You might also like
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (1)
- Thumbs up Trucking llc E-book: Step by step e-book on how to start a trucking companyFrom EverandThumbs up Trucking llc E-book: Step by step e-book on how to start a trucking companyNo ratings yet
- Recertification by CCP ApplicationDocument4 pagesRecertification by CCP ApplicationJoshua RuizNo ratings yet
- Application Form For Class-2 DSC - Individual Type - EditableDocument1 pageApplication Form For Class-2 DSC - Individual Type - EditableJitendra LakhotiaNo ratings yet
- APECET2023 UserGuideDocument28 pagesAPECET2023 UserGuideK. AyyappanNo ratings yet
- Cscs Smartcard Application Form: PhotoDocument2 pagesCscs Smartcard Application Form: PhotoGabiNo ratings yet
- Ukrr - 2010 - Acca Re Registration FormDocument4 pagesUkrr - 2010 - Acca Re Registration FormEl DanielNo ratings yet
- BGC Form - Campus TraineesDocument7 pagesBGC Form - Campus TraineesSimbu Rockzz75% (4)
- Application Form For CSWIP 5 Year Renewal (Overseas) - v3 1Document7 pagesApplication Form For CSWIP 5 Year Renewal (Overseas) - v3 1Bamarasan ArasanNo ratings yet
- CQI 5pp Membership Application FormDocument5 pagesCQI 5pp Membership Application FormSaravanan KulothunganNo ratings yet
- PSL57WIADocument12 pagesPSL57WIANenad MarkovićNo ratings yet
- CSC Civil Service Exam 2024Document6 pagesCSC Civil Service Exam 2024SandyNo ratings yet
- Psl/28 Issue 18 Dated 1 April 2018 Implementation Date: 1 May 2018Document6 pagesPsl/28 Issue 18 Dated 1 April 2018 Implementation Date: 1 May 2018ANH TAI MAINo ratings yet
- Course Registration Form: Contact InformationDocument2 pagesCourse Registration Form: Contact InformationJoyrikki FernandoNo ratings yet
- Online Application For Certification Guide: Do Not Begin Until You Have All Required DocumentationDocument6 pagesOnline Application For Certification Guide: Do Not Begin Until You Have All Required DocumentationizmitlimonNo ratings yet
- Apecet - 2019 (ADMISSIONS) : Instructions To CandidatesDocument12 pagesApecet - 2019 (ADMISSIONS) : Instructions To CandidatesM S KalyanNo ratings yet
- Pak Broadcast Corp FormDocument4 pagesPak Broadcast Corp FormMuhammadFarhanShakeeNo ratings yet
- Well Fare Officer FormDocument3 pagesWell Fare Officer FormKhawar AliNo ratings yet
- U M O S A F: SER Anual For Nline Ubmission of Pplication ORM NEET-PG 2023Document6 pagesU M O S A F: SER Anual For Nline Ubmission of Pplication ORM NEET-PG 2023ssv sai suryaNo ratings yet
- Application Form For CSWIP 5 Year Renewal (Overseas) - v3Document8 pagesApplication Form For CSWIP 5 Year Renewal (Overseas) - v3Renauka HasanovaNo ratings yet
- Application Form For CSWIP 10 Year Re-CertificationDocument7 pagesApplication Form For CSWIP 10 Year Re-Certificationchandana kumar0% (1)
- Excep Case Review Form For BGAS 5 Year Renewal (Overseas) - v4Document8 pagesExcep Case Review Form For BGAS 5 Year Renewal (Overseas) - v4sttwf85yvpNo ratings yet
- Punjab Prisons Department: S T NS T NDocument4 pagesPunjab Prisons Department: S T NS T NNoman KhanNo ratings yet
- U M O S A F: SER Anual For Nline Ubmission of Pplication ORM NEET-PG 2022Document5 pagesU M O S A F: SER Anual For Nline Ubmission of Pplication ORM NEET-PG 2022ratnapatilNo ratings yet
- Frequently Asked Questions: Information About Vacancies and Online ApplicationDocument5 pagesFrequently Asked Questions: Information About Vacancies and Online ApplicationankursonicivilNo ratings yet
- ASNT L3 - Renew ApplicationDocument15 pagesASNT L3 - Renew ApplicationSuntech Testing Limited STLNo ratings yet
- CMD Notification V1-1Document4 pagesCMD Notification V1-1aravindakpwdNo ratings yet
- APEDCET2023 UserGuideDocument25 pagesAPEDCET2023 UserGuideKishore KonduruNo ratings yet
- APC Enrolment Form MENADocument10 pagesAPC Enrolment Form MENAOsuntola OlayemiNo ratings yet
