You might also like
- Bones of The Upper LimbDocument27 pagesBones of The Upper LimbFoday H Kalokoh100% (1)
- Excitable Cells: Monographs in Modern Biology for Upper School and University CoursesFrom EverandExcitable Cells: Monographs in Modern Biology for Upper School and University CoursesNo ratings yet
- About Pleomorphism. Suppressed Medical KnowledgeDocument17 pagesAbout Pleomorphism. Suppressed Medical KnowledgeCarl MacCord50% (2)
- Complete Biology For Cambridge Secondary 1 Workbook Pam Large ZDocument128 pagesComplete Biology For Cambridge Secondary 1 Workbook Pam Large ZPhyo Eaindray Myint50% (2)
- Fisiopatologia de La EpilepsiaDocument18 pagesFisiopatologia de La EpilepsiaVíctor ManuelNo ratings yet
- Pogil Evolution and SelectionDocument7 pagesPogil Evolution and Selectionapi-320698226100% (1)
- Chapter 3 - Uvea - 2012 - Clinical Anatomy and Physiology of The Visual SystemDocument21 pagesChapter 3 - Uvea - 2012 - Clinical Anatomy and Physiology of The Visual SystemAldo CortesNo ratings yet
- Macroanatomy and Microanatomy of The Temporal Lobe 2007Document12 pagesMacroanatomy and Microanatomy of The Temporal Lobe 2007Juan José Pabón CastroNo ratings yet
- Acute and Chronic Pain Following Craniotomy: A Review: ReviewarticleDocument12 pagesAcute and Chronic Pain Following Craniotomy: A Review: ReviewarticleКулик АндрійNo ratings yet
- Arteries of The Insula: U T, M.D., M. G Y, M.D., O A - M, M.D., D C. H. Y, R.NDocument12 pagesArteries of The Insula: U T, M.D., M. G Y, M.D., O A - M, M.D., D C. H. Y, R.NMihaela AndreiNo ratings yet
- CerebrumDocument26 pagesCerebrumMangala Prema MohanarangamNo ratings yet
- Spinal Cord Anatomy, Localization, and Overview of Spinal Cord SyndromesDocument25 pagesSpinal Cord Anatomy, Localization, and Overview of Spinal Cord SyndromesValentina Pimentel PatiñoNo ratings yet
- Thespinalcord: A Review of Functional NeuroanatomyDocument18 pagesThespinalcord: A Review of Functional NeuroanatomyasfwegereNo ratings yet
- Anatomyandphisiology Lab Topic-3 Module3Document21 pagesAnatomyandphisiology Lab Topic-3 Module3Ash PadillaNo ratings yet
- Скелетна ммускулна клетка - устройство на саркомерDocument4 pagesСкелетна ммускулна клетка - устройство на саркомерMartin PetkovNo ratings yet
- AnatosuchusDocument6 pagesAnatosuchusJorge BarrientosNo ratings yet
- J Otot 2010 08 007Document6 pagesJ Otot 2010 08 007Fatharani FazaNo ratings yet
- Anatomy of The Elbow: Trauma and ReconstructionDocument13 pagesAnatomy of The Elbow: Trauma and ReconstructionSrinivasNo ratings yet
- Topographic Anatomy of The Insular Region: U T, M.D., D C. H. Y, R.N., O A - M, M.D., M. G Y, M.DDocument14 pagesTopographic Anatomy of The Insular Region: U T, M.D., D C. H. Y, R.N., O A - M, M.D., M. G Y, M.DAlejandro TpnsNo ratings yet
- The Normal Anterior Inferior Cerebellar ArteryDocument19 pagesThe Normal Anterior Inferior Cerebellar Artery16fernandoNo ratings yet
- Managementofelbow Trauma:: Anatomy and ExposuresDocument11 pagesManagementofelbow Trauma:: Anatomy and ExposuresMishael Diaz PoncecaNo ratings yet
