You might also like
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Original Research Paper Obstetrics & GynaecologyDocument4 pagesOriginal Research Paper Obstetrics & GynaecologyVogireddy SindhuNo ratings yet
- Jurnal CohortDocument21 pagesJurnal CohortAstri Anindita UtomoNo ratings yet
- Severity of Anemia During Pregnancy and Adverse Maternal and Fetal OutcomesDocument13 pagesSeverity of Anemia During Pregnancy and Adverse Maternal and Fetal OutcomesIlda IldaNo ratings yet
- Gestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDocument8 pagesGestational Diabetes Mellitus Is Associated With Adverse Outcomes in Twin PregnanciesDwi OktaviliaNo ratings yet
- Jurnal Mikia - Page - 1-9+29+novDocument9 pagesJurnal Mikia - Page - 1-9+29+novaizah afifaturNo ratings yet
- JGWH - Ms.id.555623 1 KirimDocument6 pagesJGWH - Ms.id.555623 1 KirimBaiq Bunga Citra PratiwiNo ratings yet
- Articulo 5Document6 pagesArticulo 5Monica ReyesNo ratings yet
- Jurnal JaundiceDocument8 pagesJurnal JaundiceniaNo ratings yet
- Preeclampsia Prevalence, Risk Factors, and Pregnancy OutcomesDocument14 pagesPreeclampsia Prevalence, Risk Factors, and Pregnancy OutcomesHaris FadillaNo ratings yet
- The High Prevalence and Impact of Rheumatic High Income NationsDocument10 pagesThe High Prevalence and Impact of Rheumatic High Income NationsZahed UllahNo ratings yet
- Poryo2018 IvhDocument8 pagesPoryo2018 IvhGabriel DaneaNo ratings yet
- International Conference On Applied Science and HealthDocument6 pagesInternational Conference On Applied Science and HealthUmi Marfungatun MudrikahNo ratings yet
- RiskfactorretainedplacentaDocument9 pagesRiskfactorretainedplacentaDONNYNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologySuis MionooNo ratings yet
- Winter, Spring, Summer or Fall Temporal Patterns in Placenta-Mediated Pregnancy Complications-An Exploratory AnalysisDocument8 pagesWinter, Spring, Summer or Fall Temporal Patterns in Placenta-Mediated Pregnancy Complications-An Exploratory AnalysisTushar RameshNo ratings yet
- MJMU Volume 50 Issue 4 Pages 155-163-1Document9 pagesMJMU Volume 50 Issue 4 Pages 155-163-1Fred OkelloNo ratings yet
- tseng-et-al-2022-severe-maternal-morbidity-in-pregnancies-complicated-by-fetal-congenital-heart-diseaseDocument10 pagestseng-et-al-2022-severe-maternal-morbidity-in-pregnancies-complicated-by-fetal-congenital-heart-diseaseUMAE GINENo ratings yet
- Jurnal 4Document6 pagesJurnal 4lomba Panah Dies UnsriNo ratings yet
- 1 s2.0 S1028455919300178 Main PDFDocument5 pages1 s2.0 S1028455919300178 Main PDFRadinal PrayitnoNo ratings yet
- Thyroid and Pregnancy OutcomeDocument9 pagesThyroid and Pregnancy OutcomeCindy KestyNo ratings yet
- Vol9 Issue1 06Document4 pagesVol9 Issue1 06annisaNo ratings yet
- Risk Factor Assessment For Pre-Eclampsia: A Case Control StudyDocument6 pagesRisk Factor Assessment For Pre-Eclampsia: A Case Control StudyPutra SeptiansyahNo ratings yet
- Characteristics of Preeclampsia with Severe FeaturesDocument4 pagesCharacteristics of Preeclampsia with Severe FeaturesBella AgiusselaNo ratings yet
- High Rate of Early Onset Preeclampsia in MauritiusDocument4 pagesHigh Rate of Early Onset Preeclampsia in MauritiusHarvey MatbaganNo ratings yet
- Stubert2014 PDFDocument11 pagesStubert2014 PDFRolando TintayaNo ratings yet
- Preeclampsia RiesgoDocument6 pagesPreeclampsia RiesgoRedina Tuya RamirezNo ratings yet
- PreeclampsiaDocument7 pagesPreeclampsiaObginunhas Juli2017No ratings yet
- Risk Factors For Acute Respiratory Morbidity in Moderately Preterm InfantsDocument10 pagesRisk Factors For Acute Respiratory Morbidity in Moderately Preterm InfantsYeda NicolNo ratings yet
- Tusimin 2016Document6 pagesTusimin 2016Silvie WidyaNo ratings yet
- Preeclampsia and The Risk of Bronchopulmonary Dysplasia in VLBW Infants A Population Based StudyDocument7 pagesPreeclampsia and The Risk of Bronchopulmonary Dysplasia in VLBW Infants A Population Based Studyatika sgrtNo ratings yet
- Maternal and Perinatal Outcome of Maternal Obesity atDocument6 pagesMaternal and Perinatal Outcome of Maternal Obesity attaufik perdanaNo ratings yet
- Herrera 2017Document9 pagesHerrera 2017Bianca Maria PricopNo ratings yet
- 33873-Article Text-121761-1-10-20170831Document6 pages33873-Article Text-121761-1-10-20170831AnggaNo ratings yet
