Professional Documents
Culture Documents
Nassal Provocation Test - 5
Uploaded by
Lengkung BajaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nassal Provocation Test - 5
Uploaded by
Lengkung BajaCopyright:
Available Formats
Review article
Supported by a grant from AstraZeneca Pharmaceuticals
Nasal provocation testing: a review
Ludmila I. Litvyakova, MD, PhD* and James N. Baraniuk, MD†
Objective: This review focuses on the uses of nasal provocation testing (NPT) for effects. The possibility that an allergen
scientific investigations of the mechanisms of allergic and nonallergic rhinitis. It may cause a positive nasal response,
also describes the use of NPT as a diagnostic tool in clinical practice. The indica- but not be relevant to a subject’s
tions, contraindications, advantages, and limitations of different techniques for asthma must be considered.15 The
evaluation of nasal responses are reviewed. The paper familiarizes investigators same dilemma occurs with allergen
with particulars of different nasal delivery systems, provocation agents, nasal skin testing for prediction of bronchial
patency measurements, secretion collection, and nasal lavage techniques. responses to allergen. Despite these
Data Sources: Relevant publications obtained from a literature review. concerns NPT generally offers a safer
Study Selection: Relevant publications on the topics of NPT, allergic, and alternative to bronchial provocation
nonallergic rhinitis were critically evaluated. when evaluating the role of specific
Results and Conclusions: To date, NPT has been used primarily as a research allergens in a patients’ asthma. Indica-
tool for the investigation of allergic and nonallergic rhinitis with a wide variety of tions for scientific investigations have
techniques depending on the specific scientific purposes. NPT will continue to been described (Table 2) because NPT
provide useful information about the pathogenesis of airway diseases. Standardized allows ready access to respiratory mu-
nasal provocation testing has the potential to become a more frequently used clinical cosa for sampling of mediators, cells,
test in the diagnosis of allergic and occupational rhinitis and for determination of the and secretions.
appropriate and focused therapy.
Ann Allergy Asthma Immunol 2001;86:355–365. CONTRAINDICATIONS
Acute bacterial or viral mucosal in-
INTRODUCTION niques, the absence of standardization flammation is accompanied by rhinor-
Nasal provocation testing (NPT) has for methods and some reagents, and rhea, stuffy nose, and nonspecific hy-
been crucial for the scientific investi- lack of validated direct comparisons perreactivity, which preclude NPT
gation of the pathophysiology, immu- between methods. The absence of data (Table 3). In accordance to the general
nology, and pharmacotherapy of aller- regarding inter- and intra-subject vari- approach in allergy, generalized aller-
gic and nonallergic rhinitis. These ability needs to be addressed to stan- gic reactions, including anaphylactic
studies also offer insights into the dardize allergen NPT so that it may shock and severe bronchospasm and
pathophysiology of hyperreactivity in become a more widely accepted diag- status asthmaticus can occurr in pa-
lower airways because of the similarity nostic method.1,2 tients during the acute phase or exac-
of the response to allergen challenge of erbation of their allergic disease (rhi-
the upper and lower airways. Several INDICATIONS nitis, food allergy, drug allergy, insect
techniques of NPT have been used de- NPT is mainly used for scientific pur- allergy, urticaria) or in patients with
pending on purpose of the investiga- poses in the United States,3 but in sev- previous anaphylactic reactions to the
tion. Each method has its own advan- eral European countries, it is used for allergen of interest. NPT should not be
tages and disadvantages. Limitations clinical evaluation.4,5 conducted in patients with restricted
include the wide variety of test tech- Indications for NPT as an office pro- lung capacity. The danger of miscar-
cedure range from diagnosis of com- riage due to anaphylaxis prohibits NPT
plicated clinical cases to selection of during pregnancy. A wide variety of
optimal therapy (Table 1). Nasal aller- drugs can cause false-negative NPT
* International Center of Interdisciplinary Stud-
ies of Immunology, Georgetown University, gic reactions are thought to be predic- and should be withdrawn before test-
Washington, DC. tive of bronchial responses. This can ing (Table 4). Nasal congestion may
† Division of Rheumatology, Immunology, and occur only if both target organs are also result from oral contraceptives
Allergy, Georgetown University, Washington, DC. sensitized and responsive to the same and preparations containing sulfite pre-
Supported by PHS Award RO1 AI42403.
Received for publication May 12, 2000. allergen. Under this frequent circum- servatives such as bronchodilator solu-
Accepted for publication in revised form De- stance, nasal provocations will likely tions (metaproterenol, isoproterenol,
cember 30, 2000. be predictive of bronchial, asthmatic isoetharine), analgesics (meperidine),
VOLUME 86, APRIL, 2001 355
Table 1. Clinical Indications for NPT increase false-positive results. Viral in- European practice, but are not ac-
1. To identify a role of an individual, fections alter patterns of vascular per- cepted for clinical use in the United
nonstandardized, novel, or unique meability and mucus macromolecule States. Testing should be performed by
specific allergen in the nasal target exocytosis and induce mucosal hyper- well trained personnel in a well
organ using allergen preparations.6 responsiveness.33 NPT should be de- equipped unit under standard condi-
2. To confirm the role of a special layed to 2 to 4 weeks after an infection. tions4 to readily identify and limit non-
occupational agent, such as baker’s Nasal reactivity is also decreased for 4 specific irritant effects, and treat aller-
yeast and dusts, carpenter’s saw dusts,
to 8 weeks after nasal or sinus surgery gic side effects as soon as they appear.
or latex.7,8
3. To confirm the clinical relevance of a
since atypical reactions may be in- The best time for NPT is in the morn-
specific allergen in patients with duced.21 Nasal pathology such as pol- ing, before lunch time because this
multiple positive allergy skin tests.6 yps, atrophic rhinitis, and septal devi- limits effects of daily-life stimuli
4. To assess the role of allergens ation can give false-positive or false- (fumes, cold air, spicy food, physical
implicated by a patient’s history when negative results in NPT depending on exercise). After adaptation to room
allergy skin test and/or RAST are their severity.34 temperature for 30 minutes, clinical
negative or when the reactions of the symptom score and basal nasal func-
nasal mucosa to an allergen are more TECHNIQUES tion should be evaluated. Basal nasal
pronounced than those of skin.9,10 Rhinoscopic examination should pre- function can be measured by nasal
5. To investigate food-induced
cede any nasal provocation to inspect peak expiratory flow rate [NPEFR], or
rhinorrhea.11
6. To determine if nasal application of
the baseline condition of nasal mucosa nasal peak inspiratory flow rate
allergen can induce symptoms in the and evaluate structural pathology such [NPIFR], anterior or posterior rhino-
conjunctiva, middle ear, sinus, and as polyps, septal deviation, atrophic manometry, or acoustic rhinometry
lower respiratory airways.12–14 rhinitis or sinusitis. If significant (gives volume of nasal cavity). Method
7. To confirm the allergic nature of pathologic changes are found, NPT of NPEFR is not accepted by experts in
asthma, since positive nasal reactions may not be required. Subjects should the United States. These measures are
may be obtained when the have previous skin tests or/and RAST repeated three times and the mean
corresponding bronchial provocation performed to evaluate the likely atopic value is recorded. Each measurement
tests are negative15 or can not be safely sensitivities. should differ from the mean by less
performed.
For clinical purposes, the most prac- than 10% to 15%.35,37 Values within
8. To confirm nasal reactivity before
starting local nasal immunotherapy.16
tical method is simple, safe, and easily 15% of normal are recommended be-
repeatable (Fig 1).4,34 –36 Most of the cause preexisting nasal obstruction
clinical protocols are consistent with may lead to false-negative results be-
cause further obstruction may not be
and eye drops (sulfacetamide, pred- Table 2. Indications for the possible, measurable or significant.