- Applied Epidural Anatomy CEACCP 2005Document3 pagesApplied Epidural Anatomy CEACCP 2005eryxspNo ratings yet
- 1 s2.0 S2666084923005089 MainDocument6 pages1 s2.0 S2666084923005089 MainGabriel JoséNo ratings yet
- Norm Anatomy Elbow 2011Document11 pagesNorm Anatomy Elbow 2011Екатерина БербецNo ratings yet
- The Anatomy of The Cerebellum: ErebellumDocument6 pagesThe Anatomy of The Cerebellum: ErebellumjoyousNo ratings yet
- Articulo DX Semana 14Document7 pagesArticulo DX Semana 14Valeria Garcia QuijanoNo ratings yet
- Gliomas Insulares PDFDocument8 pagesGliomas Insulares PDFRathavishwarajNo ratings yet
- Wrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHDocument22 pagesWrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHMd Ahsanuzzaman PinkuNo ratings yet
- Anatomy and Landmarks For Branches of The Brachial Plexus: A Vade MecumDocument10 pagesAnatomy and Landmarks For Branches of The Brachial Plexus: A Vade MecumRocoso StonesNo ratings yet
- Auricula Orejita PDFDocument8 pagesAuricula Orejita PDFRICARDO ANDRES TOSCANO VILLAMIZARNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument4 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- Oseo UppDocument28 pagesOseo UppMariana Mojica DiazNo ratings yet
- Tokyo, Japan and Vienna, Austria: Disclosure: The Authors Have No Financial InterestsDocument14 pagesTokyo, Japan and Vienna, Austria: Disclosure: The Authors Have No Financial InterestsVanessaGGSNo ratings yet
- The Anatomy of The Cerebellum TicsDocument7 pagesThe Anatomy of The Cerebellum Ticsvikhen0712No ratings yet
- 2 - Neuroanatomy of SpineDocument18 pages2 - Neuroanatomy of SpineAndre ZanellaNo ratings yet
- Ocular Embryology With Special Reference To Chamber Angle DevelopmentDocument2 pagesOcular Embryology With Special Reference To Chamber Angle DevelopmentnabilahNo ratings yet
- Did Mozart Have A Chronic Extradural HaeDocument4 pagesDid Mozart Have A Chronic Extradural HaeGiovanni MercuriNo ratings yet
- Imaging of Skull Base: Pictorial Essay: M - S - H NDocument12 pagesImaging of Skull Base: Pictorial Essay: M - S - H NGeorge Harrison Jr.No ratings yet
- Uru Ingles ADocument7 pagesUru Ingles ASaurabh SatheNo ratings yet
- The Cranial Cavity: Bony FeaturesDocument5 pagesThe Cranial Cavity: Bony FeaturesbibierabiaNo ratings yet
- Ekenstam 1985Document9 pagesEkenstam 1985Arthur TeixeiraNo ratings yet
- (Journal of Neurosurgery) Microsurgical Anatomy of The Middle Cerebral ArteryDocument19 pages(Journal of Neurosurgery) Microsurgical Anatomy of The Middle Cerebral ArteryMarilenaNo ratings yet
- Anatomia Normal y Variantes Anatomicas Por RM Wrist and HandDocument14 pagesAnatomia Normal y Variantes Anatomicas Por RM Wrist and HandOscar Huancoillo TiconaNo ratings yet
- Applied Anatomy of The Wrist, Thumb and Hand: Joints, Joint Capsules and LigamentsDocument10 pagesApplied Anatomy of The Wrist, Thumb and Hand: Joints, Joint Capsules and LigamentsroyvillafrancaNo ratings yet
- 3013 - Bookfile 200 900 (200 400)Document201 pages3013 - Bookfile 200 900 (200 400)gemapesfNo ratings yet
