You might also like
- Skinny Gut Diet by Brenda Watson - ExcerptDocument24 pagesSkinny Gut Diet by Brenda Watson - ExcerptCrown Publishing Group56% (9)
- Medical AbbreviationDocument13 pagesMedical AbbreviationRaf Luis100% (1)
- PN NCLEX PRACTICE TESTDocument75 pagesPN NCLEX PRACTICE TESTjedisay1100% (1)
- Clinical Microbiology and Infection: Original ArticleDocument6 pagesClinical Microbiology and Infection: Original ArticleAkira Masumi100% (1)
- Anxiety DisordersDocument9 pagesAnxiety DisordersShara SampangNo ratings yet
- Hema312 Lec 10 Trans 10Document14 pagesHema312 Lec 10 Trans 104jzbxz64kqNo ratings yet
- International Standard: Colorimetry - CIE 1976 L A B Colour SpaceDocument18 pagesInternational Standard: Colorimetry - CIE 1976 L A B Colour SpaceEduard-Marius Lungulescu100% (2)
- Current Surgical Therapy 13th EditionDocument61 pagesCurrent Surgical Therapy 13th Editiongreg.vasquez490100% (40)
- Iso 9352 - 1995Document9 pagesIso 9352 - 1995Eduard-Marius LungulescuNo ratings yet
- Parasitic Infections and the Immune SystemFrom EverandParasitic Infections and the Immune SystemFelipe KierzenbaumNo ratings yet
- Icpc Pembahasan Coding Dengan IcpcDocument52 pagesIcpc Pembahasan Coding Dengan IcpcMelita RamadhaniNo ratings yet
- Case Study Endometrial PDFDocument17 pagesCase Study Endometrial PDFapi-279886264No ratings yet
- BPJS Coding IcdDocument4 pagesBPJS Coding IcdDewi Agustina100% (1)
- Autoclave CycleDocument7 pagesAutoclave CycleHaroon RasheedNo ratings yet
- The Stethoscope As A Vector of Infectious Diseases in The Paediatric DivisionDocument3 pagesThe Stethoscope As A Vector of Infectious Diseases in The Paediatric DivisionAlagarsamy GNo ratings yet
- Cereus 3Document19 pagesCereus 3Natalia DuqueNo ratings yet
- Vibrio Cholerae Strains ComparisonDocument4 pagesVibrio Cholerae Strains ComparisonKhaye MendozaNo ratings yet
- Ienz 37 2039918Document11 pagesIenz 37 2039918Robert StryjakNo ratings yet
- Community Acquired Pneumonia In+childrenDocument4 pagesCommunity Acquired Pneumonia In+childrendai shujuanNo ratings yet
- Aborto Septico 2020Document5 pagesAborto Septico 2020Adrian Pardo VillegasNo ratings yet
- Sphingomonas KoreensisDocument11 pagesSphingomonas KoreensisSMIBA MedicinaNo ratings yet
- Bloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesDocument4 pagesBloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesrasioputraNo ratings yet
- Aj Infection Control 2011 Vestimenta de Enf y Medicos Como Posible Fuente de Infeccion NosocomialDocument5 pagesAj Infection Control 2011 Vestimenta de Enf y Medicos Como Posible Fuente de Infeccion NosocomialJuanNo ratings yet
- Miller 2016Document4 pagesMiller 2016Lidia JimenezNo ratings yet
- Jurnal O3Document5 pagesJurnal O3Ghita ShupiyesaNo ratings yet
- Acinetobacter BaumanniiDocument12 pagesAcinetobacter BaumanniiKenneth Smith IINo ratings yet
- Highly Effective Against EsblDocument9 pagesHighly Effective Against Esblgaurav rawalNo ratings yet
- Vondessauer 2016Document7 pagesVondessauer 2016زينب محمد عبدNo ratings yet
- Microorganisms Associated With Incisional Infections After Gastrointestinal Surgery in Dogs and CatsDocument6 pagesMicroorganisms Associated With Incisional Infections After Gastrointestinal Surgery in Dogs and CatsAriel GamalNo ratings yet
- 1 s2.0 S0196655316307350 MainDocument3 pages1 s2.0 S0196655316307350 MainBam ManNo ratings yet
- American Journal of Infection ControlDocument6 pagesAmerican Journal of Infection ControlAuliasari SiskaNo ratings yet
- Evaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalDocument6 pagesEvaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalEditor IJTSRDNo ratings yet
- Risk Factors For Ventilator-Associated Events - Liu 2019Document6 pagesRisk Factors For Ventilator-Associated Events - Liu 2019Maxi BoniniNo ratings yet