- NROTC Scholarship Application Instructions - Updated JUN 2021Document10 pagesNROTC Scholarship Application Instructions - Updated JUN 2021Shekhinah GreenNo ratings yet
- National Telecommunication Corporation: Registration NoDocument4 pagesNational Telecommunication Corporation: Registration NoAqeel AbbasiNo ratings yet
- For All Professions Which Involve Working in A SchoolDocument3 pagesFor All Professions Which Involve Working in A Schoolapi-365346043No ratings yet
- APLAWCET2023 UserGuideDocument24 pagesAPLAWCET2023 UserGuideRama Krishna Reddy CNo ratings yet
- GuideDocument5 pagesGuidejanclaudinefloresNo ratings yet
- Exam Multistate Application ChecklistDocument4 pagesExam Multistate Application ChecklistIdaNo ratings yet
- LDA 6april2014 FormDocument4 pagesLDA 6april2014 FormWasim AkramNo ratings yet
- Appendix G: Retest Application: Certified Technology Specialist™ CTS®, CTS-D® or CTS-I® RETEST ApplicationDocument4 pagesAppendix G: Retest Application: Certified Technology Specialist™ CTS®, CTS-D® or CTS-I® RETEST ApplicationnewworlderNo ratings yet
- NROTC Scholarship Application Instructions - Updated Aug 2022 - WordDocument12 pagesNROTC Scholarship Application Instructions - Updated Aug 2022 - Wordkhamarts68No ratings yet
- Probationary License (PL) Petition: Driver InformationDocument3 pagesProbationary License (PL) Petition: Driver InformationHoward ShowersNo ratings yet
- Cswip 3.1Document4 pagesCswip 3.1samuelNo ratings yet
- CISA Certification Application: Applicants Who Passed CISA Exam 2016 To May 2019Document4 pagesCISA Certification Application: Applicants Who Passed CISA Exam 2016 To May 2019KoKoNo ratings yet
- APPGECET2023 UserGuideDocument24 pagesAPPGECET2023 UserGuideHiiiNo ratings yet
- Enrolment Form SeaDocument3 pagesEnrolment Form SeaJong Tzy ChingNo ratings yet
- APICET2023 UserGuideDocument25 pagesAPICET2023 UserGuidenaveenenglish23No ratings yet
- Registration Guide CAT 2014Document18 pagesRegistration Guide CAT 2014Chaitanya WadiNo ratings yet
- Registration Guide CAT 2014Document18 pagesRegistration Guide CAT 2014Abdul RahimNo ratings yet
- MIArb Membership Application FormDocument3 pagesMIArb Membership Application FormFawwazFikri13No ratings yet
- OACETT Membership ApplicationDocument4 pagesOACETT Membership Applicationsalah51No ratings yet
- Processing of Examination Application (Career Service Examination-Paper and Pencil Test) (Professional or Subprofessionaltest)Document7 pagesProcessing of Examination Application (Career Service Examination-Paper and Pencil Test) (Professional or Subprofessionaltest)Anonymous GRPQhJxNo ratings yet
- Procedure For Renewal DLC 08032022Document12 pagesProcedure For Renewal DLC 08032022Abhishek ChhabraNo ratings yet
- Bel2014 Ghaziabad - Application Form 2013Document4 pagesBel2014 Ghaziabad - Application Form 2013Jagdeep ArryNo ratings yet
- CRISC Application 2021 Later FRM Eng 0821Document4 pagesCRISC Application 2021 Later FRM Eng 0821Jennifer OgbujiNo ratings yet
- BGAS-CSWIP Application Form For 10 Year Recertification (Overseas) - v3Document7 pagesBGAS-CSWIP Application Form For 10 Year Recertification (Overseas) - v3Baleegh UzzamanNo ratings yet
- Khalid Cement Complex Limited: Please Carefully Read The Guidelines On The Last Page Before Filling This FormDocument10 pagesKhalid Cement Complex Limited: Please Carefully Read The Guidelines On The Last Page Before Filling This FormMahira MalikNo ratings yet
- Application Form VtpfdsDocument12 pagesApplication Form VtpfdsLarry GarciaNo ratings yet
- Recertification by Exam Application March 2014Document2 pagesRecertification by Exam Application March 2014Ashley CampbellNo ratings yet
- License Application 991714Document9 pagesLicense Application 991714Agnes Anu cyriacNo ratings yet
