You might also like
- Handouts Psych Prof. AlvizDocument2 pagesHandouts Psych Prof. AlvizKristine QuindozaNo ratings yet
- Nursing Leadership, Management and Research Competency AppraisalDocument2 pagesNursing Leadership, Management and Research Competency AppraisalCharissa Magistrado De LeonNo ratings yet
- Case FormatDocument16 pagesCase FormatDr.Akshata ShriyanNo ratings yet
- Emergency Cardiac Medications for ArrhythmiasDocument14 pagesEmergency Cardiac Medications for ArrhythmiasRomzy BasañesNo ratings yet
- Ob Ward Rle Drug StudyDocument3 pagesOb Ward Rle Drug StudyArisza Shane B.No ratings yet
- CHN TopicsDocument19 pagesCHN TopicsKristine AnaenNo ratings yet
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers andDocument12 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers andZyntrx VillasNo ratings yet
- NCM 119 Assignment Galutan Kimberly Erika FDocument5 pagesNCM 119 Assignment Galutan Kimberly Erika Faaron tabernaNo ratings yet
- OrchiectomyDocument35 pagesOrchiectomyYosa Angga OktamaNo ratings yet
- UNIT 1 (MS 1) Care of Clients With Problems in OxygenationDocument10 pagesUNIT 1 (MS 1) Care of Clients With Problems in OxygenationElle MirandaNo ratings yet
- Professional AdjustmentDocument22 pagesProfessional AdjustmentArgee Alonsabe100% (1)
- Guiding Environmentally Safe Nursing CareDocument7 pagesGuiding Environmentally Safe Nursing CarepauchanmnlNo ratings yet
- Fluid Volume Deficit and Excess: Types, Causes, Signs and Nursing ManagementDocument32 pagesFluid Volume Deficit and Excess: Types, Causes, Signs and Nursing ManagementAcohCChaoNo ratings yet
- Page 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Document3 pagesPage 17 ACUTE PAIN Related To Joint Stiffness Secondary To Aging.Senyorita KHayeNo ratings yet
- 31 Therapeutic Communication Techniques With Elderly and Children2Document42 pages31 Therapeutic Communication Techniques With Elderly and Children2Ab Staholic BoiiNo ratings yet
- Film Analysis: in Health Care Ethics (NR-NUR127)Document5 pagesFilm Analysis: in Health Care Ethics (NR-NUR127)John MagtibayNo ratings yet
- Geria Lec Portfolio CasiaDocument9 pagesGeria Lec Portfolio CasiaMarie Ashley CasiaNo ratings yet
- Nursing Care Plan for a Male Patient with Pleural EffusionDocument48 pagesNursing Care Plan for a Male Patient with Pleural EffusionNo EulNo ratings yet
- Phases of The COPAR ProcessDocument8 pagesPhases of The COPAR ProcessmerlNo ratings yet
- Nursing Care Plan For Subarachnoid HemorrhagicDocument2 pagesNursing Care Plan For Subarachnoid HemorrhagicAshram Smart100% (1)
- MnemonicsDocument10 pagesMnemonicsRichard GarciaNo ratings yet
- Handout # 10Document22 pagesHandout # 10Ram August100% (1)
- VerA Ok-Prelim Ncm104 (Autosaved) VeraDocument30 pagesVerA Ok-Prelim Ncm104 (Autosaved) Verajesperdomincilbayaua100% (1)
- MS NeuroDocument28 pagesMS NeuroFrechel Ann Landingin PedrozoNo ratings yet
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitRainier IbarretaNo ratings yet
- High-Risk Pregnancy Factors & CareDocument19 pagesHigh-Risk Pregnancy Factors & CareRoger Jr PumarenNo ratings yet
- Pneumonia AnswersDocument5 pagesPneumonia AnswersColeen Mae CamaristaNo ratings yet
- Electrolyte ImbalanceDocument4 pagesElectrolyte ImbalanceDoneva Lyn MedinaNo ratings yet
- Physical Evaluation Checklist For NurseDocument3 pagesPhysical Evaluation Checklist For NurseGiridhar RagavasimhanNo ratings yet
- Nursing Care for Mr. X with Benign Prostatic HyperplasiaDocument4 pagesNursing Care for Mr. X with Benign Prostatic HyperplasiaHafin WardanaNo ratings yet
- Diet: Bath: ActivityDocument2 pagesDiet: Bath: ActivityKristian Karl Bautista Kiw-isNo ratings yet
- Care For Patients With Alteration in Perception and CoordinationDocument12 pagesCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- Ct7 Fluid, Electrolyte ImbalanceDocument9 pagesCt7 Fluid, Electrolyte ImbalanceAlondra VelascoNo ratings yet
