You might also like
- Head To Toe Patient AssessmentDocument2 pagesHead To Toe Patient AssessmentJaypee Nuñez100% (2)
- Waves That Heal (Mark Clement)Document62 pagesWaves That Heal (Mark Clement)THE NIKOLA TESLA INSTITUTE100% (6)
- The ORGONE ENERGY ACCUMULATOR in Treating Cancer in MiceDocument8 pagesThe ORGONE ENERGY ACCUMULATOR in Treating Cancer in MiceCambiador de MundoNo ratings yet
- Light Therapy in Mental Hospitals: 1929, 75:410-419. H. Dove CormacDocument11 pagesLight Therapy in Mental Hospitals: 1929, 75:410-419. H. Dove CormacAreesha AhmadNo ratings yet
- 1866 Lee Animal Magnetism and Magnet Lucid SomnambulismDocument354 pages1866 Lee Animal Magnetism and Magnet Lucid SomnambulismtvosNo ratings yet
- Naval Aviation News - Apr 1950Document44 pagesNaval Aviation News - Apr 1950CAP History LibraryNo ratings yet
- Lakhovsky Waves That HealsDocument30 pagesLakhovsky Waves That Healsplan2222100% (2)
- Russell, Bertrand - ABC of Atoms (Dutton, 1923) PDFDocument171 pagesRussell, Bertrand - ABC of Atoms (Dutton, 1923) PDFGerardo HerculesNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
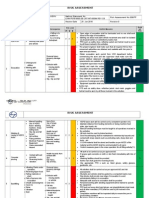
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Extreme Survival: A Serious Technical Diving Accident: March 2005Document6 pagesExtreme Survival: A Serious Technical Diving Accident: March 2005worefdNo ratings yet
- DocumentDocument12 pagesDocumentJon Saiman0% (1)
- 4.schedule Waste Management UTM - SWMP - 22mei2018 PDFDocument54 pages4.schedule Waste Management UTM - SWMP - 22mei2018 PDFfaraNo ratings yet
- Can Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.Document15 pagesCan Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.ALIXNo ratings yet
- Professional Growth and DevelopmentDocument154 pagesProfessional Growth and DevelopmentNina Anne Paracad100% (3)
- Tung DocumentreviewDocument8 pagesTung DocumentreviewRodrigo Bittencourt100% (3)
- SpitzDocument30 pagesSpitzprabhatNo ratings yet
- Fermentation - How Antibiotics Are Produced by Fermentation TechnologyDocument12 pagesFermentation - How Antibiotics Are Produced by Fermentation TechnologyArfia Chowdhury Arifa88% (57)
- Human Skin Blood VesselsDocument2 pagesHuman Skin Blood VesselsВладимир ДружининNo ratings yet
- Wesener 1897Document2 pagesWesener 1897Illuminate ValorantNo ratings yet
- 2425-Article Text-7181-1-10-20141208Document4 pages2425-Article Text-7181-1-10-20141208Patricia Anne Nicole CuaresmaNo ratings yet
- Lymphocyte-A Disgraceful Gap in Medical KnowledgeDocument4 pagesLymphocyte-A Disgraceful Gap in Medical KnowledgeSuvas_Patel_2902No ratings yet
- Smith 1958Document5 pagesSmith 1958AmoNo ratings yet
- Early History and Development of MicrobiologyDocument10 pagesEarly History and Development of MicrobiologyMR. MISHRANo ratings yet
- Cadmium Chloride Aerosol Induces Rat Lung EmphysemaDocument9 pagesCadmium Chloride Aerosol Induces Rat Lung EmphysemaPercy SolisNo ratings yet
- Causes of Death from High Intestinal ObstructionDocument20 pagesCauses of Death from High Intestinal ObstructionGrecu IgorNo ratings yet
- Physics,: ConceptionDocument8 pagesPhysics,: ConceptionShem Peter Mutua MutuiriNo ratings yet
- Canmedaj00659 0028Document3 pagesCanmedaj00659 0028Joana TavaresNo ratings yet
- English Reading Skill, Determine The Main Idea of A PassageDocument11 pagesEnglish Reading Skill, Determine The Main Idea of A PassageLeonsius100% (1)