nisolone, dexamethasone). Oral con- Scientific Investigations The wider side of the nose is used for
traceptives may also influence NPT challenge, but airway obstruction mea-
1. To investigate the spectrum of allergen-
since women taking these drugs show surements are performed on both sides
induced immediate and late phase
squamous metaplasia, interepithelial responses and the dose dependent
during NPT to identify nasal cycle ef-
edema, glandular hyperplasia, histio- nature of these reactions.17–19 fects.4
The nasal provocation begins with
cytic proliferation, and fibrous tissue 2. To identify the morphological and
cellular responses to inhaled allergens administration of a known volume of a
deposition similar to those patients
using nasal lavage, biopsy, and diluent solution such as phosphate-
with chronic hypertrophic nonallergic brushing.20,21
rhinitis.31 The need for withdrawal of 3. To detect chemical mediators, markers
these medications before the nasal of glandular exocytosis, and vascular
Table 3. Absolute Contraindications
challenge is not clear. permeability in nasal lavage following 1. Acute bacterial or viral rhinitis or
Recent rhinitis can result in nasal allergen provocation.22,23 sinusitis
priming to allergen or upregulation of 4. To assess the response of nasal airways 2. Acute period or exacerbation of allergic
the mechanisms of nasal hyperreactiv- to allergens and nonallergic provocative disease (rhinitis, food allergy, drug
agents and following changes in allergy, insect allergy, urticaria)
ity.32 NPT should be performed at least bronchial responsiveness.24–26 3. Previous anaphylactic reaction to an
2 to 4 weeks after any acute allergic 5. To examine the therapeutic effects of allergen
episode or seasonal allergic rhinitis. drugs such as antihistamines, 4. Severe general diseases or acute
Differentiation of allergic perennial corticosteroids, cromoglycate, period of diseases, especially severe
rhinitis from nonallergic represents a anticholinergic medications, and asthma, obstructive bronchial diseases,
difficult problem because nonallergic vasoconstrictors on acute, late phase, cardiopulmonary diseases with
mechanisms may lead to chronic nonspecific, and other aspects of restricted lung capacity
airway diseases.27 5. Pregnancy
changes in nasal reactivity and may
356 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
buffered saline with 0.4% phenol, lac- 3 to 4 ⫽ 1 point; 5 or more ⫽ 3 blockage and itching.3,37 Changes in
tated Ringer’s solution, or normal sa- points), pruritus (nose, palate or ear ⫽ the nasal temperature (using thermog-
line into one or both nostrils using a 1 point each), rhinorrhea (0 to 3 raphy) and the pH of nasal secretions
metered dose delivery device. This points), blockage (1 to 3 points), and have also been proposed as endpoints.
challenge will detect nonspecific re- ocular symptoms (1 point). The end- Allergen challenge makes the pH more
sponses. Over the next 15 minutes, point is the amount of antigen required alkaline, while the temperature in-
sneezes are counted, nasal discharges to produce a total symptom score of 5 creases.40,41 These latter methods are
are collected, and pruritus, rhinorrhea, of a maximum of 13. The severity of not widely used.
nasal blockage, and ocular symptoms each sensation can also be evaluated False-positive results can be caused
are scored. Symptom scoring systems by 10-cm linear visual analog scale: by preservatives in extracts such as
including 10-cm linear analog scales, mild, 1 to 3 cm; moderate, 4 to 7 cm; phenol, glycerol, benzalkonium chlo-
4-point severity scales, and other ordi- and severe, 8 to 10 cm at the dose that ride; extremes of extract pH, tempera-
nal methods have been used. If there caused a positive response.38 Accord- ture, and osmolarity; evaluation within
are no clinical symptoms or significant ing to German guidelines, positive test 2 to 4 weeks of allergic, viral or bac-
changes of rhinomanometric measure- criteria should include flow reduc- terial rhinitis; and when allergen ex-
ments (reduction ⬍ 20% by baseline), tion ⬎ 40% and/or more than three tract concentrations reach 1:500 wt/vol
then allergen is deposited into the score points: secretion, 0 to 2 points or higher.28,34,35 Appropriate vehicle
nose. An approximate guide for the (moderate, 1 point; severe, 2 points); control solutions are essential to iden-
starting dose is determined before NPT sneezing, 0 to 2 points (0 to 2 tify nonspecific irritant reactions and
(see “Outcomes”). During allergen ap- sneezes ⫽ 0 point; 3 to 5 sneezes ⫽ 1 prevent false-positive test results. Ex-
plication the patient must hold his point; ⬎5 sneezes ⫽ 2 points); addi- tracts should be used at room temper-
breath to avoid inhaling allergen into tional symptoms such as tearing, itch- ature and pH of 5 to 8.28 The allergen
the larynx or lower airways. If the ini- ing (eyes, throat) ⫽ 1 point; conjunc- should be diluted in isoosmolar solu-
tial nasal allergen response is negative tivitis, cough, urticaria, and/or tion such as 0.9% saline or lactated
after 15 minutes, then the extract con- dyspnea ⫽ 2 points.39 Another investi- Ringer’s solution. These issues are es-
centration can be increased 3-fold. gators considered the positive NPT pecially important if the allergen ex-
These sequential increments can be with a decrease of 20% or more in tracts are prepared by the investigator.
given at 15-minute intervals. Doses are NEPFR and occurrence of nasal symp- Latex solution provides a good illus-
increased in step-wise fashion until a toms such as sneezes, rhinorrhea, nasal tration of these problems.42
positive result is obtained, a maximum The NPT is considered to be true
concentration is given without any sig- negative if the patient has no clinical
Table 4. Relative Contraindications
nificant reaction, or concentrations of symptoms and no changes of nasal pa-
1:500 wt/vol or higher are reached that 1. Episodes of allergic or infectious rhinitis tency after receiving the 1:1,000 wt/
cause nonspecific irritant effects in (2 to 4 weeks) vol extract or maximum allergen
nonallergic control subjects, and espe- 2. Nasal surgery (6 to 8 weeks after nasal dose.35
surgery)
cially at levels above 1:100 with house False-negative NPT occur after the
3. Nasal pathology such as polyps,
dust and fungus extracts.35 atrophic rhinitis, or a deviated nasal
use of contraindicated medications;
septum. within 8 weeks of nasal surgery, in
OUTCOMES 4. Treatment with certain medications. patients with atrophic rhinitis, nasal
Clinical symptoms of sneezing, itch- Recommended withdrawal periods for polyps, or occasionally after specific
ing, rhinorrhea, and obstructed nasal drugs before NPT21,28–30 immunotherapy. Subjects with chronic
airflow, and measures of nasal patency a. antihistamines (48 hours to 1 week) sinusitis may also have abnormal re-
are evaluated before administration of b. astemizole (4 to 12 weeks) sults since they have high levels of
each dose of allergen. NPT is stopped c. ketotifen (2 weeks) baseline mucous secretion, but do not
when a positive response occurs. The d. nasal corticosteroids (6 hours to 2 or respond to secretagogues such as
3–6 weeks)
intensity of the response is evaluated methacholine.43
e. sodium cromoglycate (1 or 3 weeks)
by dose of allergen given to patient and f. nasal ␣-adrenergic agonist (0 or 1
by total system score. True positive day)
ALLERGEN DOSING
response occurs at an allergen concen- g. oral corticosteroids ⬎10 mg (2 to 4 As a safety measure, it is recom-
tration causing at least two of the fol- weeks) mended to begin with a low allergen
lowing three criteria: 5 sneezes, 50% h. nonsteroidal analgesics (1 week) concentration. For skin test-negative
fall in NPEFR, or rhinorrhea.7 Other i. central nervous antihypertensives patients, the initial dose of allergen
symptom scoring systems have also such as reserpine, clonidine (3 should be in the range of 1:10,000 to
been used.4,38 For example, one previ- weeks) 1:5,000 wt/vol, or 50 to 100 PNU
ously validated system38 scores the j. imipramines and related tricyclic (overall pollen protein concentra-
drugs (2 to 3 weeks)
number of sneezes (0 to 2 ⫽ 0 points; tion).35 If the initial allergen applica-
VOLUME 86, APRIL, 2001 357
onyssinus was tested in patients with
mild and moderate skin reactions using
5, 50, 250, 500, and 1000 AU/mL ap-
plied in a fixed volume of 0.1 mL
aqueous solution per puff into each
nostril using metered dose pump
spray.10 Nasal immunotitration with 5,
10, 20, 40, 60, 80, 120, 160, and 240
AU was used before local immuno-
therapy with birch pollen aerosol and
powder methods. The initial treatment
dose was defined as the provocation
dose giving a positive reaction.46,47
Identification of a role of Blomia tropi-
calis as a cause of allergic rhinitis was
performed with concentrations of
1:125,000, 1:25,000, 1:5,000 vol/vol,
1:1,000, and 1:200 vol/vol.48 Compar-
isons of nasal reactions to house dust
and dust mite allergen extracts in skin
positive subjects with perennial rhinitis
were performed with 10, 100, 1,000,
and 2,000 PNU (house dust) and 5, 50,
and 500 PNU (dust mites). Allergic
patients varied considerably in nasal
sensitivity but all reacted to the final
dose.49 Identification of latex allergy
by NPT was performed with a
0.0005% latex solution.42 As can be
seen, the different methods of allergen
standardization such as allergy units
(AU) or biologic units (BU) and mea-
sures of overall pollen protein concen-
tration (PNU, wt/vol) make compari-
sons between studies difficult.
