You might also like
- Production Book Template 1Document38 pagesProduction Book Template 1Ria Nicole78% (9)
- NounsDocument13 pagesNounsapi-242894068100% (1)
- Basics of Orthopedic RadiologyDocument94 pagesBasics of Orthopedic RadiologyandreNo ratings yet
- TemporoMandibular Joint SEMINAR NiviDocument173 pagesTemporoMandibular Joint SEMINAR Nivinivethasesha100% (1)
- D CONSTITUTIONAL LAW The Philippines As A StateDocument13 pagesD CONSTITUTIONAL LAW The Philippines As A StateSunjeong Macho100% (1)
- Semilunar Coronally Repositioned FlapDocument5 pagesSemilunar Coronally Repositioned FlapTarun Kumar Bhatnagar100% (1)
- The Jaw and Related StructuresDocument6 pagesThe Jaw and Related Structuresarzdar100% (1)
- Anterolateral Thigh - ALT - Free Flap For Head and Neck ReconstructionDocument12 pagesAnterolateral Thigh - ALT - Free Flap For Head and Neck ReconstructionАрман ЖуманкуловNo ratings yet
- J. R. Searle - Rationality in ActionDocument320 pagesJ. R. Searle - Rationality in ActionIva Shane80% (5)
- IT Companies in CoimbatoreDocument1 pageIT Companies in Coimbatoresureshkumarmask60% (5)
- Enraf 854 Atg Interface Application NotesDocument43 pagesEnraf 854 Atg Interface Application NotesArmando Angeles MartinezNo ratings yet
- Oseo UppDocument28 pagesOseo UppMariana Mojica DiazNo ratings yet
- Caspar I 1997Document4 pagesCaspar I 1997Sarly FebrianaNo ratings yet
- Macroanatomy and Microanatomy of The Temporal Lobe 2007Document12 pagesMacroanatomy and Microanatomy of The Temporal Lobe 2007Juan José Pabón CastroNo ratings yet
- Functional Primary Closure of The Cleft LipDocument11 pagesFunctional Primary Closure of The Cleft LipAndrés Faúndez TeránNo ratings yet
- Detailed Orbital AnatomyDocument12 pagesDetailed Orbital AnatomyMashood AhmedNo ratings yet
- OrbitDocument10 pagesOrbitayrahrahmanNo ratings yet
- Anatomy of The Elbow: Trauma and ReconstructionDocument13 pagesAnatomy of The Elbow: Trauma and ReconstructionSrinivasNo ratings yet
- Periocularanatomy Andaging: Lily P. Love,, Edward H. FarriorDocument7 pagesPeriocularanatomy Andaging: Lily P. Love,, Edward H. FarriorCamila CrosaraNo ratings yet
- AnatosuchusDocument6 pagesAnatosuchusJorge BarrientosNo ratings yet
- Ankle X-Ray InterpretationDocument9 pagesAnkle X-Ray InterpretationBeeNo ratings yet
- Anatomía Correlativa Del DiafragmaDocument7 pagesAnatomía Correlativa Del Diafragmaomar morelosNo ratings yet
- Differential Diagnoses For Disc HerniationDocument11 pagesDifferential Diagnoses For Disc HerniationZulvina FaozanudinNo ratings yet
- Maxillo Acial Prosthesis: The Maxillary Resection and Its Prosthetic ReplacementDocument14 pagesMaxillo Acial Prosthesis: The Maxillary Resection and Its Prosthetic Replacementayush srivastavaNo ratings yet
- Co Lohan 1985Document3 pagesCo Lohan 1985RathavishwarajNo ratings yet
- Chapter 3 - Uvea - 2012 - Clinical Anatomy and Physiology of The Visual SystemDocument21 pagesChapter 3 - Uvea - 2012 - Clinical Anatomy and Physiology of The Visual SystemAldo CortesNo ratings yet
- E. PH.D., F.Z.S.,: 8. Further The Myology of The Pectoral by Seakn, Onndle SchoolDocument21 pagesE. PH.D., F.Z.S.,: 8. Further The Myology of The Pectoral by Seakn, Onndle SchoolasNo ratings yet
- Auricula Orejita PDFDocument8 pagesAuricula Orejita PDFRICARDO ANDRES TOSCANO VILLAMIZARNo ratings yet
- 272.full Hallux ValgusDocument22 pages272.full Hallux ValgusAlex MoscoNo ratings yet
- Sylvian Cistern PDFDocument2 pagesSylvian Cistern PDFTiger PowerNo ratings yet
- Hypospadias and The Embryogenesis of The Penile UrethraDocument6 pagesHypospadias and The Embryogenesis of The Penile UrethraNailahRahmahNo ratings yet
- Reader in Orthopaedics, University of Glasgow: Roland BarnesDocument11 pagesReader in Orthopaedics, University of Glasgow: Roland BarnesAustine OsaweNo ratings yet