- CISA Application 2016 Later FRM Eng 0818Document4 pagesCISA Application 2016 Later FRM Eng 0818Ashish SinghalNo ratings yet
- Engineer In-Training Designation Packet 5.6.2020Document15 pagesEngineer In-Training Designation Packet 5.6.2020Nora KirstenNo ratings yet
- Qualification Assessment FormDocument2 pagesQualification Assessment FormRaoofNo ratings yet
- Shalina Healthcare JD - Business AnalyticsDocument2 pagesShalina Healthcare JD - Business AnalyticsMeow bunNo ratings yet
- Working of Online Trading in Indian Stock MarketDocument81 pagesWorking of Online Trading in Indian Stock MarketVarad Mhatre100% (1)
- Talent Neuron NewsletterDocument2 pagesTalent Neuron NewsletterTalent NeuronNo ratings yet
- Module 2 - Part 2Document85 pagesModule 2 - Part 2Tanvi DeoreNo ratings yet
- Map of The 110 and 220 KV Power Transmission Line and Substation Ulaanbaatar City " Ikh Toirog " ProjectDocument10 pagesMap of The 110 and 220 KV Power Transmission Line and Substation Ulaanbaatar City " Ikh Toirog " ProjectAltanochir AagiiNo ratings yet
- CompressDocument14 pagesCompressAnonymous gfR3btyU0% (1)
- BS en Iso 11114-4-2005 (2007)Document30 pagesBS en Iso 11114-4-2005 (2007)DanielVegaNeira100% (1)
- Nagpur Company List 2Document10 pagesNagpur Company List 2Kaushik BachanNo ratings yet
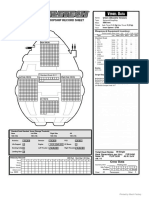
- Union Class Dropship 3025Document1 pageUnion Class Dropship 3025A KNo ratings yet
- Encryption LessonDocument2 pagesEncryption LessonKelly LougheedNo ratings yet
- Writing NuocRut Ver02Document118 pagesWriting NuocRut Ver02thuy linhNo ratings yet
- DocumentDocument2 pagesDocumentAddieNo ratings yet
- 12-24VDC Powered Ignition System: N N N N N N NDocument2 pages12-24VDC Powered Ignition System: N N N N N N NLeinner RamirezNo ratings yet
- Sharp AR-C172M ServiceM EN PDFDocument308 pagesSharp AR-C172M ServiceM EN PDFpiaggio_nrgNo ratings yet
- Merenstein Gardners Handbook of Neonatal Intensive Care 8Th Edition Sandra Lee Gardner Brian S Carter Mary I Enzman Hines Jacinto A Hernandez Download PDF ChapterDocument52 pagesMerenstein Gardners Handbook of Neonatal Intensive Care 8Th Edition Sandra Lee Gardner Brian S Carter Mary I Enzman Hines Jacinto A Hernandez Download PDF Chapterrichard.martin380100% (17)
- GCE Composite 1306 v4 PDFDocument28 pagesGCE Composite 1306 v4 PDFParapar ShammonNo ratings yet
- Assignment 1: Unit 3 - Week 1Document80 pagesAssignment 1: Unit 3 - Week 1sathiyan gsNo ratings yet
- ESAT FormulaDocument11 pagesESAT FormulaSKYE LightsNo ratings yet
- Thermister O Levels Typical QuestionDocument4 pagesThermister O Levels Typical QuestionMohammad Irfan YousufNo ratings yet
- Engineering & Machinery Corp vs. CADocument8 pagesEngineering & Machinery Corp vs. CALaila Ismael SalisaNo ratings yet
- Release Notes Csi Bridge V 2020Document9 pagesRelease Notes Csi Bridge V 2020Abdul KadirNo ratings yet
- PROPOSALDocument4 pagesPROPOSALsacheendra singhNo ratings yet
- Sciencedirect Sciencedirect SciencedirectDocument7 pagesSciencedirect Sciencedirect SciencedirectMiguel AngelNo ratings yet
- Science, Technology and SocietyDocument2 pagesScience, Technology and SocietyHamieWave TVNo ratings yet
- 147380-1 Motoman XRC Controller Fieldbus (XFB01) Instruction ManualDocument102 pages147380-1 Motoman XRC Controller Fieldbus (XFB01) Instruction Manualrubi monNo ratings yet
- 09120110155668 (1)Document49 pages09120110155668 (1)Upul NishanthaNo ratings yet
- Cambridge International Advanced Subsidiary and Advanced LevelDocument4 pagesCambridge International Advanced Subsidiary and Advanced Leveljunk filesNo ratings yet
- Reinforcement Project Examples: Monopole - Self Supporter - Guyed TowerDocument76 pagesReinforcement Project Examples: Monopole - Self Supporter - Guyed TowerBoris KovačevićNo ratings yet
- 14.symmetrix Toolings LLPDocument1 page14.symmetrix Toolings LLPAditiNo ratings yet