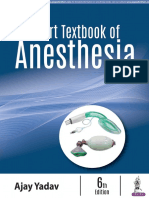
Figure 1. Protocol of NPT with allergens. DELIVERY SYSTEMS
For clinical purposes the most accept-
able simple techniques with good re-
tion is negative, then the extract con- disk method a 10-L dose and 4-mm producibility involve delivering aque-
centration can be increased in 3-fold paper disk could be applied.44 ous allergen extract by syringe, bottle
sequential increments at 15-minute in- A number of dosing regimens has dropper, micropipette or pump action
tervals (1:10,000, 1:3,000, 1:1,000 wt/ been used previously in NPT research nasal spray devices.14,35,50,51 Additional
vol).34,35 For subjects with positive protocols that may be applied to diag- techniques for research purposes in-
scratch and puncture tests, skin titra- nostic investigations.3 The dose de- clude: a powder and pollen grain in-
tion is performed with 3-fold dilutions pends on the technique of delivery, sufflator52,53; a “nasal pool” device for
of extracts. The concentration causing allergen preparation, and the purpose aqueous allergen extracts and soluble
a 3-mm wheal can be used for nasal of investigation. For the diagnosis of agents54; saturated wads of cotton wool
provocation.2 For intradermal tests, the dust mite allergy in childhood asthma, that are placed under the medial con-
lowest concentration generating a 10,000 AU/mL in one puff (0.01 to cha of the nose55; impregnated paper
wheal can be determined, and a con- 0.05 mL) was sprayed into each nasal discs placed on the inferior turbinate or
centration 10 times more dilute used cavity by a metered dose pump-spray nasal septum with forceps24,56; and
for NPT.34 For atomizer-dosimeter, a insufflator with a total dose of 800 to modified airbrush techniques.57 Each
dose of 0.1 mL of allergen per spray 1,000 AU for both nostrils.45 Nasal method has its own advantages and
could be used, whereas for the paper- sensitivity to Dermatophagoides pter limitations.
358 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
The area of distribution of solutions sponses in subjects who are studied out ter) that are dry can be placed to collect
deposited via syringes and droppers of the pollen season. Hydration of small, undiluted samples of nasal fluid.
cannot be readily predicted. These dried, defatted pollen grains leads to For example, the osmolarity of the ab-
bulk application methods have the risk the explosive release of a pollen eluate sorbed secretions was evaluated after
that, in some cases, fluid may be aspi- with high osmolarity60 that may be suf- nasal provocation with cold dry air and
rated into the larynx, inducing cough, ficient to cause irritation reactions in after stimulation with hypertonic saline
laryngeal irritation, edema, or bron- patients with nonspecific nasal hyper- and mannitol solutions (800 to 1,000
chospasm. These unwanted side ef- reactivity. Similarly, some patients mOsmol/kg H2O).63 The discs may
fects are very rare if care is taken to may have nonspecific reactions to the preferentially sample the sol phase of
instruct the patient not to inhale force- lactose that is used to pack the pollen the epithelial lining fluid, but may also
fully or bend their head backwards af- grains into inert capsules. Generally, promote transepithelial exudation of
ter the allergen is placed. Carriage of the dose of lactose is insufficient to interstitial fluid from the upper lamina
the allergen posteriorly by mucociliary cause symptoms in lactose-intolerant propria.64
clearance past the orifice of the Eusta- subjects. The option of using either unilateral
chian tube and into the pharynx may The “nasal pool” device, a com- or bilateral challenges is a great advan-
lead to nasopharyngeal swelling, itch, pressible plastic container with a nasal tage over bronchial provocations. Af-
or middle ear discomfort or dysfunc- adapter, offers significant improve- ter unilateral challenge, ipsilateral re-
tion.56 The use of 5- to 10-L pipettes ments of provocation and lavage tech- sponses are due to local, direct effects
allows the deposition of small, exact nique.54 The device can hold a soluble and recruited parasympathetic reflex
volumes of the allergen directly onto agent of known volume and concentra- effects whereas responses in the con-
the turbinate under direct rhinoscopic tion. The adapter is pressed to the nos- tralateral nostril represent “pure” para-
control. tril and the container compressed to sympathetic reflex effects (Fig 2).65
Nasal pump spray devices improve push the fluid into the nose for a pre-
contact of the provocative agent with the cise time and in the defined space of NASAL PATENCY
nasal mucosa by distributing it over the the anterior nasal cavity. The lavage MEASUREMENTS
exposed anterior nasal cavity surfaces. fluid is collected when the container is Nasal patency is extremely dependent
Precise volumes on the order of 100 L re-expanded. Any soluble agent can be on structures such as the septum and
are applied that generally do not lead to tested. Even children can use the de- nasal valve. The degree of swelling of
bronchospastic reactions. Unfortunately, vice correctly. A disadvantage of this venous sinusoids deep in the mucosa
the popular beclomethasone (Vancenase, technique is the unknown dilutional ef- regulates mucosal thickness, air space
Schering-Plough, Kenilworth, NJ and fect of nasal secretions by lavage fluid. volume and nasal patency. Other fac-
Beconase, Glaxo Wellcome, Research The devices are no longer available in tors that may also participate are mu-
Triangle Park, NC) spray bottles have the United States. cosal edema, cellular infiltration, and
become difficult to obtain because these Topical application of allergenic ex- the presence of luminal secretions.
products have been largely replaced in tracts by means of cotton wool swabs Several methods are available to mea-
the market place. Hand-held automizers in the middle meatus under the medial sure nasal airflow resistance: NPIFRs,
generate large-diameter particles, which concha, impregnated paper discs, or a NPEFRs, nasal spirometry, passive an-
helps to avoid the delivery of allergens to modified airbrush technique for appli- terior rhinomanometry, active anterior
the lower airways. Volumes of 0.2 to 0.5 cation onto the inferior turbinate have rhinomanometry, active posterior rhi-
mL per nostril are arbitrarily but com- been used mostly for scientific inves- nomanometry, balloon method/intra-
monly used.58 The materials suspended tigations. The site of provocation is nasal pressure measurements, and os-
in the mist may be more readily ab- relatively small, but changes in muco- cillometry.35,36 The nasal volume can
sorbed by the mucosa than with the bulk sal appearance can be observed at both be measured by acoustic rhinometry.66
application methods mentioned previ- the local site and more distant mucosal The nasal peak flow method is easy to
ously. Allergen meter-dose pump spray locations. Placing allergens in the mid- perform, inexpensive, and reasonably
was recommended for clinical routine dle meatus seems dangerous and po- well correlated with rhinomanometry,
and research in Europe.4 tentially could lead to sinusitis. but is less reproducible.36,67 Passive an-
Pollen grain insufflations can be Filter paper discs (3-mm diameter) terior rhinomanometry is a suitable
used to imitate natural exposures. This impregnated with allergen solution can technique for recording air pressure
technique is simple and the dose of be placed bilaterally by forceps on the and airflow during breath-holding and
pollen grains can be well controlled.59 anterior part of the inferior turbinate or has been used in children, patients with
However, most investigators prefer to nasal septum.61,62 Doses can be in- problematic dental prostheses, or with
use aqueous extracts because of the creased in step-wise fashion, but the an overactive gag reflex. In contrast,
hydroscopic properties of pollen. Very concentrations used may need to be this technique does not truly represent
high doses of pollens are generally re- individualized based upon the extract the physiologic breathing process.68
quired to obtain large magnitude re- potency.61 Larger discs (8-mm diame- Active anterior rhinomanometry eval-
VOLUME 86, APRIL, 2001 359
uates the pressure/volume or pressure/
flow relationship for the nostril during
tidal breathing. It is the most widely
used technique. However, the active
inspirations cause significant changes
in the nasal valve, resulting in breath-
to-breath variability in measurements.
This technique cannot be used for pa-
tients with fragile and bleeding nasal
mucosa or with frequent sneezing, be-
cause the insertion of nasal adapter of
device can alter the nasal valve.
Changes in resistance may be limited
when there is severe occlusion of a
nostril by turbinate hypertrophy, pol-
yps, septal deviation, or severe rhinor-
rhea at the onset of the study.69 Active
posterior rhinomanometry also records
pressure, volume and flow rates during
tidal breathing. This technique is not
suitable for children, patients unable to Figure 2. Nasal Provocation. Unilateral administration of allergen or other materials may lead to local,
tolerate the close-fitting masks, and ipsilateral responses, and parasympathetic reflex effects. Allergen leads to mast cell degranulation with
patients who cannot satisfactorily co- the release of histamine, LTC4/D4/E4, tryptase, and other mediators. Histamine acts upon H1-receptors
on endothelium to cause vascular permeability and exudation of an albumin-rich, watery discharge.
ordinate the required nasal, palate,
H1-receptors on nociceptive nerves lead to the sensation of itch. The neural mechanism leading to the
glottic, and breathing maneuvers.70 sensation of nasal congestion is not clearly understood. Nociceptive nerves may release neuropeptides
Acoustic rhinometry is a newer when activated (“axon response” mechanism). Substance P may cause glandular secretion, whereas
technique that measures the cross-sec- calcitonin gene-related peptide may cause vasodilation. Vasodilation with swelling of venous sinusoids
tional area of the nasal cavity.71 Pulsed leads to thickening of the mucosa and obstruction to nasal airflow. Histamine, as well as other mediators
sounds are broadcast into the nose. and cytokines, plays a key role in regulating cellular infiltration as seen in the late phase response and
Signals are reflected from the mucosal clinical allergic rhinitis. Activation of nociceptive nerves recruits bilateral parasympathetic reflexes that
walls back to a microphone. After cause acetylcholine-mediated glandular exocytosis.