- Ten Questions On Kienbock's DiseaseDocument6 pagesTen Questions On Kienbock's DiseaseProfesseur Christian DumontierNo ratings yet
- 3 - Mendelson PREMASSETERIC SPACE 2Document10 pages3 - Mendelson PREMASSETERIC SPACE 2Diego Henrique MoreiraNo ratings yet
- Manual of Nearctic Diptera V1 McAlpine Et Al 1981 9 MorphologyDocument80 pagesManual of Nearctic Diptera V1 McAlpine Et Al 1981 9 MorphologyChristophe AvonNo ratings yet
- ALL Clinicals of Upper LimbDocument28 pagesALL Clinicals of Upper LimbБайден ТрампNo ratings yet
- Anatomy of The SkullDocument3 pagesAnatomy of The SkullYeraldin EspañaNo ratings yet
- Nomenclature and Geometric Classification of Cleavage Transected Folds-T.e. JohnsonDocument14 pagesNomenclature and Geometric Classification of Cleavage Transected Folds-T.e. JohnsonEdilberAntonyChipanaPariNo ratings yet
- Stress Fields About Strike-Slip Faults Inferred From Stylolites and Tension GashesDocument8 pagesStress Fields About Strike-Slip Faults Inferred From Stylolites and Tension Gashessanchese11No ratings yet
- Orbicular FracturesDocument81 pagesOrbicular FracturesMARISOL GALLEGO DUQUENo ratings yet
- Jexbio 27 3 264Document28 pagesJexbio 27 3 264Nikhil JohnNo ratings yet
- Oyster 2Document12 pagesOyster 2aonaran4lifeNo ratings yet
- Orbital Bony Anatomy and Orbital Fractures: GlossaryDocument9 pagesOrbital Bony Anatomy and Orbital Fractures: Glossarym29hereNo ratings yet
- Articulo DX Semana 14Document7 pagesArticulo DX Semana 14Valeria Garcia QuijanoNo ratings yet
- Smith 1957Document7 pagesSmith 1957Emanuel MartinezNo ratings yet
- Temporalis Muscle Flap-1Document5 pagesTemporalis Muscle Flap-1Mohd Rehan QureshiNo ratings yet
- Tentorial IncisuraDocument23 pagesTentorial Incisurabodeadumitru9261100% (1)
- Articulo CientificoDocument8 pagesArticulo CientificoLuis Miguel Vacacela QuizhpeNo ratings yet
- 87 - CH 3 - Summary of The Gross Anatomy of The Extra Ocular Muscles, P. 38-51Document14 pages87 - CH 3 - Summary of The Gross Anatomy of The Extra Ocular Muscles, P. 38-51imranjan81No ratings yet
- Amis 2012Document8 pagesAmis 2012abdo houamerNo ratings yet
- Managementofelbow Trauma:: Anatomy and ExposuresDocument11 pagesManagementofelbow Trauma:: Anatomy and ExposuresMishael Diaz PoncecaNo ratings yet
- Gall-Bladder,: For Exact Anatomy Concerns Does Rectus OrganDocument6 pagesGall-Bladder,: For Exact Anatomy Concerns Does Rectus OrganNcunbarNo ratings yet
- Surgical Anatomy of The Midcheek: Facial Layers, Spaces, and The Midcheek SegmentsDocument11 pagesSurgical Anatomy of The Midcheek: Facial Layers, Spaces, and The Midcheek SegmentsDavid BaramidzeNo ratings yet
- ('14) Described A Vascular Layer WhichDocument18 pages('14) Described A Vascular Layer WhichhaneefmdfNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument4 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- Triangle of Doom and Pain 1Document7 pagesTriangle of Doom and Pain 1AnantaSiddhiPrawaraNo ratings yet
- Norm Anatomy Elbow 2011Document11 pagesNorm Anatomy Elbow 2011Екатерина БербецNo ratings yet
- A Modified Judet Approach To The ScapulaDocument4 pagesA Modified Judet Approach To The ScapulaGiulio PriftiNo ratings yet
- Supracondileas NiñosDocument10 pagesSupracondileas NiñosMaría Antonia Perdomo GarciaNo ratings yet
- Fractures of Distal End of RadiusDocument25 pagesFractures of Distal End of RadiusVenkee SaiNo ratings yet
- Cordula Schmolke 1994 - The - Relationship - Between - The - Temporomandibular - Joint - Capsule, - Articular - Disc - and - Jaw - MusclesDocument11 pagesCordula Schmolke 1994 - The - Relationship - Between - The - Temporomandibular - Joint - Capsule, - Articular - Disc - and - Jaw - MusclesbélaNo ratings yet
- Surgical Technique: Posterolateral Approach For Open Reduction and Internal Fixation of Trimalleolar Ankle FracturesDocument4 pagesSurgical Technique: Posterolateral Approach For Open Reduction and Internal Fixation of Trimalleolar Ankle FracturesVictor M. GarciaNo ratings yet