- Patient with Cellulitis Right Arm ReportDocument1 pagePatient with Cellulitis Right Arm ReportJhevilin RMNo ratings yet
- Availability: Classifications: Antihistamine Antipruritic Pregnancy Category: CDocument4 pagesAvailability: Classifications: Antihistamine Antipruritic Pregnancy Category: CCay SevillaNo ratings yet
- Jake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersDocument8 pagesJake Yvan Dizon Case Study, Chapter 49, Assessment and Management of Patients With Hepatic DisordersJake Yvan DizonNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- Post Test - Neuro - Dr. Arreglo (SC)Document2 pagesPost Test - Neuro - Dr. Arreglo (SC)Kristen FajilanNo ratings yet
- Postpartum ExaminationDocument10 pagesPostpartum ExaminationKrystelle Jade LabineNo ratings yet
- Handouts Renal Fabs Ucu InhouseDocument42 pagesHandouts Renal Fabs Ucu Inhousejon elleNo ratings yet
- Roles and Functions of the Community Health NurseDocument4 pagesRoles and Functions of the Community Health NurseDanz Kie100% (1)
- Futuristic Change-Oriented Continuous Dynamic Process Flexible Systemic ProcessDocument3 pagesFuturistic Change-Oriented Continuous Dynamic Process Flexible Systemic ProcessCharlene GonzalesNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- MS TEST-QUESTIONAIRE 2: Nursing Assessment and PrioritizationDocument24 pagesMS TEST-QUESTIONAIRE 2: Nursing Assessment and PrioritizationJackie AbarraNo ratings yet
- Nursing Interview Guide To Collect Subjective Data From The Client Questions RationaleDocument19 pagesNursing Interview Guide To Collect Subjective Data From The Client Questions RationaleKent Rebong100% (1)
- Orientation On Community Health - Doh Programs & ServicesDocument11 pagesOrientation On Community Health - Doh Programs & ServicesAudrey Beatrice ReyesNo ratings yet
- Republic Act 9173 Philippine Nursing Act of 2002: Why We Have RA 9173?Document7 pagesRepublic Act 9173 Philippine Nursing Act of 2002: Why We Have RA 9173?czeremar chan100% (1)
- NCPDocument2 pagesNCPMelissa David100% (1)
- GRP 4 CLO 2 Concept Map PT 1 PDFDocument14 pagesGRP 4 CLO 2 Concept Map PT 1 PDFMaria Lyn Ocariza ArandiaNo ratings yet
- Nursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionDocument2 pagesNursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionTammy De GuzmanNo ratings yet
- Pleural Effusion: Bukidnon State University City of MalaybalayDocument49 pagesPleural Effusion: Bukidnon State University City of MalaybalayKarima JonesNo ratings yet
- Lab 5 Diabetes InsipidusDocument6 pagesLab 5 Diabetes InsipidusLisa EkapratiwiNo ratings yet
- Activity 2Document7 pagesActivity 2Karen T. CeletariaNo ratings yet
- Omeprazole Nursing ConsiderationsDocument9 pagesOmeprazole Nursing ConsiderationsVanessa Naomi GalidoNo ratings yet
- Neuro - Sir Chavez - AS OF 12PMDocument5 pagesNeuro - Sir Chavez - AS OF 12PMCarl JustineNo ratings yet
- CetirizineDocument2 pagesCetirizinelintangNo ratings yet
- Case Study, Chapter 70, Management of Patients WithOncologic or Degenerative Neurologic DisordersDocument1 pageCase Study, Chapter 70, Management of Patients WithOncologic or Degenerative Neurologic Disordersclyde i am100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 4 Assessment of The Female GenitaliaDocument31 pages4 Assessment of The Female GenitaliaJae TyNo ratings yet
- 1 Skin Hair Nails SCRIPTDocument7 pages1 Skin Hair Nails SCRIPTJae Ty100% (1)
- Assessing Male GenitaliaDocument8 pagesAssessing Male GenitaliaJae TyNo ratings yet
- Abdomen, Musculoskeletal, NeurologicalDocument179 pagesAbdomen, Musculoskeletal, NeurologicalJae TyNo ratings yet
- ENDORCRINE SYSTEM - Review Anaphy NotesDocument10 pagesENDORCRINE SYSTEM - Review Anaphy NotesJae TyNo ratings yet