spectral analysis, the cross-sectional
area is plotted as a function of distance
from the tip of the instrument. Changes different forms of rhinitis and in re- anterior flexion of the head combined
in the minimum cross-sectional area sponse to different provocation agents with nasal exhalation. This method
and volume of the cavity can be deter- and methods of collection. In clinical samples nasal and nasopharyngeal air-
mined. practice, secretions may be collected ways. ␣-Adrenergic agonists have
Nasal microcirculation has been by blowing directly onto a plastic film been used to improve fluid recovery.
used as an endpoint. Laser Doppler or into a funnel, cup, or tube. However, Druce and Raphael58,76 began using
velocimetry evaluates capillary blood interpretation may be difficult if the pump spray devices and collected se-
flow in the superficial mucosa.72 Ra- fluid is viscous or swallowed, collec- cretions by placing a small, soft, red,
dioactive xenon washout and clearance tions are incomplete, or the volumes of rubber 8F urethral catheter along the
of hydrogen (3H2) into exhaled nasal secretions are small. Secretion of 0.5 floor of the nostril. Unilateral provoca-
air are limited to research institu- mL (0.5 g) with 5 or more sneezes and tions could be performed with secre-
tions.73 Colorimetric evaluation of mu- ⬎20% decrease in peak flow is con- tions continuously collected from both
cosal erythema has also been used.74 sidered a positive test.37 sides. As described above, the nasal
Introduction of nasal lavage fluid pool device is a further refinement for
COLLECTION OF NASAL promotes collection for biochemical challenge, lavage, and collection.54
SECRETIONS AND analysis, but raises the problem of se- These techniques sample large sur-
LAVAGE FLUID cretion dilution. Naclerio75 pioneered face areas of mucosa, and can quantify
The amount, viscosity, and spinability the method of instilling 4 to 5 mL of vascular, glandular, neuronal, and cel-
of the nasal mucous discharge, and lavage fluid directly into the nose us- lular events simultaneously. Nasal la-
quantity of the mediators, cytokines, ing a pipette. Subjects are required to vages with isoosmolar saline can be
plasma proteins, glandular secretory hyperextend their necks and obstruct performed repeatedly without causing
products, extracellular matrix mole- their posterior nasopharynx by palatal nasal mucosal irritation. The disadvan-
cules and cells in lavage fluids vary in closure. Lavage fluid is recovered by tages of repeated nasal lavages are the
360 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
dilution of samples, the removal of im- mast cell mediators. The clinical nonspecific nasal hyperreactivity. Cap-
portant target cells such as adherent symptoms of the late phase response saicin stimulates nociceptive type C
eosinophils or metachromatic cells are limited to nasal congestion, poste- fibers and neuropeptide release from
during the initial provocations, and al- rior drainage of secretions, and sinus their sensory nerve endings. Capsaicin
terations in the dynamics of fluid flux or facial pressure. Cell, mediators, cy- provocations stimulate excessive glan-
across the mucosal barrier. In each tokines, and neurohormones in the na- dular secretion in a subset of vasomo-
method, the degree of dilution of the sal secretions of the late phase re- tor rhinitis subjects.91 Capsaicin also
original epithelial lining fluid cannot sponse are different from those of damages C fibers, and has been pro-
be determined. However, the addition acute response.18,85,86 The clinical im- posed as a treatment for nonallergic
of exogenous radiolabeled albumin or plications of having a late phase re- rhinitis.92 Bradykinin (BK) induces va-
lithium to the lavage fluid permits cal- sponse after NPT are still debated. The sodilatation and vascular permeability
culation of the percentage of recovery European Academy of Allergy and because of the stimulation of vascular
in research studies.77,78 These tech- Clinical Immunology’s recommenda- BK-B2 receptors.89,93 BK receptors on
niques have provided useful informa- tions for investigation of late-phase re- sensory nerves are upregulated in se-
tion about the amount of secretions, actions entail assessments at 0.5, 10, vere allergic rhinitis and lead to acti-
but they do not define their source, 20, 30, 45, 60 minutes, then every hour vation of cholinergic reflexes.94 Nico-
physical properties, or composition. to 10 hours after provocation.2 If a tine and serotonin also induce sensory
Measurement of urea in plasma and positive allergen response occurs, then nerve stimulation with presumed axon
lavage fluid provides an estimate of the the subject should be challenged with responses and cholinergic reflexes. Ir-
volume of epithelial lining fluid sam- the diluent to determine whether it had ritants such as ozone, sulfur dioxide,
pled.79 These methods are impractical induced a false-positive response. The formaldehyde, cigarette smoke, organ-
for office practice. Dry filter paper times for evaluation after the vehicle ic-solvent fumes, and cold air (or re-
discs collect only small quantities of challenge should be exactly the same warming after cold exposure) induce
undiluted secretions, limiting the num- as after the allergen. Both placebo re- nasal obstruction and rhinorrhea that
ber of analytes that can be assayed actors and subjects with nonspecific may be attributable to mast or epithe-
with precision. hyperresponsiveness will be detected. lial cell damage, the stimulation and
depolarization of trigeminal sensory
NASAL CYTOLOGY OTHER PROVOCATION nerves, and the induction of axon re-
Cellular changes during NPT can be AGENTS sponses and parasympathetic reflex-
evaluated by nasal smear, blown secre- Histamine produces the triple response es.65 Nasal and bronchial inhalations of
tions, cotton swabs, imprints, nasal of nerves in the skin and causes an hypertonic solutions of saline, manni-
scraping, nasal brushes, and biopsy. analogous pattern in the nose: stimula- tol or other solutes have been used to
Multiple methods of biochemical, his- tion of a population of H1-receptor investigate nonspecific irritant and
tochemical, immunochemical, and bearing type C neurons that mediate neural sensitivity, and may offer in-
electron micrographic can then be ap- itch that recruit cholinergic parasym- sights into exercise-induced asth-
plied.80 Collection of cells with cotton pathetic reflexes that induce glandular ma.60,95–98 NPT with acetylsalicylic
swabs is a simple but low reproducibil- exocytosis; stimulation of plasma ex- acid and lysyl-acetylsalicylic acid is a
ity technique.81 The advantage of im- travasation with stimulation of endo- helpful procedure for diagnosis of as-
prints and scrapings is that monocytes thelial H1-receptors leads to exudation pirin-sensitive asthma, but is less sen-
and lymphocytes can be enumerat- of plasma into the lamina propria lead- sitive than oral challenge.99 Lysyl-ace-
ed.82– 84 Nasal biopsy is rarely used for ing to edema with hydrostatically tylsalicylic acid is not approved for use
diagnostic purposes in rhinitis, but it driven exudation across the epithelium in the United States.
has provided valuable information into the nasal cavity to cause watery
about the ciliary dysfunction, role of rhinorrhea and vasodilatation of deep CONCLUSION
lymphocytes and cytokines in allergic venous sinusoids leading to mucosal As the methods of NPT become more
reactions. Biopsies are the only means thickening, reduced nasal patency, and standardized, we anticipate that NPT
to study the structural elements. The obstruction to airflow. All of these may become a more frequently used
nature of cellular infiltrates can be mechanisms are seen on the ipsilateral clinical tool. Its place will be to define
evaluated, but persistent bleeding may side after unilateral histamine provoca- the presence of allergic rhinitis when
follow the trauma of the biopsy. tion, whereas only the reflex-induced the history is highly suggestive but
glandular secretion is seen in the con- skin testing and RAST testing are neg-
LATE-PHASE RESPONSE tralateral nonchallenged nasal cavi- ative, for the evaluation of unique or
The immediate allergic response is ty.87– 89 Methacholine induces glandu- occupational allergens, and to demon-
characterized by itch, sneezing, rhinor- lar secretion only.90 Challenge with strate nonallergic, irritant, or nasal hy-
rhea, plasma exudation, and glandular histamine and methacholine have been perresponsiveness mechanisms. In
secretion attributable to the release of widely carried out for exploring of these instances, the NPT responses
VOLUME 86, APRIL, 2001 361
may lead to more appropriate and fo- nol 1997;79:427– 430. and during natural allergen exposure.
cused therapy. These tests may also be 11. Raphael G, Raphael MH, Kaliner M. Int Arch Allergy Immunol 1996;110:
useful to determine whether allergen- Gustatory rhinitis: a syndrome of food- 85–90.
specific IgE that can be detected in induced rhinorrhea. J Allergy Clin Im- 24. Sicherer S, Wood RA, Eggleston PA.
munol 1989;83:110 –115. Determinants of airway responses to
nonallergic nasal polyp and sinusitis
12. Filiaci F, Masieri S, Zambetti G, Or- cat allergen: comparison of environ-
subjects are relevant to the develop- lando MP. Nasal hypersensitivity in mental challenge to quantitative nasal
ment of these “nonatopic” diseases. purulent middle ear effusion. Allergol and bronchial allergen challenge. J Al-
The nasal mucosa will also be of value Immunopathol (Madr) 1997;25:91–94. lergy Clin Immunol 1997;99:
as a surrogate for bronchial testing, 13. Olive Perez A. Rhinitis and asthma: 798 – 805.
and will continue to provide useful in- nasal provocation test in the diagnosis 25. Fokkens WJ, Rowe-Jones JM. The
formation about the pathogenesis of of asthma. J Investig Allergol Clin Im- management of perennial
airway diseases. munol 1997;7:397–399. rhinitis–links between the nose, lung,
14. Pelikan Z, Pelikan-Filipek M. Role of asthma. Allergy 1997;52 (Suppl):
REFERENCES nasal allergy in chronic maxillary 20 –28.
sinusitis– diagnostic value of nasal 26. Adinoff AD, Corren J, Irvin CG.