- Haemoglobin and altitude: the body's response to hypoxiaDocument4 pagesHaemoglobin and altitude: the body's response to hypoxiamuhamad isafarudinNo ratings yet
- Metaphysical ArchitectureDocument11 pagesMetaphysical ArchitectureIdaHodzicNo ratings yet
- 23-26 An Autopsy Case of Decompression Sickness. Hemorrhages in The Fat Tissue and Fat EmbolismDocument4 pages23-26 An Autopsy Case of Decompression Sickness. Hemorrhages in The Fat Tissue and Fat EmbolismLoredana MorosanuNo ratings yet
- Introduction of Tracheal Tubes by The Mouth Instead of Performing Tracheotomy or Laryngotomy.Document3 pagesIntroduction of Tracheal Tubes by The Mouth Instead of Performing Tracheotomy or Laryngotomy.Pablo PradoNo ratings yet
- Copen Radiation Rectifier Schematic, & OranurDocument6 pagesCopen Radiation Rectifier Schematic, & Oranurgpevicky007No ratings yet
- Gofman 2Document4 pagesGofman 2RobertoNo ratings yet
- A History of Science Volume 4Document127 pagesA History of Science Volume 4bunnywidgeNo ratings yet
- Dixon A Preliminary Note On The Pharmacology of The Alkaloids Derived From The Mescal PlantDocument2 pagesDixon A Preliminary Note On The Pharmacology of The Alkaloids Derived From The Mescal PlantpiniedduNo ratings yet
- A Case Report - Surgical Relief of Colic in An EquineDocument4 pagesA Case Report - Surgical Relief of Colic in An Equinelinda nugrohoNo ratings yet
- False Evidence of Evolution - 2: The Miller ExperimentDocument10 pagesFalse Evidence of Evolution - 2: The Miller ExperimentHarunyahya EnglishNo ratings yet
- Jama 1898 72440590004001aDocument5 pagesJama 1898 72440590004001aNilsonMarianoFilhoNo ratings yet
- Chernobyl CatastropheDocument6 pagesChernobyl Catastrophealondra martinezNo ratings yet
- CHERNOBYL DISASTER EXPLAINEDDocument6 pagesCHERNOBYL DISASTER EXPLAINEDalondra martinezNo ratings yet
- Chernobyl Catastrophe: Oscar Oswaldo Cardiel MoralesDocument6 pagesChernobyl Catastrophe: Oscar Oswaldo Cardiel Moralesalondra martinezNo ratings yet
- Chernobyl CatastropheDocument6 pagesChernobyl Catastrophealondra martinezNo ratings yet
- A History of Science (Volume 4)Document311 pagesA History of Science (Volume 4)simona robuNo ratings yet
- Chloroform For The KingDocument7 pagesChloroform For The Kingapi-184836296No ratings yet
- jphysiol02608-0001Document25 pagesjphysiol02608-0001Sonia PujalsNo ratings yet
- The History of Chlorine Discovery and Growth as a Chemical CommodityDocument14 pagesThe History of Chlorine Discovery and Growth as a Chemical CommodityСаня СкорикNo ratings yet
- Scientific Evidence of Pre-Columbian Syphilis Remains UnprovenDocument4 pagesScientific Evidence of Pre-Columbian Syphilis Remains UnprovenLâm NguyễnNo ratings yet
- Acute Pancreatitis Diagnosis ChallengesDocument2 pagesAcute Pancreatitis Diagnosis ChallengesdyahyektiindrajatiNo ratings yet
- (2010) The History of CapnographyDocument1 page(2010) The History of CapnographyDominik Chirito PastorNo ratings yet
- Chloroform in Clinical Anaesthesia: Br. Anaesth. (1981), 53, lISDocument5 pagesChloroform in Clinical Anaesthesia: Br. Anaesth. (1981), 53, lISAlinNo ratings yet
- Historia de La MH Ii2007Document20 pagesHistoria de La MH Ii2007Carolina CortezNo ratings yet
- Sudden Death and HopeDocument8 pagesSudden Death and HopemanowarNo ratings yet
- Nthralvt!ot .. C Ca, Al' (: Membri/"LDocument13 pagesNthralvt!ot .. C Ca, Al' (: Membri/"LSanikaNo ratings yet
- Canmedaj00449 0102 1Document2 pagesCanmedaj00449 0102 1siti aisyahNo ratings yet
