlga CîrsteaNo ratings yet
- Trainers Guide EngDocument538 pagesTrainers Guide EngOlga CîrsteaNo ratings yet
- Health Professionals Guide To Coping at NightDocument19 pagesHealth Professionals Guide To Coping at NightOlga CîrsteaNo ratings yet
- Postnatal Care Up To 8 Weeks After Birth GUIDELINEDocument63 pagesPostnatal Care Up To 8 Weeks After Birth GUIDELINEOlga CîrsteaNo ratings yet
- Guidelines EngDocument96 pagesGuidelines EngOlga CîrsteaNo ratings yet
- Conversations For The Health Visiting Team: Key PointsDocument2 pagesConversations For The Health Visiting Team: Key PointsOlga CîrsteaNo ratings yet
- Red Flags GuideDocument50 pagesRed Flags GuidesolideoNo ratings yet
- Banana Flavor MSDS: Material Safety Data SheetDocument3 pagesBanana Flavor MSDS: Material Safety Data Sheetralphael obodoNo ratings yet
- (Template) BEED CHAPTER 3 MODULE 3 - Sci 1Document6 pages(Template) BEED CHAPTER 3 MODULE 3 - Sci 1Regilyn GalasNo ratings yet
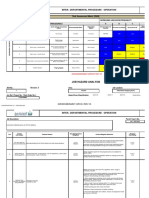
- Inter - Departmental Procedure Operation: IP-OPS-066Document10 pagesInter - Departmental Procedure Operation: IP-OPS-066AnuradheNo ratings yet
- Catalog: Product and SolutionsDocument84 pagesCatalog: Product and SolutionsAnonymous w4ZnisPlazNo ratings yet
- Funda DemoDocument10 pagesFunda DemoariadnebabasaNo ratings yet
- 3M Particulate Respirator 8210, N95: Key FeaturesDocument3 pages3M Particulate Respirator 8210, N95: Key FeaturesJohnyNo ratings yet
- Nursing Care Plan #1Document6 pagesNursing Care Plan #1Yamete KudasaiNo ratings yet
- Anaesthesia Management in Endoscopic Ultrasound Guided Lung BiopsyDocument2 pagesAnaesthesia Management in Endoscopic Ultrasound Guided Lung BiopsyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mindful Breathing MeditationDocument3 pagesMindful Breathing MeditationHannah Johana Basadre TambanilloNo ratings yet
- Ibps Po-Xi Prelims Mt-94: Sreedhar'sDocument12 pagesIbps Po-Xi Prelims Mt-94: Sreedhar'sMaheshNo ratings yet
- Material Safety Data Sheet (MSDS)Document2 pagesMaterial Safety Data Sheet (MSDS)Krlos LunaNo ratings yet
- Management of Patient-Ventilator Asynchrony: Clinical Focus ReviewDocument8 pagesManagement of Patient-Ventilator Asynchrony: Clinical Focus ReviewResidentes HomiNo ratings yet
- MSDS Rheflat PlusDocument6 pagesMSDS Rheflat PlusJose AlejandroBlancoNo ratings yet
- 1600 - Friday - PFT and CPET Case Studies - Marciniuk PDFDocument64 pages1600 - Friday - PFT and CPET Case Studies - Marciniuk PDFtechang1No ratings yet
- Laporan Kasus BronkopneumoniaDocument30 pagesLaporan Kasus BronkopneumoniaShifa Ali JannatinNo ratings yet
- Spo2 Sensor: Working PrincipleDocument17 pagesSpo2 Sensor: Working PrincipleSudarshan KanseNo ratings yet
- 2017 Dur A Gard Esd Submittal Package 170804Document35 pages2017 Dur A Gard Esd Submittal Package 170804Boy BangusNo ratings yet
- MSDS BitacrylDocument4 pagesMSDS Bitacryledi100% (1)
- CopdandexerciseDocument11 pagesCopdandexerciseapi-663023028No ratings yet
- 7.4 Gas Exchange in Plants and Animals 2Document3 pages7.4 Gas Exchange in Plants and Animals 2yiuzz hcyNo ratings yet
- BasicsDocument87 pagesBasicsمصطفى فؤاد عمران داودNo ratings yet
- Weaning Oxygen in Infants With Bronchopulmonary DysplasiaDocument26 pagesWeaning Oxygen in Infants With Bronchopulmonary DysplasiaJHONATAN MATA ARANDANo ratings yet
- 1359 Eng PDFDocument1 page1359 Eng PDFHaleem Ur Rashid BangashNo ratings yet
- Pneumonia PamphletDocument2 pagesPneumonia PamphletMairiz Jem Santos100% (6)
- Exam # Respiratory Study Blueprint 2019Document2 pagesExam # Respiratory Study Blueprint 2019Stephanie DeeNo ratings yet
- Biology As/A Level Classwork: Submitted By: Kannita Sipaseuth (Jane)Document5 pagesBiology As/A Level Classwork: Submitted By: Kannita Sipaseuth (Jane)Kannita SIPASEUTHNo ratings yet
- QUESTIONAIRE Research Final PDFDocument2 pagesQUESTIONAIRE Research Final PDFAli AfaqNo ratings yet
- Benefits of RelaxationDocument2 pagesBenefits of RelaxationDina MossaadNo ratings yet
- Rat DissectionDocument9 pagesRat Dissectionapi-296981910No ratings yet
- COVID-19 Contingency Plan for Bambad NHSDocument4 pagesCOVID-19 Contingency Plan for Bambad NHSGLENN QUIBUYEN100% (1)