1. Peebles RS, Hartert TV. In vivo diag-
nostic procedures: skin testing, nasal challenge with allergen. J Allergy Clin Changes in bronchial responsiveness
provocation, and bronchial provoca- Immunol 1990;86:484 – 491. following nasal provocation with aller-
tion. Methods 1997;13:14 –24. 15. Stenius-Aarniala BS, Malmberg CH, gen. J Allergy Clin Immunology 1992;
2. Melillo G, Bonini S, Cocco G, et al. Holopainen EE. Relationship between 89:611– 618.
Provocation tests with allergens. Al- the results of bronchial, nasal and con- 27. Andersson M, Greiff L, Svensson C, et
lergy 1997;52(Suppl):5–36. junctival provocation tests in patients al. Allergic and nonallergic rhinitis. In:
3. Naclerio RM, Norman PS. In vivo with asthma. Clin Allergy 1978;8: Busse W, Holgate ST, eds. Asthma
methods for the study of allergic rhi- 403– 409. and Rhinitis. Oxford: Blackwell, 1995:
nitis. Mucosal tests, techniques, and 16. Passalacqua G, Albano M, Pronzato C, 145–155.
interpretations. In: Middleton E, ed. et al. Long-term follow-up of nasal 28. Bousquet J, Francois-Bernard Michel.
Allergy: Principles and Practice. 5th immunotherapy to Parietaria: clinical Diagnostic tests. In: Korenblat PE,
ed. St Louis: Mosby, 1998;440 – 453. and local immunological effects. Clin Wedner HJ, eds. Allergy: Theory and
4. Bachert C. Nasal provocation test: crit- Exp Allergy 1997;27:904 –908. Practice. 2nd ed. Philadelphia: WB
ical evaluation. In: Ring J, Behrendt H, 17. Pelikan Z. Late and delayed responses Saunders, 1995:156 –163.
D, eds. New Trends in Allergy IV. of the nasal mucosa to allergen chal- 29. McLean JA, Bacon JR, Mathews KP,
Vieluf. Springer-Verlag Berlin Heidel- lenge. Ann Allergy 1978;41:37– 47. et al. Effects of aspirin on nasal re-
berg, 1997;277–280. 18. Pelikan Z. The late nasal response, its sponses in atopic subjects. J Allergy
5. Holopainen E, Tarkiainen E, Malm- clinical and immunologic features, Clin Immunol 1983;72:187–192.
berg H. Nasal challenge. Rhinology possible mechanisms and pharmaco- 30. Demoly P, Campbell A, Lebel B,
1976;14:181–188. logic modulation. Thesis. Free Univer- Bousquet J. Experimental models in
6. Lavasa S, Kumar L, Kaushal SC, Gan- sity in Amsterdam, 1996. rhinitis. Clin Exp Allergy 1999;29:
guli NK. Wheat threshing dust–a “new 19. Horak F, Toth J, Hirschwehr R, et al. 72–76.
allergen” in April-May nasobronchial Effect of continuous allergen chal- 31. Toppozada H, Toppozada M, El-
allergy. Indian Pediatr 1996;33: lenge on clinical symptoms and medi- Ghazzawi I, Elwany S. The human re-
566 –570. ator release in dust-mite–allergic pa- spiratory nasal mucosa in females us-
7. Hytonen M, Sala E. Nasal provocation tients. Allergy 1998;53:68 –72. ing contraceptive pills. An
test in the diagnostics of occupational 20. Del Prete GF, De Carli M, D’Elios ultramicroscopic and histochemical
allergic rhinitis. Rhinology 1996;34: MM, et al. Allergen exposure induces study. J Laryngol Otol 1984;98:43–51.
86 –90. the activation of allergen-specific Th2 32. Togias A. The role of enviromental
8. Gorski P, Krakowiak A, Pazdrak K, et cells in the airway mucosa of patients allergens in rhinitis. In: Busse W, Hol-
al. Nasal challenge test in the diagnosis with allergic respiratory disorders. Eur gate S, eds. Asthma and Rhinitis. Cam-
of allergic respiratory diseases in sub- J Immunol 1993;23:1445–1449. bridge, MA: Blackwell Scientific,
jects occupationally exposed to a high 21. Andersson M, Greiff L, Svensson C, 1995;1009 –1033.
molecular allergen (flour). Occup Med Persson C. Various methods for testing 33. Yuta A, Doyle WJ, Gaumond E, et al.
(Lond) 1998;48:91–97. nasal responses in vivo: a critical re- Rhinovirus infection induces mucous
9. Testa B, Mesolella C, Testa F, et al. view. Acta Otolaryngol 1995;115: hypersecretion. Am J Physiol 1990;
Comparison of SPT and NPT in the 705–713. 274:L1017–L1023.
ascertainment of nasal mucosa as 22. Walden SM, Proud D, Bascom R, et al. 34. Meltzer E, Schatz M, Zeiger R. Aller-
shock organ. Rhinology (Netherlands) Experimentally induced nasal allergic gic and nonallergic rhinitis. In:
1996;34:160 –162. responses. J Allergy Clin Immunol Middleton E, ed. Allergy: Principles
10. Kanthawatana S, Maturim W, Fooanan 1988;81:940 –949. and Practice. 4th ed. St Louis: Mosby,
S, Trakultivakorn M. Skin prick reac- 23. Wang D, Smitz J, Derbe MP, Clement 1993;1253–1288.
tion and nasal provocation response in PA. Concentrations of myeloperoxi- 35. Solomon WR. Nasal procative testing.
diagnosis of nasal allergy to the house dase in nasal secretions of atopic pa- In: Spector SL, ed. Provocation Test-
dust mite. Ann Allergy Asthma Immu- tients after nasal allergen challenge ing in Clinical Practice, vol 5. New
362 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
York: Marcel Dekker,1995:647– 692. lergy Asthma Immunol 1995;75: 241–246.
36. Malm L, Gerth van Wijk R, Bachert C. 501–506. 62. Baroody FM, Wageman M, Naclerio
Guidelines for nasal provocations with 50. Karlsson G, Rundcrantz H. Peroral RM. Comparison of the secretory re-
aspects on nasal patency, airflow, and chromones. A new way to treat allergic sponse of the nasal mucosa to metha-
airflow resistance. International Com- rhinitis? Acta Otolaryngol Suppl 1979; choline and histamine. J Appl Physiol
mittee on Objective Assessment of the 360:27–29. 1993;74:2661–2671.
Nasal Airways, International Rhino- 51. Mygind N, Vesterhauge S. Aerosol 63. Anderson SD, Togias A. Dry air and
logic Society. Rhinology 2000;38:1– 6. distribution in the nose. Rhinology hyperosmolar challenge in asthma
37. Wihl JA. Methodological aspects of 1978;16:131–136. and rhinitis. In: Busse W, Holgate S,
nasal allergen challenges based on a 52. Andri L, Senna GE, Betteli C, et al. eds. Asthma and Rhinitis. Cambridge,
three-year tree pollen immunotherapy Specific nasal provocation test with al- MA: Blackwell Scientific, 1995:1178 –
study. Allergy 1986;41:357–364. lergens in powder form proves a reli- 1195.
38. Linder A. Symptom scores as mea- able and reproducible technique. Al- 64. Erjefalt I, Persson CJ. On the use of
sures of the severity of rhinitis. Clin lergy 1992;47:243. absorbing discs to sample mucosal sur-
Allergy 1988;18:29 –37. 53. Connell JT. Quantitative intranasal face liquids. Clin Exp Allergy 1990;
39. Bachert C, Gonsior E, Berdel D, et al. pollen challenge. III. The priming ef- 20:193–198.
Richtlinien fur die Durchfuhrung von fect in allergic rhinitis. J Allergy 1969; 65. Baraniuk JN, Kaliner MA. Functional
nasalen Provokationstests mit Aller- 43:33– 42. activity of upper-airway nerves. In:
genen Bei Erkrankungen der oberen 54. Greiff L, Pipkorn U, Alkner U, Pers- Busse W, Holgate S, eds. Asthma and
Luftwege. Allergologie 1990;13: son C. The nasal pool device applies Rhinitis. Cambridge, MA: Blackwell
53–55. controlled concentrations of solutes on Scientific, 1995:652– 667.