- Asymmettic Space Closure: Clinicians' CornerDocument7 pagesAsymmettic Space Closure: Clinicians' CornerMonojit DuttaNo ratings yet
- Endoscopic Transorbital Surgery - Medial Orbital - Precaruncular - ApproachDocument13 pagesEndoscopic Transorbital Surgery - Medial Orbital - Precaruncular - ApproachjackelineNo ratings yet
- A New Order of Fishlike Amphibia From the Pennsylvanian of KansasFrom EverandA New Order of Fishlike Amphibia From the Pennsylvanian of KansasNo ratings yet
- Basic For Micro ComputersDocument354 pagesBasic For Micro ComputersGiovanni MercuriNo ratings yet
- The Timex Personal Computer Made SimpleDocument164 pagesThe Timex Personal Computer Made SimpleGiovanni MercuriNo ratings yet
- Blackbox PDFDocument17 pagesBlackbox PDFGiovanni MercuriNo ratings yet
- Statisticalevalu00gian PDFDocument156 pagesStatisticalevalu00gian PDFGiovanni MercuriNo ratings yet
- Digital Fundamentals: FloydDocument60 pagesDigital Fundamentals: FloydAyesha NazirNo ratings yet
- DodgeballDocument34 pagesDodgeballQiaoqian Zheng ZhengNo ratings yet
- Maintenance Alat Berat Hd785 7pdf PRDocument208 pagesMaintenance Alat Berat Hd785 7pdf PRDeni SubektiNo ratings yet
- Chapter 26 Satellite Multiple Accessing Arrangements 192 197Document6 pagesChapter 26 Satellite Multiple Accessing Arrangements 192 197raymondNo ratings yet
- BioFluid Mechanics 1Document29 pagesBioFluid Mechanics 1roxannedemaeyerNo ratings yet
- 2006 - Amc - 10 BDocument13 pages2006 - Amc - 10 BSUNGMIN CHOI100% (1)
- Lawphil: Be It Enacted by The Senate and The House of Representatives of The Philippines in Congress AssembledDocument31 pagesLawphil: Be It Enacted by The Senate and The House of Representatives of The Philippines in Congress AssembledMarie Nickie BolosNo ratings yet
- Favorskii R.A. by M.AsifDocument18 pagesFavorskii R.A. by M.AsifMUhammad AsifNo ratings yet
- NgabenDocument2 pagesNgabenrisarizkynurliaNo ratings yet
- Dasypus Novemcinctus,: Assessment By: Loughry, J., Mcdonough, C. & Abba, A.MDocument11 pagesDasypus Novemcinctus,: Assessment By: Loughry, J., Mcdonough, C. & Abba, A.Mnatalia chamorro solorzanoNo ratings yet
- Mir d245s & d45ks Rev.2Document1 pageMir d245s & d45ks Rev.2open hartigNo ratings yet
- Durastar DS1910HFDocument2 pagesDurastar DS1910HFEvelyn SigoliNo ratings yet
- MFE Study GuideDocument17 pagesMFE Study Guideahpohy100% (1)
- Redundant SystemDocument4 pagesRedundant Systemsuresh5254No ratings yet
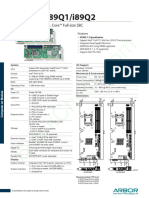
- Arbor Hicore I89q1 I89q2Document2 pagesArbor Hicore I89q1 I89q2Waleed MareeNo ratings yet
- Desquamative GingivitisDocument18 pagesDesquamative GingivitisSonia MehtaNo ratings yet
- Photo Courtesy of Paul Jeffrey.: ON THE WEB: Http://cisr - Jmu.edu/journal/16.2/index - HTMDocument1 pagePhoto Courtesy of Paul Jeffrey.: ON THE WEB: Http://cisr - Jmu.edu/journal/16.2/index - HTMpaulmazziottaNo ratings yet
- Waste Management: Construction Materials As A Waste Management Solution For Cellulose SludgeDocument8 pagesWaste Management: Construction Materials As A Waste Management Solution For Cellulose Sludgedante mormontoy ruelasNo ratings yet
- Lab Report 3Document8 pagesLab Report 3sagarchawlaNo ratings yet
- Curriculum Vitae MAJESTICDocument1 pageCurriculum Vitae MAJESTICSoekhaidir SuripnoNo ratings yet
- XBTG5230 PDFDocument112 pagesXBTG5230 PDFjcudrisNo ratings yet
- Alok Upd. ResumeDocument3 pagesAlok Upd. ResumeBhavesh MishraNo ratings yet
- Hydraulic Principles PDFDocument35 pagesHydraulic Principles PDFeng_zidNo ratings yet
- Tier1-Cvs, Cns and Respiratory Safety Pharmacology, Herg Assay Tier2-Gi, Renal and Other StudiesDocument30 pagesTier1-Cvs, Cns and Respiratory Safety Pharmacology, Herg Assay Tier2-Gi, Renal and Other StudiesCHETHAN K SNo ratings yet