- Musculo TemporalDocument4 pagesMusculo TemporalSimón Pérez LópezNo ratings yet
- Post - Triangle of NeckDocument5 pagesPost - Triangle of NeckAjay Pal NattNo ratings yet
- Sulcal and Gyral Anatomy of The Basal Occipital-Temporal LobeDocument7 pagesSulcal and Gyral Anatomy of The Basal Occipital-Temporal LobeRubén Darío Arenas DíazNo ratings yet
- Ten Questions On Kienbock's DiseaseDocument6 pagesTen Questions On Kienbock's DiseaseProfesseur Christian DumontierNo ratings yet
- Spinal CordDocument8 pagesSpinal CordCUESCANO, CRISTEL G. BSMT 2-ANo ratings yet
- Normal Brain Anatomy On Magnetic Resonance ImagingDocument9 pagesNormal Brain Anatomy On Magnetic Resonance ImagingNathaly CantorNo ratings yet
- Ligamentos de La ManoDocument9 pagesLigamentos de La ManoEnrique Maturana SepulvedaNo ratings yet
- Musculo TemporalDocument6 pagesMusculo TemporalNaim CalilNo ratings yet
- Topognosis of Facial Nerve LesionsDocument11 pagesTopognosis of Facial Nerve LesionsAudiologiaNo ratings yet
- Chapter2 - Meninges and CSFDocument19 pagesChapter2 - Meninges and CSFthegiggleloopNo ratings yet
- Chapter 12 - Zebrafish Myology - 2020 - The Zebrafish in Biomedical ResearchDocument7 pagesChapter 12 - Zebrafish Myology - 2020 - The Zebrafish in Biomedical ResearchNicolas BaronNo ratings yet
- Central Core of The Cerebrum: Laboratory InvestigationDocument7 pagesCentral Core of The Cerebrum: Laboratory InvestigationZeptalanNo ratings yet
- Periocularanatomy Andaging: Lily P. Love,, Edward H. FarriorDocument7 pagesPeriocularanatomy Andaging: Lily P. Love,, Edward H. FarriorCamila CrosaraNo ratings yet
- Alberta Stroke Program Early CT Score - 1Document4 pagesAlberta Stroke Program Early CT Score - 1Ardina Nur PramudhitaNo ratings yet
- Anatomy Lecture Chapter 12 Vertebral Coulmn and Back v2Document3 pagesAnatomy Lecture Chapter 12 Vertebral Coulmn and Back v2Neil Vincent De AsisNo ratings yet
- L1-Bones of Upper LimbDocument25 pagesL1-Bones of Upper LimbYakshender AhlawatNo ratings yet
- Chapter 36 Internal EarDocument23 pagesChapter 36 Internal EarMohan PalanimalaiNo ratings yet
- Emea Knot Tying ManualDocument64 pagesEmea Knot Tying ManualTiger PowerNo ratings yet
- Transforaminal Intraoperative Complications - Local Dural TearDocument8 pagesTransforaminal Intraoperative Complications - Local Dural TearTiger PowerNo ratings yet
- InterLaminar Window DescriptionDocument6 pagesInterLaminar Window DescriptionTiger PowerNo ratings yet
- Arterial Blood Gas AnalysisDocument35 pagesArterial Blood Gas AnalysisTiger PowerNo ratings yet
- Psych9223 F2014 L08 GroupDataDocument67 pagesPsych9223 F2014 L08 GroupDataCassia LmtNo ratings yet
- TG FormatDocument5 pagesTG FormatEncluna Lindon JayNo ratings yet
- Final ExamsDocument15 pagesFinal ExamsMelody WhelanNo ratings yet
- Fidelis & Zirondi (2021) - Floração CerradoDocument7 pagesFidelis & Zirondi (2021) - Floração CerradorobertoNo ratings yet
- Bartonella in Benin 2016Document9 pagesBartonella in Benin 2016Yahya TfeilNo ratings yet