40. Phipatanakul CS, Slavin RG. Use of human nasal airway mucosa and sam- 66. Roithmann R, Chapnik J, Zasmel N, et
thermography in clinical allergy. J Al- ples its surface exudations/secretions. al. Acoustic rhinometric assessment of
lergy Clin Immunol 1972;50:264 –275. Clin Exp Allergy 1990;20:253–259. the nasal valve. Am J Rhinol 1997;11:
41. Jankowski W, Bednarski W, 55. Pelikan Z, Feenstra L, Barree GO. Re- 379 –385.
Mikulewicz W. Measurement of the sponse of the nasal mucosa to allergen 67. Taylor G, MacNeil AR, Frud DLJ. As-
pH of the mucosa in allergic rhinitis in challenge measured by two different sessing degree of nasal patency by
children. Otolaryngol Pol 1969;23: methods of rhinomanometry. Ann Al- measuring peak expiratory flow rate
493– 498. lergy 1977;38:263–267. through the nose. J Allergy Clin Im-
42. Stankiewicz J, Ruta U, Gjorski P. La- 56. Saito H, Asakura K, Ogasawara H. munol 1973;52:193–198.
tex allergy. Int J Occup Med Environ Topical antigen provocation increases 68. Davies RJ, Corrado OJ. Diagnostic
Health 1995;8:139 –148. the number of immunoreactive IL-4-, tests– challenge tests: oral, nasal and
43. Jeney EV, Raphael GD, Meredith SD, IL-5- and IL-6-positive cells in the na- bronchial. In: Lessof MH, ed. Allergy:
Kaliner MA. Abnormal cholinergic sal mucosa of patients with perennial Immunological and Clinical Aspects.
parasympathetic responsiveness in the allergic rhinitis. Int Arch Allergy Im- London: Wiley & Sons, 1984;83–105.
nasal mucosa of patients with recurrent munol 1997;114:81– 85. 69. Eccles R. Rhinomanometry and nasal
sinusitis. J Allergy Clin Immunol 57. Phillips MJ, Ollier S, Davies RJ. Use challenge. In: Mackay Ian, ed.
1990;86:10 –18. of anterior rhinomanometry in nasal Rhinitis: Mechanisms and Manage-
44. Druce H.M, Schumacher M.J. Nasal provocation challenges with allergen ment. London: Royal Society of Med-
provocation challenge. J Allergy Clin and evaluation of the effects of keto- icine Services, 1989;53– 67.
Immunol 1990;86:261–264. tifen, clemastine and sodium cromo- 70. Clement PA. Committee report on
45. Baki A, Ucar B. Diagnostic value of glycate on these responses. Respiration standardization of rhinomanometry.
the nasal provocation test with Der- 1980;39(Suppl):26 –31. Rhinology 1984;22:151–155.
matophagoides pteronyssinus in child- 58. Druce HM. Nasal provocation 71. Lenders H, Pirsig W. Diagnostic value
hood asthma. Allergy 1995;50: challenge–strategies for experimental of acoustic rhinometry: patients with
751–754. design. Ann Allergy 1988;60: allergic and vasomotor rhinitis com-
46. Cirla AM, Sforza N, Roffi GP, et al. 191–195. pared to normal controls. Rhinology
Preseasonal intranasal immunotherapy 59. Naclerio RM, Meier HI, Kagey- 1990;28:5–16.
in birch-alder allergic rhinitis. A dou- Sobotka A, et al. Mediator release after 72. Druce HM, Bonner RF, Patow C, et al.
ble-blind study. Allergy 1996;51: nasal airway challenge with allergen. Response of nasal blood flow to neu-
299 –305. Am Rev Respir Dis 1983;128: rohormones as measured by laser-
47. Salzano FA. Specific nasal provoca- 597– 602. Doppler velocimetry. J Appl Physiol
tion test with powder allergen. Allergy 60. Baraniuk JN, Bolick M, Buckley CE. 1984;57:1276 –1283.
1997;52(Suppl):32–35. Pollen grain column chromatography: 73. Olson P. A comparison between the
48. Stanaland BE, Fernandez-Caldas E, A novel method for separation of pol- Xe133 washout and laser-Doppler
Jacinto CM, et al. Positive nasal chal- len wall solutes. Ann Botany 1990;66: techniques for estimation of nasal mu-
lenge responses to Blomia tropicalis. J 321–329. cosal blood flow in humans. Acta Oto-
Allergy Clin Immunol 1996;97: 61. Okuda M. Basic study of nasal provoc- laryngol 1986;102:106 –112.
1045–1049. ative test first report: side, site of the 74. Konno A, Togawa K, Nishira S. Par-
49. Small P, Barret D. Evaluation of dust nose, size of site and allergen amount. ticipation of vascular reflexes in mu-
and mite nasal provocation. Ann Al- Arch Otorhinolaryngol 1977;214: cosal swelling in nasal allergy. Acta
VOLUME 86, APRIL, 2001 363
Otolaryngol 1982;94:131–140. mucosa for morphological and bio- cous membranes. Analysis of bradyki-
75. Naclerio R, Togias A, Flowers B, et al. chemical analysis. Eur Respir J 1988; nin binding site distribution and secre-
Nasal lavage: a technique for elucidat- 1:856 – 862. tory responses in vitro and in vivo. Am
ing the pathophysiology of allergic rhi- 84. Meltzer E, Jalowayski A. Nasal cytol- Rev Respir Dis 1990;141:706 –714.
nitis. In: Mygind N, Pipkorn U, Dahl ogy in clinical practice. Am J Rhinol 94. Riccio MM, Proud D. Evidence that
R, eds. Rhinitis and Asthma: Similar- 1988;2:47–54. enhanced nasal reactivity to bradyki-
ities and Differences. Copenhagen: 85. Naclerio R. Clinical manifestations of nin in patients with symptomatic al-
Munksgaard, 1990;213–222. the release of histamine and other in- lergy is mediated by neural reflexes.
76. Raphael GD, Druce HM, Baraniuk JN, flammatory mediators. J Allergy Clin J All Clin Immunol 1996;97:1252–
Kaliner MA. Pathophysiology of rhi- Immunol 1999;103:S382—S385. 1263.
nitis. 1. Assessment of the sources of 86. Christodoulopoulos P, Cameron L, 95. Togias A, Naclerio RM, Proud D, et al.
protein in methacholine-induced nasal Durham S, Hamid Q. Molecular pa- Nasal challenge with cold dry air re-
secretions. Am Rev Respir Dis 1988; thology of allergic disease. II: Upper sults in release of inflammatory medi-
138:413– 420. airway disease. J Allergy Clin Immu- ators, possible involvement of mast
77. Bisgaard H, Krogsgaard OW, Mygind nol 2000;105:211–223. cells. J Clin Invest 1985;76:
N. Measurement of secretion in nasal 87. Clement PA, Stoop AP, Kaufmann L. 1375–1381.
lavage. Clin Sci (Colch) 1987;73: Histamine threshold and nasal hyper- 96. Drettner B. Vascular reactions of
217–222. reactivity in nonspecific allergic rhi- the human nasal mucosa on exposure
78. Linder A, Strandberg K, Deuschl H. nopathy. Rhinology 1985;23:35– 42. to cold. Acta Otolaryngol 1961;
Histamine concentrations in nasal se- 88. Gerth van Wijk RG. Nasal hyperreac- (Suppl)166:1– 83.
cretion and secretory activity in aller- tivity. Thesis, Erasmus University, 97. Andersson S. Recent advances in the
gic rhinitis. Allergy 1987;42:126 –134. Rotterdam, 1991. understanding of exercise-induced
79. Kaulbach HC, White MV, Igarashi Y, 89. Baraniuk JN. Neuropeptides. Am J asthma. Eur Respir Dis 1983;
et al. Estimation of nasal epithelial lin- Rhinol 1998;12:9 –16. (Suppl)128:225–236.
ing fluid using urea as a marker. J 90. Borum P. Nasal methacholine chal- 98. Silber G, Proud D, Warner J, et al. In
Allergy Clin Immunol 1993;92: lenge, a test for the measurement of vivo release of inflammatory media-
457– 465. nasal reactivity. J Allergy Clin Immu- tors by hyperosmolar solutions. Am
80. Baroody FM. Mucosal cytology. In: nol 1979;63:253–257. Rev Respir Dis 1988;137:606 – 612.
McCaffrey TV, ed. Rhinology and 91. Stjarne P, Lundblad L, Lundberg JM, 99. Patriarca G, Nucera E, DiRienzo V, et
Sinusology: Rhinologic Diagnosis and Anggard A. Capsaicin and nicotine al. Nasal provocation test with lysine
sensitive afferent neurones and nasal acetylsalicylate in aspirin-sensitive pa-
Treatment. Thieme, NY: 1997:
tients. Ann Allergy 1991;67:60 – 62.
