You might also like
- Micro-computed Tomography (micro-CT) in Medicine and EngineeringFrom EverandMicro-computed Tomography (micro-CT) in Medicine and EngineeringKaan OrhanNo ratings yet
- Reducing The Model Variance of A Rectal Cancer Segmentation NetworkDocument9 pagesReducing The Model Variance of A Rectal Cancer Segmentation NetworkDiego Marcelino Santos SilvaNo ratings yet
- Information: A Novel Bio-Inspired Deep Learning Approach For Liver Cancer DiagnosisDocument36 pagesInformation: A Novel Bio-Inspired Deep Learning Approach For Liver Cancer DiagnosiselmannaiNo ratings yet
- 3D Fully CNNDocument8 pages3D Fully CNNkoushikraj900No ratings yet
- Applsci 12 08650 v2Document15 pagesApplsci 12 08650 v2Sabir MuhammadNo ratings yet
- Prostate Segmentation ThesisDocument9 pagesProstate Segmentation Thesisgj9ggjry100% (2)
- Diagnostics 12 01788 v2Document17 pagesDiagnostics 12 01788 v2Shakhnazar ZhumabekovNo ratings yet
- Pancreas Disease Detection and Segmentation Using Abdominal CT ScanDocument9 pagesPancreas Disease Detection and Segmentation Using Abdominal CT ScanIJAR JOURNALNo ratings yet
- Brain Tumour Detection Using The Deep LearningDocument8 pagesBrain Tumour Detection Using The Deep LearningIJRASETPublicationsNo ratings yet
- Encoder Decoder With Dense Dilated Spatial Pyramid Pooling For Prostate MRDocument8 pagesEncoder Decoder With Dense Dilated Spatial Pyramid Pooling For Prostate MRSatyaNurAnggaNo ratings yet
- (IJCST-V10I5P48) :mrs J Sarada, Pandi Vishnu VardhanDocument6 pages(IJCST-V10I5P48) :mrs J Sarada, Pandi Vishnu VardhanEighthSenseGroupNo ratings yet
- Automated Segmentation of Head CT Scans for Computerassisted Craniomaxillofacial Surgery Applying a Hierarchical Patchbased Stack of Convolutional Neural NetworksInternational Journal of Computer Assisted RadiologyDocument9 pagesAutomated Segmentation of Head CT Scans for Computerassisted Craniomaxillofacial Surgery Applying a Hierarchical Patchbased Stack of Convolutional Neural NetworksInternational Journal of Computer Assisted Radiologyhajar.outaybiNo ratings yet
- Report 13Document11 pagesReport 13opmobile gamerNo ratings yet
- Multimodal Brain MRI Tumor Segmentation Via Convolutional Neural Network PDFDocument10 pagesMultimodal Brain MRI Tumor Segmentation Via Convolutional Neural Network PDFSharif AhamedNo ratings yet
- Ijcrt2105065 1Document4 pagesIjcrt2105065 1Sheba ParimalaNo ratings yet
- Transformer Based 3D U Net For Pulmonary Vessel Segmentation and Artery Vein Separation From CT ImagesDocument15 pagesTransformer Based 3D U Net For Pulmonary Vessel Segmentation and Artery Vein Separation From CT ImagesThérèse NtabuhasheNo ratings yet
- BT4470 ReportDocument8 pagesBT4470 Reporthero huNo ratings yet
- Qin 2018Document5 pagesQin 2018sadNo ratings yet
- Applied Sciences: Classification of Brain Tumors From MRI Images Using A Convolutional Neural NetworkDocument13 pagesApplied Sciences: Classification of Brain Tumors From MRI Images Using A Convolutional Neural NetworkZe PushNo ratings yet
- Three-Dimensional Computerized Orthognathic Surgical Treatment PlanningDocument10 pagesThree-Dimensional Computerized Orthognathic Surgical Treatment PlanningRajan KarmakarNo ratings yet