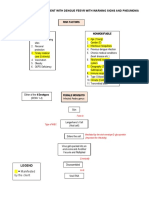
- Schematic diagram of dengue fever patient with warning signs and pneumonia risk factorsDocument4 pagesSchematic diagram of dengue fever patient with warning signs and pneumonia risk factorsJae TyNo ratings yet
- College Nursing Drug RecordDocument12 pagesCollege Nursing Drug RecordJae TyNo ratings yet
- The Nursing Care of A Family With A NewbornDocument5 pagesThe Nursing Care of A Family With A NewbornDonell EscalanteNo ratings yet
- Fetal SkullDocument4 pagesFetal SkullSherene Jacob Mathew VaidyanNo ratings yet
- Abnormal Fontanel PDFDocument6 pagesAbnormal Fontanel PDFMithlesh DewanganNo ratings yet
- Advanced Pediatric AssessmentDocument582 pagesAdvanced Pediatric AssessmentBenjamin Gabriel100% (1)
- Neonatal Cranial Ultrasonography: Third EditionDocument344 pagesNeonatal Cranial Ultrasonography: Third EditionTsega Hagos100% (3)
- Open Fontanel in A ChildDocument9 pagesOpen Fontanel in A ChildAmjad JoharNo ratings yet
- Newborn Assessment: IntroductionDocument16 pagesNewborn Assessment: Introductionsandeepv080% (1)
- Newborn AssessDocument19 pagesNewborn AssessMeredith Carroll McSwainNo ratings yet
- Newborn Appraisal BenitaDocument172 pagesNewborn Appraisal BenitaBenudavid David100% (2)
- Characteristics and Vital Signs of the Newborn InfantDocument102 pagesCharacteristics and Vital Signs of the Newborn InfantSusan HepziNo ratings yet
- B2nursing Care of A Family With A Newborn Part 2BDocument44 pagesB2nursing Care of A Family With A Newborn Part 2BJustine Jean GuillermoNo ratings yet
- FETAL Skull For Undergrad 3980962Document88 pagesFETAL Skull For Undergrad 3980962Sheela VictorNo ratings yet
- Unit 2 Blue BoxesDocument19 pagesUnit 2 Blue Boxesstarblue265100% (1)
- Fronto-Ethmoidal Meningoencephalocele: A Case Report: TAF. Benitaryani, PD. UtomoDocument1 pageFronto-Ethmoidal Meningoencephalocele: A Case Report: TAF. Benitaryani, PD. UtomotrifoniastriNo ratings yet
- Newborn AssessmentDocument12 pagesNewborn AssessmentstellaclarkNo ratings yet
- 2 Introduction To Embryology and FetalDocument55 pages2 Introduction To Embryology and Fetaldemeke andebetNo ratings yet
- Anterior Fontanel Size: Sarla Mattur Ram Kumar G.P. Mathur V.K. Singh Veena Gupta V.N. Tripathi Material and MethodsDocument4 pagesAnterior Fontanel Size: Sarla Mattur Ram Kumar G.P. Mathur V.K. Singh Veena Gupta V.N. Tripathi Material and MethodsrvsharmaNo ratings yet
- Normal Labor and DeliveryDocument46 pagesNormal Labor and DeliveryNen BandarNo ratings yet
- Newborn Assessment 2.16Document16 pagesNewborn Assessment 2.16rrbischofbergerNo ratings yet
- Newborn Care: A Newborn Baby or Animal Is One That Has Just Been BornDocument26 pagesNewborn Care: A Newborn Baby or Animal Is One That Has Just Been BornJenny-Vi Tegelan LandayanNo ratings yet
- Newborn Case StudyDocument16 pagesNewborn Case StudyErl Joy Montaño Cañete0% (1)
- Lossing BerylArbucklesCranial PDFDocument67 pagesLossing BerylArbucklesCranial PDFdeemoney3100% (1)
- Module NCM 107 Unit 6Document56 pagesModule NCM 107 Unit 6Gebriel Igdon TomarongNo ratings yet
- Fetal Skull DefinitionsDocument107 pagesFetal Skull DefinitionsBharat Thapa50% (2)
- 2 - Applied AnatomyDocument46 pages2 - Applied AnatomyKholoud KholoudNo ratings yet
- Procedure On New Born AssessmentDocument19 pagesProcedure On New Born AssessmentPriyaNo ratings yet
- what are cranial sutures - Google SearchDocument1 pagewhat are cranial sutures - Google Searchgiamaj4No ratings yet
- Ch18 Nursing Care of A Family With A NewbornDocument109 pagesCh18 Nursing Care of A Family With A NewbornKathleen Ang100% (1)
- Micro-Teaching Fetal SkullDocument26 pagesMicro-Teaching Fetal SkullDaily DoseNo ratings yet
- CHILD HEALTH NURSING: Growth and DevelopmentDocument67 pagesCHILD HEALTH NURSING: Growth and DevelopmentEllen Angel100% (3)