You might also like
- Before The Procedure: 1.using A Flowchart, Provide The Whole Procedure of Lumbar TapDocument2 pagesBefore The Procedure: 1.using A Flowchart, Provide The Whole Procedure of Lumbar TapColene MoresNo ratings yet
- Tryout Excuse Letter VballDocument8 pagesTryout Excuse Letter VballPatricia CaladoNo ratings yet
- Assignment in NCM 106 LectureDocument6 pagesAssignment in NCM 106 LectureJeanessa Delantar QuilisadioNo ratings yet
- Learning Objectives: Assessing For Passy Muir Speaking Valve and PO Candidacy in The Tracheostomized Patient PopulationDocument6 pagesLearning Objectives: Assessing For Passy Muir Speaking Valve and PO Candidacy in The Tracheostomized Patient Populationalfredo_dagondonNo ratings yet
- PALi 3rd 5th Year Notes 2011 Including Comm Skills PDFDocument49 pagesPALi 3rd 5th Year Notes 2011 Including Comm Skills PDFgus_lions100% (1)
- Endoscopy ChecklistDocument4 pagesEndoscopy Checklistdk15janNo ratings yet
- Skills Demo Guide For ClerksDocument11 pagesSkills Demo Guide For ClerksMariana B.No ratings yet
- Case StudyDocument8 pagesCase StudyKrisianne Mae Lorenzo FranciscoNo ratings yet
- Breast Lump History OSCE Guide Breast Cancer Geeky MedicsDocument1 pageBreast Lump History OSCE Guide Breast Cancer Geeky MedicsAnne Julia AgustinNo ratings yet
- Respi Hema NotesDocument16 pagesRespi Hema NotesLucky GomezNo ratings yet
- Clinical OSCE NotesDocument49 pagesClinical OSCE NotesYusri HarisNo ratings yet
- Upper Respiratory Tract Infection URTI - PPTX GROUP 2 BSN 3CDocument22 pagesUpper Respiratory Tract Infection URTI - PPTX GROUP 2 BSN 3CIren RamosoNo ratings yet
- DR Shahid Methods OriginalDocument31 pagesDR Shahid Methods OriginalHumna YounisNo ratings yet
- Urgical Afety Hecklist: Before Induction of Anaesthesia Before Skin Incision Before Patient Leaves Operating RoomDocument2 pagesUrgical Afety Hecklist: Before Induction of Anaesthesia Before Skin Incision Before Patient Leaves Operating RoomSyahri DzikriNo ratings yet
- Fine Needle Aspiration Cytology EDITEDDocument90 pagesFine Needle Aspiration Cytology EDITEDclaimstudent3515No ratings yet
- Checklist For Vaginal ExaminationDocument7 pagesChecklist For Vaginal ExaminationjoaguilarNo ratings yet
- PassPACES Respiratory ExaminationDocument4 pagesPassPACES Respiratory ExaminationIbrahim AbbassNo ratings yet
- RABE 2 ReviewerDocument9 pagesRABE 2 ReviewerHazel carrascalNo ratings yet
- LST 2009 Surgical Safety Check List (Australia and New Zealand) PDFDocument1 pageLST 2009 Surgical Safety Check List (Australia and New Zealand) PDFaskjhwiuehNo ratings yet
- Dmc-College Foundation Inc.: Sta. Filomena, Dipolog CityDocument9 pagesDmc-College Foundation Inc.: Sta. Filomena, Dipolog Cityviper79678No ratings yet
- Telehealth Physical Exam: Eyes Neck Chest SkinDocument1 pageTelehealth Physical Exam: Eyes Neck Chest SkinYazeed QadadhaNo ratings yet
- Procedure PARACENTASISDocument11 pagesProcedure PARACENTASISaparnaNo ratings yet
- Odette's Sonography Portfolio: Patient HistoryDocument2 pagesOdette's Sonography Portfolio: Patient Historyqditya nurNo ratings yet
- 2-Respiratory System Diagnostic TestsDocument4 pages2-Respiratory System Diagnostic TestsEllyza EvangelistaNo ratings yet
- Review of Systems For Current Health Problems (Health Assessment)Document5 pagesReview of Systems For Current Health Problems (Health Assessment)younggirldavid100% (1)
- Istory Taking Examination Symptomatology and Yurveda Treatment in NO Rectal PatientsDocument111 pagesIstory Taking Examination Symptomatology and Yurveda Treatment in NO Rectal Patientsyoga_kusmawanNo ratings yet