175–192. secretion in healthy human volunteers
81. Whelan CF. Problems in examination and in patients with vasomotor rhinitis.
of nasal smears in allergic rhinitis. J Br J Pharmacol 1989;96:693–701. Requests for reprints should be addressed to:
Laryngol Otol 1980;84:399 – 404. 92. Blom HM, Van Rijswijk JB, Garrelds James N. Baraniuk, MD
82. Pipkorn U, Karlsson G, Enerback L. A IM, et al. Intranasal capsaicin is effi- Division of Rheumatology, Immunology, and
brush method to harvest cells from the cacious in non-allergic, non-infectious Allergy
nasal mucosa for microscopic and bio- perennial rhinitis. A placebo-con- Lower Level Gorman Building
chemical analysis. J Immunol Methods trolled study. Clin Exp Allergy 1997; 3800 Reservoir Road, NW
1988;112:37– 42. 27:796 – 801. Georgetown University, Washington, DC
83. Pipkorn U, Karlsson G. Methods for 93. Baraniuk JN, Lundgren JD, Mizoguchi 20007-2197
obtaining specimens from the nasal H, et al. Bradykinin respiratory mu- E-mail: baraniuj@gunet.georgetown.edu
CME Examination
1–5, Baraniuk JN and Lityakova LI. 2001;86:355–365
CME Test Questions c. To identify a novel allergen 2. Which of the following is NOT an
causing allergic rhinitis absolute contraindication for
1. Indications for the use of NPT in NPT?
clinical practice include all of the d. To confirm nasal reactivity to
allergen before starting immu- a. Acute period of allergic rhinitis
following EXCEPT:
a. To confirm the role of allergen in notherapy b. Mild asthma in remission
cases of disagreement of pa- e. To prove the allergic nature c. Previous anaphylactic reaction
tient’s history and skin testing of asthma when correspond- to an allergen
and/or RAST ing bronchial allergen provo- d. Acute viral or bacterial rhinitis
b. For the diagnosis of occupa- cation tests are postivie and sinusitis
tional allergic rhinitis e. Pregnancy
364 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
3. Which of these statements is patients with restricted lung ca- a. NPT is a well standardized
false? pacity (TLC ⬍60%) method and is frequently used
a. NPT can be done 4 weeks after 4. A positive NPT is determined by: in clinical practice in the
the episode of allergic or infec- a. The maximum allergen dose United States
tious rhinitis that patient received b. NPT has shown promise for the
b. Polyps, atrophic rhinitis, and b. Self-report scoring of clinical diagnosis of allergic and occu-
deviated nasal septum are ab- symptoms pational rhinits
solute contraindications for c. 10-cm linear visual analog c. The analysis of mechanisms of
NPT scales of symptoms NPT responses may lead to a
c. NPT can be done 6 weeks after d. Measures of nasal patency more appropriate and focused
nasal or sinus surgery e. The assessment of clinical therapy
d. Nasal congestion can result symptoms scores, nasal secre- d. There is a wide variety of NPT
from oral contraceptives and tion, and nasal patency mea- test techniques for research
preparations containing sulfite surements e. NPT provides useful informa-
preservatives 5. Which of these statements is tion about the pathogenesis of
e. NPT should not be done in false? airway diseases
Answers found on page 386.
VOLUME 86, APRIL, 2001 365
You might also like
- Incident ReportDocument3 pagesIncident Reportthuynh12No ratings yet
- Diagnosing ADHD in Adults with Intellectual DisabilitiesDocument20 pagesDiagnosing ADHD in Adults with Intellectual DisabilitiesEspíritu Ciudadano92% (26)
- Medical word association and formation exercisesDocument50 pagesMedical word association and formation exercisesMarius Belean100% (1)
- Ajay YadavDocument351 pagesAjay YadavTabish Javaid90% (10)
- Ethical Issues in Geriatrics A Guide For CliniciansDocument9 pagesEthical Issues in Geriatrics A Guide For CliniciansThanc FishNo ratings yet
- Immunotherapy in AsthmaDocument125 pagesImmunotherapy in Asthmarizwanas100% (1)
- Diabetes Urdu OnDocument35 pagesDiabetes Urdu OnShahid AminNo ratings yet
- Pantoprazole Drug StudyDocument1 pagePantoprazole Drug StudyNone Bb100% (2)
- 2018.surgery Intestinal Obstruction in Infants and ChildrenDocument11 pages2018.surgery Intestinal Obstruction in Infants and ChildrenFranz SalazarNo ratings yet
- Nassal Provocation Test - 2Document5 pagesNassal Provocation Test - 2Lengkung BajaNo ratings yet
- Nassal Provocation Test - 6Document5 pagesNassal Provocation Test - 6Lengkung BajaNo ratings yet
- Allergen-Specifi C Nasal Provocation Testing: Review by The Rhinoconjunctivitis Committee of The Spanish Society of Allergy and Clinical ImmunologyDocument12 pagesAllergen-Specifi C Nasal Provocation Testing: Review by The Rhinoconjunctivitis Committee of The Spanish Society of Allergy and Clinical ImmunologyRian Permana PNo ratings yet
- Evidence-Based SLIT Benefits for Allergic RhinitisDocument10 pagesEvidence-Based SLIT Benefits for Allergic RhinitisPeter SalimNo ratings yet
- Diagnosing Rhinitis: Allergic vs. Nonallergic: David M. Quillen, M.D., and David B. Feller, M.DDocument8 pagesDiagnosing Rhinitis: Allergic vs. Nonallergic: David M. Quillen, M.D., and David B. Feller, M.DLia Mbag LiaNo ratings yet
- Allergic Rhinitis - StatPearls - NCBI BookshelfDocument9 pagesAllergic Rhinitis - StatPearls - NCBI BookshelfIndra kusuma mardiaNo ratings yet
- Inflamación Por Inhaladores de Corticosteroides en La Faringe de AsmáticosDocument7 pagesInflamación Por Inhaladores de Corticosteroides en La Faringe de AsmáticosEstefani Romero ArriagadaNo ratings yet
- 4 PDFDocument9 pages4 PDFAdan MorenoNo ratings yet
- CPG On Allergic Rhinitis 2Document8 pagesCPG On Allergic Rhinitis 2mkct111No ratings yet
- Clinical and Experimental Allergy ReviewsDocument29 pagesClinical and Experimental Allergy ReviewsSinta DarmaNo ratings yet
- NIH Public Access: Author ManuscriptDocument9 pagesNIH Public Access: Author Manuscriptimmortally89No ratings yet
- Johnson 2004Document9 pagesJohnson 2004Abdul Wahab 2008126345No ratings yet
- Nassal Provocation Test - 1Document5 pagesNassal Provocation Test - 1Lengkung BajaNo ratings yet
- Nasal Provocation Test in The Diagnosis of Allergic RhinitisDocument31 pagesNasal Provocation Test in The Diagnosis of Allergic RhinitisValentina AdindaNo ratings yet
- Alergic Desease PRACTALL-consensusDocument12 pagesAlergic Desease PRACTALL-consensusNaty FernandezNo ratings yet
- Vol28issue4 1Document17 pagesVol28issue4 1BTS LGONo ratings yet
- 011AADocument8 pages011AAAtef AlbooqNo ratings yet
- Respiratory ResearchDocument8 pagesRespiratory ResearchStacey BakerNo ratings yet
- HHS Public Access: The Pathophysiology of AnaphylaxisDocument29 pagesHHS Public Access: The Pathophysiology of AnaphylaxisdilaNo ratings yet
- Futurehorizonsinallergy: Michael J. Marino,, Amber U. LuongDocument9 pagesFuturehorizonsinallergy: Michael J. Marino,, Amber U. Luongmadhumitha srinivasNo ratings yet
- Occupational Rhinitis: Making The Diagnosis: by Mélanie Duval, MD and Martin Desrosiers, MD, FRCSCDocument4 pagesOccupational Rhinitis: Making The Diagnosis: by Mélanie Duval, MD and Martin Desrosiers, MD, FRCSCMelanie DuvalNo ratings yet
- Allergic Rhinitis 2011Document9 pagesAllergic Rhinitis 2011SheinGervacioErnacioNo ratings yet
- Ciprandi1997 PDFDocument5 pagesCiprandi1997 PDFTamaz GugeshashviliNo ratings yet
- A Guideline To Local Anestetic Alergy TestingDocument7 pagesA Guideline To Local Anestetic Alergy TestingKomal GuptaNo ratings yet
- Suspected Allergy To Local AnaestheticsDocument7 pagesSuspected Allergy To Local AnaestheticsIvette M. Carroll D.No ratings yet