- tmp64DF TMPDocument4 pagestmp64DF TMPFrontiersNo ratings yet
- Effectiveness of Contact Isolation During A Hospital Outbreak of Methicillin-Resistant Staphylococcus AureusDocument9 pagesEffectiveness of Contact Isolation During A Hospital Outbreak of Methicillin-Resistant Staphylococcus Aureusmoniart2587No ratings yet
- Intestinal colonization with multidrug-resistant enterobacteriaceae in a healthy adult populationDocument8 pagesIntestinal colonization with multidrug-resistant enterobacteriaceae in a healthy adult populationOpenaccess Research paperNo ratings yet
- The Surveillance of Antibiotics Resistance in Indonesia: A Current ReportsDocument6 pagesThe Surveillance of Antibiotics Resistance in Indonesia: A Current ReportsRahmanu ReztaputraNo ratings yet
- datapage,+IJIC A 21712 ODocument9 pagesdatapage,+IJIC A 21712 OFizza MaryamNo ratings yet
- The Frequency of Influenza and Bacterial Co-Infection - A SystematDocument12 pagesThe Frequency of Influenza and Bacterial Co-Infection - A Systematrahma_husna_1No ratings yet
- Epidemiology Roun1Document10 pagesEpidemiology Roun1FebniNo ratings yet
- Ajol File Journals - 233 - Articles - 208047 - Submission - Proof - 208047 2773 517395 1 10 20210602Document6 pagesAjol File Journals - 233 - Articles - 208047 - Submission - Proof - 208047 2773 517395 1 10 20210602Musa ZiramiNo ratings yet
- Microbiological Profile of Bronchoalveolar Lavage in Patients With Nosocomial Pneumonia in Neonatal Intensive Care UnitDocument4 pagesMicrobiological Profile of Bronchoalveolar Lavage in Patients With Nosocomial Pneumonia in Neonatal Intensive Care UnitIJAR JOURNALNo ratings yet
- Abhishek K. Mishra and Vijay S. WadhaiDocument8 pagesAbhishek K. Mishra and Vijay S. WadhaiAbdul WakeelNo ratings yet
- Hospital Acquired Infection Incidence and Risk FactorsDocument7 pagesHospital Acquired Infection Incidence and Risk FactorsKshitiz112No ratings yet
- Biotechnology LawDocument20 pagesBiotechnology LawAKASH CHOUDHARYNo ratings yet
- Pseudomonas AeruginosaDocument8 pagesPseudomonas AeruginosaPatricia HerreraNo ratings yet
- FaccDocument11 pagesFaccendaNo ratings yet
- Literature Review On Nosocomial Infection PDFDocument6 pagesLiterature Review On Nosocomial Infection PDFafmzrvaxhdzxjs100% (1)
- ArticuloDocument4 pagesArticuloGrecia Alí AceroNo ratings yet
- Efficacy of Pneumonia Decision Rule in Vaccinated ChildrenDocument7 pagesEfficacy of Pneumonia Decision Rule in Vaccinated ChildrenMuhammad FachrurozieNo ratings yet
- Newly Identified Viruses in Human Gastroenteritis: Espid R RDocument4 pagesNewly Identified Viruses in Human Gastroenteritis: Espid R RArianne LasamNo ratings yet
- 05 N017 2931Document13 pages05 N017 2931anju negalurNo ratings yet
- Microbial Etiology of Pneumonia: Epidemiology, Diagnosis and Resistance PatternsDocument19 pagesMicrobial Etiology of Pneumonia: Epidemiology, Diagnosis and Resistance PatternsRizki Handayani SiregarNo ratings yet
- Thesis Topics About BacteriaDocument4 pagesThesis Topics About BacteriaWriteMyPaperOneDayHartford100% (2)
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- A.baumanii Colonization vs. InfectionDocument12 pagesA.baumanii Colonization vs. InfectionIvana ErakovicNo ratings yet
- Oral Care Interventions and Oropharyngeal Colonization in Children Receiving Mechanical VentilationDocument12 pagesOral Care Interventions and Oropharyngeal Colonization in Children Receiving Mechanical VentilationAdila amalitaNo ratings yet
- (03241750 - Acta Medica Bulgarica) Fungal Peritonitis Due To Gastroduodenal Perforation - Diagnostic and Treatment ChallengesDocument8 pages(03241750 - Acta Medica Bulgarica) Fungal Peritonitis Due To Gastroduodenal Perforation - Diagnostic and Treatment ChallengesTeodorNo ratings yet