- Pediatric Resucitation Pediatric Resucitation: Pgi Gasataya, Charisse Ann G Pgi Tabobo, Raymee TDocument30 pagesPediatric Resucitation Pediatric Resucitation: Pgi Gasataya, Charisse Ann G Pgi Tabobo, Raymee TCharisse Ann GasatayaNo ratings yet
- It Is Time To Put Special Tests For Rotator Cuff Related Shoulder Pain Out To PastureDocument4 pagesIt Is Time To Put Special Tests For Rotator Cuff Related Shoulder Pain Out To PastureGarrett ZajicekNo ratings yet
- Cpga002 0Document4 pagesCpga002 0sakif sNo ratings yet
- Nursing English 1Document105 pagesNursing English 1Syufyan HanafiNo ratings yet
- Urinary CatheterizationDocument3 pagesUrinary CatheterizationbabyrainbowNo ratings yet
- Sequential Compression DeviceDocument2 pagesSequential Compression Deviceal-obinay shereen0% (1)
- Varicose Case ProformaDocument2 pagesVaricose Case ProformaSneha Naulakha100% (1)
- Checklist For Vaginal ExaminationDocument7 pagesChecklist For Vaginal ExaminationANGELYN TI-ADNo ratings yet
- Trauma Tumpul Abdomen: Stase Bedah Digestif Januari 2019Document49 pagesTrauma Tumpul Abdomen: Stase Bedah Digestif Januari 2019ArifHidayatNo ratings yet
- First Edition Surgical Safety ChecklistDocument1 pageFirst Edition Surgical Safety Checklistrraven16No ratings yet
- Final Surgical Long Case Collection by Classof2016 PMCDocument32 pagesFinal Surgical Long Case Collection by Classof2016 PMCStudentNo ratings yet
- Perioperative Nursing: Preoperative PhaseDocument5 pagesPerioperative Nursing: Preoperative PhaseanjieNo ratings yet
- Fine Needle Aspiration PDFDocument5 pagesFine Needle Aspiration PDFjkNo ratings yet
- Physical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingDocument101 pagesPhysical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingBinal JoshiNo ratings yet
- Preop EvaluationDocument3 pagesPreop EvaluationRhea JavierNo ratings yet
- Male RSDocument7 pagesMale RSpravina praviNo ratings yet
- Testicular Examination OSCE GuideDocument9 pagesTesticular Examination OSCE Guidecharlyn206No ratings yet
- Doc-20240131-Wa0 240131 224157Document4 pagesDoc-20240131-Wa0 240131 22415722alhumidi2020No ratings yet
- Position and DrapingDocument9 pagesPosition and DrapingairamaebarbaNo ratings yet
- Procedural Skill by NPDocument92 pagesProcedural Skill by NPsankethg93No ratings yet
- Companion For Obstetrics and Gynecology Practical Examination 16nbsped 9389776740 9789389776744 CompressDocument246 pagesCompanion For Obstetrics and Gynecology Practical Examination 16nbsped 9389776740 9789389776744 CompressMonil ShahNo ratings yet
- 5 PPH - Scenario 1Document4 pages5 PPH - Scenario 1mjgmhgfvNo ratings yet
- ARMAMENTARIUMDocument105 pagesARMAMENTARIUMchanaish6No ratings yet
- Skills Mods Check List For NasogastricDocument6 pagesSkills Mods Check List For Nasogastricpunam todkarNo ratings yet
- Resume Nasogastric Tube InstallationDocument17 pagesResume Nasogastric Tube InstallationRedmy LasmanaNo ratings yet
- ?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEDocument14 pages?1 - Chest X-Ray Interpretation - A Structured Approach - Radiology - OSCEVerónicaNo ratings yet
- NCP (Innefect B P, Mucus)Document5 pagesNCP (Innefect B P, Mucus)CG Patron BamboNo ratings yet
- Physical Assessment TemplateDocument9 pagesPhysical Assessment TemplateArky VessaliuzNo ratings yet
- NCM 207Document29 pagesNCM 207Iligan, JamaicahNo ratings yet
- CM TransDocument4 pagesCM TransPheniel ManansalaNo ratings yet
- Video Capsule EndosDocument3 pagesVideo Capsule EndosRobert GodeanuNo ratings yet