- asthmaDocument3 pagesasthmanaomimarielleNo ratings yet
- World Allergy OrganizationDocument25 pagesWorld Allergy OrganizationHusnul HanifaNo ratings yet
- Epidemiology and Clinical Predictors of Biphasic Reactions in Children With AnaphylaxisDocument9 pagesEpidemiology and Clinical Predictors of Biphasic Reactions in Children With AnaphylaxisPrihanant BayuNo ratings yet
- IgE Allergy Testing World Allergy Position PaperDocument50 pagesIgE Allergy Testing World Allergy Position PaperAlfred AlfredNo ratings yet
- Golden 2021Document7 pagesGolden 2021jasanchez8No ratings yet
- Allergic Bronchopulmonary Aspergillosis: AAAAI Committee ReportDocument6 pagesAllergic Bronchopulmonary Aspergillosis: AAAAI Committee ReportChristian Andrés CasasNo ratings yet
- Anaphylaxis Diagnosis, TreatmentDocument6 pagesAnaphylaxis Diagnosis, TreatmentutifornaNo ratings yet
- Japanese Guidelines For Childhood Asthma 2017 PDFDocument15 pagesJapanese Guidelines For Childhood Asthma 2017 PDFcindy315No ratings yet
- Allergic Rhinitis Slides 070926 PDFDocument57 pagesAllergic Rhinitis Slides 070926 PDFmhamad kabraNo ratings yet
- Dental Anaphylaxis Knowledge SurveyDocument3 pagesDental Anaphylaxis Knowledge SurveyDiego melo limaNo ratings yet
- Current Management of Anaphylaxis: A FT BrownDocument12 pagesCurrent Management of Anaphylaxis: A FT BrowndoctorniravNo ratings yet
- Cardona Et Al 2018 AllergyDocument5 pagesCardona Et Al 2018 AllergydregleavNo ratings yet
- Clinical and Experimental Allergy: BSACI Guidelines For The Management of Drug AllergyDocument19 pagesClinical and Experimental Allergy: BSACI Guidelines For The Management of Drug AllergyJair Edu100% (1)
- Guia - 4209 Guia Rinitis AlergicaDocument16 pagesGuia - 4209 Guia Rinitis AlergicaJesus Manuel Armenta VelderrainNo ratings yet
- 12erny (Full Permission)Document15 pages12erny (Full Permission)Peter SalimNo ratings yet
- Aspirin-Exacerbated Respiratory Disease With Allergic Fungal Rhinosinusitis: A Case Series of Overlapping Sinonasal EndotypesDocument6 pagesAspirin-Exacerbated Respiratory Disease With Allergic Fungal Rhinosinusitis: A Case Series of Overlapping Sinonasal EndotypesLee제노No ratings yet
- 2739 PDFDocument2 pages2739 PDFSeptya widhiafniNo ratings yet
- World Allergy Organization JournalDocument8 pagesWorld Allergy Organization JournalUlayya Ghina NabillaNo ratings yet
- Allergie of Profile NasalPolyposisDocument7 pagesAllergie of Profile NasalPolyposisAlsyahrin Manggala PutraNo ratings yet
- 2006 AllergyDocument9 pages2006 AllergyJUAN BENITO SUAREZ PALACIOSNo ratings yet
- 10 1016@j Aller 2012 08 004Document8 pages10 1016@j Aller 2012 08 004Muhammad FakhrizalNo ratings yet
- Anaphylaxis: Review Open AccessDocument7 pagesAnaphylaxis: Review Open AccessRadyaAgriNo ratings yet
- Allergen Immunotherapy: A Guide to Types, Diagnosis, and PrognosisDocument8 pagesAllergen Immunotherapy: A Guide to Types, Diagnosis, and Prognosisjb cookiesNo ratings yet
- Dissertation Allergic RhinitisDocument8 pagesDissertation Allergic RhinitisWritingPaperServicesReno100% (1)
- Pi Is 0091674915021764Document1 pagePi Is 0091674915021764nanonanditoNo ratings yet
- Allergy Prevalence and Symptom Score CorrelationDocument7 pagesAllergy Prevalence and Symptom Score CorrelationzariaNo ratings yet
- Tsabouri 2014Document10 pagesTsabouri 2014Goesti YudistiraNo ratings yet
- GavaertDocument8 pagesGavaertstanleyNo ratings yet
- Recommendations For Appropriate Sublingual Immunotherapy Clinical TrialsDocument6 pagesRecommendations For Appropriate Sublingual Immunotherapy Clinical TrialstitatNo ratings yet
- Best Practice & Research Clinical Anaesthesiology: Contents Lists Available atDocument15 pagesBest Practice & Research Clinical Anaesthesiology: Contents Lists Available atPedro SalamancaNo ratings yet
- Sinonasal Disease: An Underappreciated EntityDocument2 pagesSinonasal Disease: An Underappreciated EntityLee제노No ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Pengpid, S., & Peltzer, K. (2018) - Utilization of Traditional and Complementary Medicine in IndonesiaDocument8 pagesPengpid, S., & Peltzer, K. (2018) - Utilization of Traditional and Complementary Medicine in IndonesiaLengkung BajaNo ratings yet
- New Perspective On The Resilience of SMEsDocument11 pagesNew Perspective On The Resilience of SMEsLengkung BajaNo ratings yet
- Priorities for Ecuadorian SMEs in the Post-COVID EraDocument9 pagesPriorities for Ecuadorian SMEs in the Post-COVID EraLengkung BajaNo ratings yet
- A Survival Analysis of Small and Medium Enterprises (Smes) in Central China and Their DeterminantsDocument17 pagesA Survival Analysis of Small and Medium Enterprises (Smes) in Central China and Their DeterminantsLengkung BajaNo ratings yet
- Epidemiological Characterization of Dermatomycosis in EthiopiaDocument7 pagesEpidemiological Characterization of Dermatomycosis in EthiopiaMini LaksmiNo ratings yet
- Occular Manifestations in Systemic DiseaseDocument42 pagesOccular Manifestations in Systemic DiseasekhalidNo ratings yet
- Anaesthesiology Case (Kaarthigan)Document36 pagesAnaesthesiology Case (Kaarthigan)Kaarthigan RamaiahNo ratings yet
- Hemant Surgical Double Lumen CathetersDocument2 pagesHemant Surgical Double Lumen CathetersKaushik Hanskumar ShahNo ratings yet
- Lucy Mayienga CV RecentDocument3 pagesLucy Mayienga CV Recentlucy.mayiengaNo ratings yet
- Quiet Time For Patients in Acute CareDocument24 pagesQuiet Time For Patients in Acute Careapi-354868439No ratings yet
- IntroductionDocument13 pagesIntroductionSaadNo ratings yet
- Neonatal Neuro ExamDocument13 pagesNeonatal Neuro ExamLisa SariNo ratings yet
- Urinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Document9 pagesUrinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Franz goNo ratings yet
- Understanding the Physiology of ShockDocument77 pagesUnderstanding the Physiology of ShocklupckyNo ratings yet
- Personal Hygiene for ChildrenDocument2 pagesPersonal Hygiene for ChildrenDonna Mae BoolNo ratings yet
- Hospital La Comunidad de Santa Rosa: Chapter I: Problem and Its SettingsDocument15 pagesHospital La Comunidad de Santa Rosa: Chapter I: Problem and Its SettingsMeynard MagsinoNo ratings yet
- Hughes Selection of Remedy PDFDocument47 pagesHughes Selection of Remedy PDFNavya VaddimukkalaNo ratings yet
- Birth Control Made Simple 2010Document5 pagesBirth Control Made Simple 2010Richard WahlNo ratings yet
- In-Flight Emergencies - Legal Implications For Medical Professionals by Dr. Marc PhuaDocument17 pagesIn-Flight Emergencies - Legal Implications For Medical Professionals by Dr. Marc PhuaMarcus PhuaNo ratings yet
- Alloderm - Breast ReconstructionDocument180 pagesAlloderm - Breast ReconstructionFlorina PopaNo ratings yet
- Malaria DR TariqDocument32 pagesMalaria DR Tariqdr_hammadNo ratings yet
- CPD Accredited ActivitiesDocument25 pagesCPD Accredited ActivitiesJancor Diagnostics Drug Testing LaboratoryNo ratings yet
- Complications of Bariatric Surgery Dumping Syndrome Reflux and Vitamin Deficiencies 2014 Best Practice Research Clinical GastroenterologyDocument10 pagesComplications of Bariatric Surgery Dumping Syndrome Reflux and Vitamin Deficiencies 2014 Best Practice Research Clinical GastroenterologyYipno Wanhar El MawardiNo ratings yet
- Anti PsychotisDocument21 pagesAnti Psychotissuresh sataguniNo ratings yet
- Community Case Serhat KokenDocument12 pagesCommunity Case Serhat Kokenmaroun ghalebNo ratings yet