- A. baumannii Infection Risk Factors and Outcomes in Hospitalized ChildrenDocument11 pagesA. baumannii Infection Risk Factors and Outcomes in Hospitalized ChildrenIvana ErakovicNo ratings yet
- Providencia StuartiiDocument7 pagesProvidencia StuartiiNoviaCandraDwipaNo ratings yet
- Atencio Azucena Besares Special ProblemDocument18 pagesAtencio Azucena Besares Special ProblemShane Catherine BesaresNo ratings yet
- Thannesberger 2017Document15 pagesThannesberger 2017Денис КрахоткинNo ratings yet
- JurnalDocument6 pagesJurnalAchmad YunusNo ratings yet
- Literature Review On Nosocomial InfectionDocument5 pagesLiterature Review On Nosocomial Infectioneowcnerke100% (1)
- BJBMS 19 86Document8 pagesBJBMS 19 86overmegaNo ratings yet
- Isolation of Pathogens Causing Sepsis Pus and Infected Wounds From Critical Care Unit A Retrospective Study - 2Document8 pagesIsolation of Pathogens Causing Sepsis Pus and Infected Wounds From Critical Care Unit A Retrospective Study - 2Omoding EmmanuelNo ratings yet
- CholeraDocument7 pagesCholeraDewa Ayu Pradnya DewiNo ratings yet
- Study of The Prevalence of Nosocomial Infections in The University Hospital Center of Béni-Messous, Algiers in 2023 - AlgeriaDocument6 pagesStudy of The Prevalence of Nosocomial Infections in The University Hospital Center of Béni-Messous, Algiers in 2023 - AlgeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Corona Virus VaccineDocument2 pagesCorona Virus VaccineYemtaNo ratings yet
- 2016 Article 645Document10 pages2016 Article 645Betharia TriayuNo ratings yet
- Arthropod Vector: Controller of Disease Transmission, Volume 1: Vector Microbiome and Innate Immunity of ArthropodsFrom EverandArthropod Vector: Controller of Disease Transmission, Volume 1: Vector Microbiome and Innate Immunity of ArthropodsStephen K. WikelNo ratings yet
- Cydzik-Kwiatkow-2015-Nitrogen-converting CommuDocument9 pagesCydzik-Kwiatkow-2015-Nitrogen-converting CommuEduard-Marius LungulescuNo ratings yet
- Alsubaie-2021-Role of Ionic Surfactants On TheDocument12 pagesAlsubaie-2021-Role of Ionic Surfactants On TheEduard-Marius LungulescuNo ratings yet
- Gamma Radiation Synthesis of Silver Nanoparticles/Chitosan Composites With Antimicrobial PropertiesDocument8 pagesGamma Radiation Synthesis of Silver Nanoparticles/Chitosan Composites With Antimicrobial PropertiesEduard-Marius LungulescuNo ratings yet
- Auriemma-2021-Microstructural Insight On StraiDocument14 pagesAuriemma-2021-Microstructural Insight On StraiEduard-Marius LungulescuNo ratings yet
- Emerging Threat and Cons ChallengeDocument25 pagesEmerging Threat and Cons ChallengeIis SabahudinNo ratings yet
- Polymer Composites With Self-Regulating Temperature Behavior: Properties and CharacterizationDocument20 pagesPolymer Composites With Self-Regulating Temperature Behavior: Properties and CharacterizationEduard-Marius LungulescuNo ratings yet
- Vanysacker-2013-Microbial Adhesion and BiofilmDocument12 pagesVanysacker-2013-Microbial Adhesion and BiofilmEduard-Marius LungulescuNo ratings yet
- Nutrients Removal From Aquaculture Wastewater by Biofilter/Antibiotic-Resistant Bacteria SystemsDocument17 pagesNutrients Removal From Aquaculture Wastewater by Biofilter/Antibiotic-Resistant Bacteria SystemsEduard-Marius LungulescuNo ratings yet
- Radiation Processing of Styrene-isoprene-styrene/Poly (Epsilon-Caprolactone) BlendsDocument18 pagesRadiation Processing of Styrene-isoprene-styrene/Poly (Epsilon-Caprolactone) BlendsEduard-Marius LungulescuNo ratings yet
- Nutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsDocument16 pagesNutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsEduard-Marius LungulescuNo ratings yet
- Rozylo-2021-Spectroscopic, Mineral, and AntioxDocument9 pagesRozylo-2021-Spectroscopic, Mineral, and AntioxEduard-Marius LungulescuNo ratings yet