- Efficacy of Yolo Deep Learning Algorithm Kidney Tumor Cancer DetectionDocument8 pagesEfficacy of Yolo Deep Learning Algorithm Kidney Tumor Cancer DetectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CT-based Deep Learning Segmentation of Ovarian Cancer and The Stability of The Extracted Radiomics FeaturesDocument12 pagesCT-based Deep Learning Segmentation of Ovarian Cancer and The Stability of The Extracted Radiomics Featuressukeshini jadhavNo ratings yet
- 2023 A Literature Review On "Lung Cancer Detection Approaches Using Medical Images"Document9 pages2023 A Literature Review On "Lung Cancer Detection Approaches Using Medical Images"graythomasinNo ratings yet
- An Efficient Visualization and Segmentation of Lung CT Scan Images For Early Diagnosis of CancerDocument5 pagesAn Efficient Visualization and Segmentation of Lung CT Scan Images For Early Diagnosis of Cancermaruthi631No ratings yet
- Cascaded V-Net Using ROI Masks For Brain Tumor SegmentationDocument11 pagesCascaded V-Net Using ROI Masks For Brain Tumor SegmentationRobertoNo ratings yet
- S3D-UNet Separable 3D U-Net For Brain Tumor SegmentationDocument11 pagesS3D-UNet Separable 3D U-Net For Brain Tumor SegmentationFaysal AhamedNo ratings yet
- ReportDocument18 pagesReportEshwarNo ratings yet
- DenseX-Net An End-To-End Model For Lymphoma Segmentation in Whole-Body PET CT ImagesDocument15 pagesDenseX-Net An End-To-End Model For Lymphoma Segmentation in Whole-Body PET CT Imagesahmet buğraNo ratings yet
- Idea Proyecto 2Document13 pagesIdea Proyecto 2Marianne GillyNo ratings yet
- Lung Cancer DetectionDocument8 pagesLung Cancer DetectionAyush SinghNo ratings yet
- Kidney and Tumor Segmentation Using Combined Deep Learning MethodDocument11 pagesKidney and Tumor Segmentation Using Combined Deep Learning MethodegamrNo ratings yet
- 1 s2.0 S1746809422003809 MainDocument12 pages1 s2.0 S1746809422003809 MainDhanush BedreNo ratings yet
- 2023-智能图像配准-attention guided refine and deformationDocument13 pages2023-智能图像配准-attention guided refine and deformationbo zhaoNo ratings yet
- Automatic Segmentation of Liver Tumor in CT ImagesDocument6 pagesAutomatic Segmentation of Liver Tumor in CT Imagesmanju.dsatmNo ratings yet
- 10 1016@j Bbe 2019 06 003Document11 pages10 1016@j Bbe 2019 06 003HaryadiNo ratings yet
- Lung Cancer DetectionDocument5 pagesLung Cancer Detectionkoushikraj900No ratings yet
- Research Paper On Computed TomographyDocument8 pagesResearch Paper On Computed Tomographyafmcsmvbr100% (1)
- Multi-Branch Ensemble Learning Architecture Based On 3D CNN For False Positive Reduction in Lung Nodule DetectionDocument12 pagesMulti-Branch Ensemble Learning Architecture Based On 3D CNN For False Positive Reduction in Lung Nodule DetectionRonald BbosaNo ratings yet
- Conebeam CT of The Head and Neck, Part 2: Clinical ApplicationsDocument8 pagesConebeam CT of The Head and Neck, Part 2: Clinical ApplicationshaneefmdfNo ratings yet
- State-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant PlacementDocument7 pagesState-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant Placementanimeilove3No ratings yet
- MAjor Project ReportDocument27 pagesMAjor Project ReportAman MouryaNo ratings yet
- Lung Cancer Detection Using Fusion, CNN and YOLO in MATLABDocument10 pagesLung Cancer Detection Using Fusion, CNN and YOLO in MATLABIJRASETPublicationsNo ratings yet
- PravallikaDocument28 pagesPravallikaVegesana SumythriNo ratings yet