- Chapter 10. Human Body System: Respiratory System and Circulatory SystemDocument61 pagesChapter 10. Human Body System: Respiratory System and Circulatory SystemMary Faith BerenguelNo ratings yet
- TP1. Ingles Scribd. Pte SimpleDocument5 pagesTP1. Ingles Scribd. Pte SimplegabyNo ratings yet
- IHCDocument4 pagesIHCSharmishtha ShekharNo ratings yet
- Methods of Bacterial Isolation and Culture and Preservation Microbial Isolation Techniques NotesDocument4 pagesMethods of Bacterial Isolation and Culture and Preservation Microbial Isolation Techniques Notesmervyn balbuenaNo ratings yet
- Skeletal Muscle Cells and Their Packaging Into Muscles: PerimysiumDocument14 pagesSkeletal Muscle Cells and Their Packaging Into Muscles: PerimysiumMadeleine RayosNo ratings yet
- Valuasi Ekonomi Ekosistem Hutan MangroveDocument16 pagesValuasi Ekonomi Ekosistem Hutan MangroveYonarizaGuchianoNo ratings yet
- Notes For Internal Examination (General English)Document22 pagesNotes For Internal Examination (General English)MehrinNo ratings yet
- Organisational BehaviourDocument251 pagesOrganisational Behaviourjhumki123No ratings yet
- ThermoregulationDocument1 pageThermoregulationJoannaNo ratings yet
- HISTOPATHOLOGY NotesDocument3 pagesHISTOPATHOLOGY NotesAndrea Faye MONTERONANo ratings yet
- Zani MCQs Zoo301Document10 pagesZani MCQs Zoo301mc190404891 ZAINAB ARSHADNo ratings yet
- Kapa Hifi PCR Kit Kr0368 - v13.19Document6 pagesKapa Hifi PCR Kit Kr0368 - v13.19Victor TieuNo ratings yet
- Bio2 11 - 12 Q3 0401 PF FDDocument32 pagesBio2 11 - 12 Q3 0401 PF FDLindsay SicatNo ratings yet
- 10 de Thi Hoc Ki 1 Tieng Anh 9 Moi Co Dap An Va Loi Giai Chi Tiet 1671183059Document135 pages10 de Thi Hoc Ki 1 Tieng Anh 9 Moi Co Dap An Va Loi Giai Chi Tiet 1671183059hongnhatnguyen0No ratings yet
- W1-6 Biochemistry of Vision and Hearing Lecture PDFDocument75 pagesW1-6 Biochemistry of Vision and Hearing Lecture PDFSAHIL AGARWALNo ratings yet
- Research Paper Topics For Junior HighDocument5 pagesResearch Paper Topics For Junior Highpqltbarif100% (1)
- CH 7 Test Bank For Essential Cell Biology 3rd Edition AlbertsDocument20 pagesCH 7 Test Bank For Essential Cell Biology 3rd Edition AlbertsRokia GhariebNo ratings yet
- MRP Transporters and Low Phytic Acid Mutants in Major Crops: Main Pleiotropic Effects and Future PerspectivesDocument12 pagesMRP Transporters and Low Phytic Acid Mutants in Major Crops: Main Pleiotropic Effects and Future PerspectivesAbrham FeyisaNo ratings yet
- Gen Bio 1 Love of Lab Group Performance Task 1Document2 pagesGen Bio 1 Love of Lab Group Performance Task 1Ryan GañaNo ratings yet
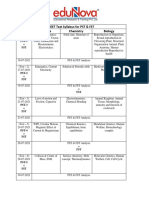
- NEET Test Syllabus For PST & FST Date Physics Chemistry BiologyDocument2 pagesNEET Test Syllabus For PST & FST Date Physics Chemistry BiologyDivyansh KhatediyaNo ratings yet
- Andraeanum Var. Tropical) Pada Media MS DenganDocument10 pagesAndraeanum Var. Tropical) Pada Media MS DenganDhiya Nur DzakirahNo ratings yet
- Soal Kelas 11Document8 pagesSoal Kelas 11Satria Muh. TaqwaNo ratings yet