- Abdel-Salam-2014-Citric Acid Effects On BrainDocument11 pagesAbdel-Salam-2014-Citric Acid Effects On BrainEduard-Marius LungulescuNo ratings yet
- Articles Vs Proceedings PapersDocument13 pagesArticles Vs Proceedings PapersMuhammad Azuan TukiarNo ratings yet
- Kaewunruen-2017-Vibration Attenuation at RailDocument6 pagesKaewunruen-2017-Vibration Attenuation at RailEduard-Marius LungulescuNo ratings yet
- Nutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsDocument16 pagesNutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsEduard-Marius LungulescuNo ratings yet
- Applied SciencesDocument21 pagesApplied SciencesEduard-Marius LungulescuNo ratings yet
- Nutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsDocument16 pagesNutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsEduard-Marius LungulescuNo ratings yet
- Nutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsDocument16 pagesNutrients Removal From Aquaculture Wastewater by Biofilter - Antibiotic-Resistant Bacteria SystemsEduard-Marius LungulescuNo ratings yet
- D2565 - Plastic WeatheringDocument4 pagesD2565 - Plastic WeatheringEduard-Marius LungulescuNo ratings yet
- BS en 14476-2013 + A1-2015 PDFDocument44 pagesBS en 14476-2013 + A1-2015 PDFHoàng Minh Tuyên100% (2)
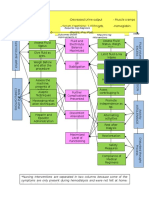
- Critical Care Concept Map 2Document1 pageCritical Care Concept Map 2nursing concept mapsNo ratings yet
- Label The Diagram of The HeartDocument1 pageLabel The Diagram of The HeartMarie HutsonNo ratings yet
- Ketogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4Document21 pagesKetogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4donmd98No ratings yet
- Research Article: Garbha Sanskar-Need of Every Expectant Mother For Healthy ProgenyDocument4 pagesResearch Article: Garbha Sanskar-Need of Every Expectant Mother For Healthy ProgenySayaliNo ratings yet
- Rated Review ExamplesDocument41 pagesRated Review ExamplesMaria AspriNo ratings yet
- Saritha Front Page HeddingsDocument13 pagesSaritha Front Page Heddingssaritha OrugantiNo ratings yet
- My Parkinson's CB - Blue Heron Health NewsDocument23 pagesMy Parkinson's CB - Blue Heron Health Newscuongch30% (1)
- Anemia in Pregnancy ACOGDocument126 pagesAnemia in Pregnancy ACOGrohitNo ratings yet
- FHPL Network Hopsitals List - 7dec2017Document819 pagesFHPL Network Hopsitals List - 7dec2017Badhra Rao100% (2)
- Evidence Supporting Broader AccessDocument4 pagesEvidence Supporting Broader Accessedi_wsNo ratings yet
- Kalsitonin PDFDocument12 pagesKalsitonin PDFFariz KasyidiNo ratings yet
- EBPG European Best Practice Guidelines on Haemodialysis Part 2Document43 pagesEBPG European Best Practice Guidelines on Haemodialysis Part 2Владимир Ильич ЛенинNo ratings yet
- Exercise # 3: How To Use CalculatorDocument5 pagesExercise # 3: How To Use CalculatorAbdullah SajidNo ratings yet
- Comparing Phenol and Apamarg Kshar for Sclerotherapy in Bleeding PilesDocument8 pagesComparing Phenol and Apamarg Kshar for Sclerotherapy in Bleeding PilesNishant SainiNo ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- Biology 12 Unit 9 Assignment 2 Blood Type and Immune Response Virtual LabDocument2 pagesBiology 12 Unit 9 Assignment 2 Blood Type and Immune Response Virtual Labapi-3385788740% (1)
- Examination of LabelDocument3 pagesExamination of LabelSintel Yonzipur9No ratings yet
- Lymphoma NPRDocument5 pagesLymphoma NPRHavier EsparagueraNo ratings yet
- Daftar Pustaka-DikonversiDocument7 pagesDaftar Pustaka-DikonversiRomi MufthiNo ratings yet
- Brisbane Convention Centre Hosts Innovative Urology ConferenceDocument4 pagesBrisbane Convention Centre Hosts Innovative Urology ConferenceDio Mafazi FabriantaNo ratings yet
- SPED Elementary Non-Graded 2016 by RegionDocument32 pagesSPED Elementary Non-Graded 2016 by RegionChristian PentinioNo ratings yet