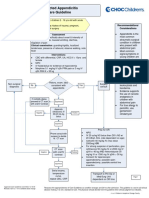
- Suspected Appendicitis Care GuidelineDocument3 pagesSuspected Appendicitis Care GuidelinetamiNo ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- Oral Path CramDocument10 pagesOral Path CramHarjotBrarNo ratings yet
- Pre-Placement Immunization Form (June 2017) BrockDocument2 pagesPre-Placement Immunization Form (June 2017) BrockroldinpgNo ratings yet
- Invasive Ductal Carcinoma, Left Breast Status PostDocument37 pagesInvasive Ductal Carcinoma, Left Breast Status PostKayla SalvadorNo ratings yet
- MCQs Endo FinalDocument6 pagesMCQs Endo Finalhassan qureshiNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- HT ConsentDocument4 pagesHT ConsentNaveed KhanNo ratings yet
- Communicative II Final ExamDocument6 pagesCommunicative II Final ExambashaNo ratings yet
- Toxic Effects, Drug CalculationDocument185 pagesToxic Effects, Drug CalculationAntonette Africa MercadoNo ratings yet
- Professor Graham R V Hughes MD FRCPDocument99 pagesProfessor Graham R V Hughes MD FRCPhastuti tajuddinNo ratings yet
- Bladder Carsinomas: Azif Zilal FauqiDocument18 pagesBladder Carsinomas: Azif Zilal FauqikadinfathiaNo ratings yet
- Antibiotic Stewardship in OrthopedicsDocument17 pagesAntibiotic Stewardship in Orthopedicsjomari dvNo ratings yet
- Chapter 14 - HematopathologyDocument66 pagesChapter 14 - Hematopathologynigel farageNo ratings yet
- Understanding Post COVID 19 Interstitial Lung Disease (ILDDocument4 pagesUnderstanding Post COVID 19 Interstitial Lung Disease (ILDjose luis iribarrenNo ratings yet
- Epilepsy Presentation1Document19 pagesEpilepsy Presentation1Daneshwari SahuNo ratings yet
- 문제행동아동 조기개입서비스 매뉴얼 (인쇄본)Document308 pages문제행동아동 조기개입서비스 매뉴얼 (인쇄본)Cube LeeNo ratings yet
- Revised Antibiotic Microbial ChecklistDocument1 pageRevised Antibiotic Microbial ChecklistNur Farihan OthmanNo ratings yet
- Colon and Rectum Colorectal CancerDocument20 pagesColon and Rectum Colorectal CancerJemima Nove JapitanaNo ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- 1-Agenda of Meeting ECOO 2010 (CH)Document3 pages1-Agenda of Meeting ECOO 2010 (CH)tarikeopsNo ratings yet
- DSM 5Document2 pagesDSM 5Alberto Preciado100% (1)
- Gelatinous Drop-Like Corneal Dystrophy - EyeWikiDocument3 pagesGelatinous Drop-Like Corneal Dystrophy - EyeWikitgrrwccj98No ratings yet
- Incorporating Mental Health Screening Into Adolescent Office VisitsDocument3 pagesIncorporating Mental Health Screening Into Adolescent Office VisitsnataliasulistyoNo ratings yet
- Depressive DisoredersDocument125 pagesDepressive DisoredersAbelNo ratings yet
- Retina As Window To CNS Disorders - Eye Based Diagnosis of CNS - MS & ALZHEIMER DISEASE - ARDY GISNAWAN (ARD)Document8 pagesRetina As Window To CNS Disorders - Eye Based Diagnosis of CNS - MS & ALZHEIMER DISEASE - ARDY GISNAWAN (ARD)UNHAS OphthalmologyNo ratings yet
- Psychiatry MCQs 2Document11 pagesPsychiatry MCQs 2Majed Alami100% (1)
- Nancy Berns - Degendering The Problem and Gendering The Blame - Political Discourse On Women and ViolenceDocument21 pagesNancy Berns - Degendering The Problem and Gendering The Blame - Political Discourse On Women and ViolenceJohir UddinNo ratings yet
- Death Penalty ReportDocument3 pagesDeath Penalty ReportaretisereneNo ratings yet
- Great.-WPS OfficeDocument11 pagesGreat.-WPS OfficeEdz EdzNo ratings yet
- Hope 11 Assessment 1 4TH QTRDocument2 pagesHope 11 Assessment 1 4TH QTRApril Rose Ferrancullo RelojNo ratings yet
- ReviewDocument12 pagesReviewAldebarán AzulNo ratings yet