- Deep Semantic Segmentation of Kidney and Space-Occupying Lesion Area Based On SCNN and Resnet Models Combined With Sift-Flow AlgorithmDocument12 pagesDeep Semantic Segmentation of Kidney and Space-Occupying Lesion Area Based On SCNN and Resnet Models Combined With Sift-Flow AlgorithmMuhamad Praja DewanataNo ratings yet
- Development of A Deep-Learning-Based Method For Breast Ultrasound Image SegmentationDocument6 pagesDevelopment of A Deep-Learning-Based Method For Breast Ultrasound Image SegmentationKEREN EVANGELINE I (RA1913011011002)No ratings yet
- Comparison of Cone-Beam Imaging With Orthopantomography and Computerized Tomography For Assessment in Presurgical Implant DentistryDocument10 pagesComparison of Cone-Beam Imaging With Orthopantomography and Computerized Tomography For Assessment in Presurgical Implant DentistryMihai DascalescuNo ratings yet
- LungSEEK - 3D Selective Kernel Residual Network For Pulmonary Nodule DiagnosisDocument14 pagesLungSEEK - 3D Selective Kernel Residual Network For Pulmonary Nodule DiagnosisRonald BbosaNo ratings yet
- 3-D Segmentation AlgorithmDocument13 pages3-D Segmentation Algorithmkoushikraj900No ratings yet
- Bai 2019Document12 pagesBai 2019SINGSTONNo ratings yet
- RPTDocument6 pagesRPTparagkulkarni11No ratings yet
- Nnu-Net: A Self-Configuring Method For Deep Learning-Based Biomedical Image SegmentationDocument14 pagesNnu-Net: A Self-Configuring Method For Deep Learning-Based Biomedical Image SegmentationTrisha DasNo ratings yet
- A Novel Bio-Inspired Deep Learning Approach For LiDocument36 pagesA Novel Bio-Inspired Deep Learning Approach For LiMohamed SalahNo ratings yet
- Performance Evaluation of TumorDocument12 pagesPerformance Evaluation of TumorAnonymous lVQ83F8mCNo ratings yet
- Brain Tumor Segmentation ThesisDocument7 pagesBrain Tumor Segmentation Thesisafksooisybobce100% (2)
- Automated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesDocument10 pagesAutomated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesTELKOMNIKANo ratings yet
- Effective Kidney Segmentation Using Gradient Based Approach in Abdominal CT ImagesDocument6 pagesEffective Kidney Segmentation Using Gradient Based Approach in Abdominal CT ImagesrajNo ratings yet
- 5 - PET and CT Image Fusion of Lung Cancer With Siamese Pyramid Fusion NetworkDocument11 pages5 - PET and CT Image Fusion of Lung Cancer With Siamese Pyramid Fusion NetworkNguyễn Nhật-NguyênNo ratings yet
- Brain Tumour Segmentation Based On Magnetic Resonance ImagingDocument3 pagesBrain Tumour Segmentation Based On Magnetic Resonance ImagingShay Patrick CormacNo ratings yet
- A Morphological Operation-Based Approach For Sub-Pleural Lung Nodule Detection From CT ImagesDocument6 pagesA Morphological Operation-Based Approach For Sub-Pleural Lung Nodule Detection From CT Imagesrekka mastouriNo ratings yet
- BM3 PlusDocument2 pagesBM3 Pluscicik wijayantiNo ratings yet
- UST - A1100 Guardian Overfill Prevention ValveDocument1 pageUST - A1100 Guardian Overfill Prevention ValvelauraNo ratings yet
- Hydrodynamic Calculation Needle Valve Closing Flow Against The Direction of Movement of The PistonDocument23 pagesHydrodynamic Calculation Needle Valve Closing Flow Against The Direction of Movement of The Pistonmet-calcNo ratings yet
- Super Capacitor - Seminar Report, PPT, PDF For ECE StudentsDocument3 pagesSuper Capacitor - Seminar Report, PPT, PDF For ECE StudentsvvkrkzNo ratings yet