- CaissonDocument68 pagesCaissonBudi SantosaNo ratings yet
- Annals of Surgery: DecemberDocument9 pagesAnnals of Surgery: DecemberJkn PekalonganNo ratings yet
- Bancroft W. D. - Claude Bernard's Theory of Narcosis (1930)Document6 pagesBancroft W. D. - Claude Bernard's Theory of Narcosis (1930)Anonymous OFQuRiZOUzNo ratings yet
- The Study of The Very SmallDocument5 pagesThe Study of The Very Smalll_boyd_clowesNo ratings yet
- Nature:: Influenza and Ozone Science Following H. P. Blavatsky'S Lead: by H. T. EdgeDocument71 pagesNature:: Influenza and Ozone Science Following H. P. Blavatsky'S Lead: by H. T. EdgeOcultura BRNo ratings yet
- Cupping: A prophetical medicine appears in its new scientific perspectiveFrom EverandCupping: A prophetical medicine appears in its new scientific perspectiveNo ratings yet
- Siftings V3 A15Document12 pagesSiftings V3 A15OlympiaNo ratings yet
- Cellular BiologyDocument132 pagesCellular BiologyunigeNo ratings yet
- Lieb Goiter and Involuntary Nervous System 13 1922Document3 pagesLieb Goiter and Involuntary Nervous System 13 1922IGNo ratings yet
- SH Erring Ton J Physiol (Lond) 1891Document8 pagesSH Erring Ton J Physiol (Lond) 1891Samit ChakrabartyNo ratings yet
- SonoluminescenceDocument17 pagesSonoluminescenceJesús Tenorio QuevedoNo ratings yet
- Week 15 - ONCO COURSE TASK - Breast Cancer DetectionDocument3 pagesWeek 15 - ONCO COURSE TASK - Breast Cancer DetectionGelo AlonzoNo ratings yet
- OBG ChapterDocument3 pagesOBG ChapterMohd IrfanNo ratings yet
- 2023 AHAR: PIT Estimates of Homelessness in The U.S.Document117 pages2023 AHAR: PIT Estimates of Homelessness in The U.S.Santiago Adolfo OspitalNo ratings yet
- Introduction To The Alpaca andDocument9 pagesIntroduction To The Alpaca andMai Chi PhạmNo ratings yet
- 8 RA 4688 (Clinical Laboratory Law)Document32 pages8 RA 4688 (Clinical Laboratory Law)AIRRA CLAIRE ALVAREZNo ratings yet
- Hospital Self Assement ToolkitDocument28 pagesHospital Self Assement ToolkitNidhi VijanNo ratings yet
- Ethics of Blood TransfusionDocument6 pagesEthics of Blood TransfusionHo Yong WaiNo ratings yet
- Clinical Immunology and AllergyDocument156 pagesClinical Immunology and AllergySoleil DaddouNo ratings yet
- Concussionspaper 1Document6 pagesConcussionspaper 1api-350027909No ratings yet
- 3075 SWMS RendererDocument13 pages3075 SWMS Renderernik KooNo ratings yet
- Otto Chemie PVT LTD: Material Safety Data SheetDocument4 pagesOtto Chemie PVT LTD: Material Safety Data Sheetenes duhanNo ratings yet
- Assist LetterDocument2 pagesAssist Lettertashy richardsNo ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- Maynilad Valenzuela Sewerage Project Environmental ReportDocument297 pagesMaynilad Valenzuela Sewerage Project Environmental ReportmarvilouNo ratings yet
- Autoimmune HepatitisDocument3 pagesAutoimmune HepatitisMohammed FaragNo ratings yet
- Rock Solid Immunity, Naturally - by Rajeev Agarwal R3Document5 pagesRock Solid Immunity, Naturally - by Rajeev Agarwal R3Rajeev B AgarwalNo ratings yet
- 2020 Corportate Sustainability ReportDocument22 pages2020 Corportate Sustainability ReportMohamed KannouNo ratings yet
- CYBERBULLYINGDocument2 pagesCYBERBULLYINGAdinda CahayaNo ratings yet
- POne MPFFL 7 RV VPSX LQRPDocument3 pagesPOne MPFFL 7 RV VPSX LQRPRavi KumarNo ratings yet
- UG MaharashtraNationalLawUniversityMNLUMumbaiDocument5 pagesUG MaharashtraNationalLawUniversityMNLUMumbaiArpan KushwahaNo ratings yet