- Dictionaries Godot GDScript Tutorial Ep 12 Godot TutorialsDocument4 pagesDictionaries Godot GDScript Tutorial Ep 12 Godot TutorialsChris LewinskyNo ratings yet
- End-Of-Sale and End-Of-Life Announcement For The Cisco Telepresence Sx20 With 12X CameraDocument3 pagesEnd-Of-Sale and End-Of-Life Announcement For The Cisco Telepresence Sx20 With 12X CameraAmrous MohamedNo ratings yet
- Biochips: Submitted byDocument17 pagesBiochips: Submitted byCharina Marie CaduaNo ratings yet
- Yellampalli S. Wireless Sensor Networks - Design, Deployment..2021Document314 pagesYellampalli S. Wireless Sensor Networks - Design, Deployment..2021Myster SceneNo ratings yet
- Section - : Exit To Main MenuDocument186 pagesSection - : Exit To Main Menuadi67% (3)
- SWFP66D Series Fine-Grinding Hammer Mill: Operation ManualDocument65 pagesSWFP66D Series Fine-Grinding Hammer Mill: Operation ManualDanielDeFrancescoNo ratings yet
- Factors Affecting System Complexity: CouplingDocument4 pagesFactors Affecting System Complexity: CouplingJaskirat KaurNo ratings yet
- Accelerating IceCubes Photon Propagation Code WitDocument11 pagesAccelerating IceCubes Photon Propagation Code WitNEed for workNo ratings yet
- Jun Jul 2021Document32 pagesJun Jul 2021Lai Kok UeiNo ratings yet
- Juhi S. Khandekar: Email ID: Contact (M) : +91-7710007972Document1 pageJuhi S. Khandekar: Email ID: Contact (M) : +91-7710007972Reddi SyamsundarNo ratings yet
- EasyEPD2 Manual 2003 12 04Document98 pagesEasyEPD2 Manual 2003 12 04Filipe LaínsNo ratings yet
- Face Recognition - HLD - V1Document4 pagesFace Recognition - HLD - V1SuryaNo ratings yet
- Temperature Control Systems: Product Reference Guide For Truck and Trailer ApplicationsDocument40 pagesTemperature Control Systems: Product Reference Guide For Truck and Trailer ApplicationsSaMos AdRiianNo ratings yet
- Submittal Patterson Bombs PDFDocument77 pagesSubmittal Patterson Bombs PDFFred GarciaNo ratings yet
- SHS SEPNAS Paper-Formatting-guidelines Pr2 Quantitative ReserachDocument24 pagesSHS SEPNAS Paper-Formatting-guidelines Pr2 Quantitative ReserachAnalyn RosarioNo ratings yet
- Progress Test 2 (Units 4-6) : Name - ClassDocument6 pagesProgress Test 2 (Units 4-6) : Name - ClassРусланNo ratings yet
- Betelhem MekuriaDocument59 pagesBetelhem MekuriaabenuzzionNo ratings yet
- SM ATF400G-6 - EN - Intern Use OnlyDocument1,767 pagesSM ATF400G-6 - EN - Intern Use OnlyReinaldo Zorrilla88% (8)
- About GoogleDocument7 pagesAbout GoogleMeera Gayathri DNo ratings yet
- Tanque Atlas Copco 2021Document23 pagesTanque Atlas Copco 2021Joel C. VegaNo ratings yet
- Module 2 Global Youth: A Estrutura Do Teste Sintetiza-Se No Quadro SeguinteDocument11 pagesModule 2 Global Youth: A Estrutura Do Teste Sintetiza-Se No Quadro SeguinteLaura HenriquesNo ratings yet
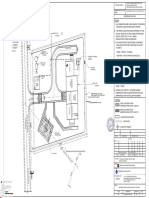
- PD2083-EL-HAZ-A1-004.pdf HAZARDOUS AREA CLASSIFICATION SV STATION-3Document1 pagePD2083-EL-HAZ-A1-004.pdf HAZARDOUS AREA CLASSIFICATION SV STATION-3Alla Naveen KumarNo ratings yet
- Cie-III Verilog HDL QPDocument2 pagesCie-III Verilog HDL QPvijayarani.katkamNo ratings yet
- The Students Allotted With The Is Available at The End of The DocumentDocument4 pagesThe Students Allotted With The Is Available at The End of The DocumentShivaNo ratings yet
- Module 11A.5.2 L1 2016-08-16Document234 pagesModule 11A.5.2 L1 2016-08-16Abdul Aziz KhanNo ratings yet
- Lesson 12&13Document4 pagesLesson 12&13Jhynes RenomeronNo ratings yet