- Video 12 PDFDocument5 pagesVideo 12 PDFAndreas NatanNo ratings yet
- Dr. Dr. Nugrahanti - PITFM23 PDFDocument24 pagesDr. Dr. Nugrahanti - PITFM23 PDFDarameutia obgynNo ratings yet
- An-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Document4 pagesAn-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Chiki CacaNo ratings yet
- Jurnal Reading Patol ADocument27 pagesJurnal Reading Patol Aalmira.shahnazNo ratings yet
- Hubungan Obesitas Dan Riwayat Hipertensi Dengan Kejadian Preeklamsi Di Puskesmas Rawat Inap Danau PanggangDocument5 pagesHubungan Obesitas Dan Riwayat Hipertensi Dengan Kejadian Preeklamsi Di Puskesmas Rawat Inap Danau PanggangNur Fany Putri MawangiNo ratings yet
- Gestational Diabetes Mellitus and COVID-19 (CRONOS)Document19 pagesGestational Diabetes Mellitus and COVID-19 (CRONOS)Diana MontoyaNo ratings yet
- Excellent Midwifery JournalDocument7 pagesExcellent Midwifery Journalvinny alvionitaNo ratings yet
- Risk Factors and Maternal-Fetal Outcomes of Placental AbruptionDocument5 pagesRisk Factors and Maternal-Fetal Outcomes of Placental AbruptionSuis MionooNo ratings yet
- The Characteristics of Preeclampsia With Severe Features: Karakteristik Preeklamsia Dengan Tanda PerburukanDocument4 pagesThe Characteristics of Preeclampsia With Severe Features: Karakteristik Preeklamsia Dengan Tanda PerburukanSari MustikaNo ratings yet
- Mor 2016Document9 pagesMor 2016Farin MauliaNo ratings yet
- Incidence and Risk Factors of Pre-Eclampsia in The Paropakar Maternity and Women's Hospital, Nepal: A Retrospective StudyDocument8 pagesIncidence and Risk Factors of Pre-Eclampsia in The Paropakar Maternity and Women's Hospital, Nepal: A Retrospective StudyJod BellNo ratings yet
- Less Is More Modern NeonatologyDocument11 pagesLess Is More Modern NeonatologyEN BUNo ratings yet
- Severe Placental Abruption Linked to Higher Maternal MorbidityDocument9 pagesSevere Placental Abruption Linked to Higher Maternal MorbidityOki WihardiyantoNo ratings yet
- Fetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control StudyDocument6 pagesFetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control Studyaulia ilmaNo ratings yet
- Role of Low Dose AspirinDocument11 pagesRole of Low Dose AspirinYudha GanesaNo ratings yet
- Impact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboDocument8 pagesImpact of Pregnancy-Induced Hypertension On Fetal Growth: Rima Irwinda, Raymond Surya, Lidia F. NemboPramatama AndhikaNo ratings yet
- Ijogr 3 (4) 407-409Document3 pagesIjogr 3 (4) 407-409Yuni Astuti DjoyomiharjoNo ratings yet
- Rahayu, 2021Document6 pagesRahayu, 2021Dara Dasawulansari SyamsuriNo ratings yet
- Aisyah HPTDocument10 pagesAisyah HPTBesari Md DaudNo ratings yet
- Asociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Document8 pagesAsociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Andrés Gaviria CNo ratings yet
- Neurocritical Care of The Pregnant PatientDocument24 pagesNeurocritical Care of The Pregnant PatientRicardo Robles AlfaroNo ratings yet
- Stroke and Cerebrovascular Disease in Pregnancy: Incidence, Temporal Trends, and Risk FactorsDocument8 pagesStroke and Cerebrovascular Disease in Pregnancy: Incidence, Temporal Trends, and Risk FactorstamiNo ratings yet
- Deense Studie PDFDocument12 pagesDeense Studie PDFBas HermansNo ratings yet
- Incidence of PreeclamsiaDocument12 pagesIncidence of PreeclamsiaAsril R. HakimNo ratings yet
- Karakteristik Preeklampsia Di RSUP Prof. Dr. R. D. Kandou ManadoDocument5 pagesKarakteristik Preeklampsia Di RSUP Prof. Dr. R. D. Kandou ManadoDewanto ChandraNo ratings yet
- Jurnal Reading ObygnDocument6 pagesJurnal Reading ObygnLimastani FebrianaNo ratings yet
- Philosophy, Logic, & Rhetoric SyllabusDocument3 pagesPhilosophy, Logic, & Rhetoric SyllabusBrynja KnappNo ratings yet
- Plant Associated Biofilms: Causes and ConsequencesDocument32 pagesPlant Associated Biofilms: Causes and ConsequencesGarima DhirNo ratings yet
- Datasheet GenDocument2 pagesDatasheet GenEdgar Bonilla MuñozNo ratings yet
- Rev Quiz All PDFDocument46 pagesRev Quiz All PDFNota Belz82% (17)
- L6219 Evaluation Board Application NoteDocument4 pagesL6219 Evaluation Board Application NoteBeenish MirzaNo ratings yet
- Telangana Govt T-PRIDE Scheme GuidelinesDocument90 pagesTelangana Govt T-PRIDE Scheme GuidelinesitzprasuNo ratings yet
- Using Coffee Grounds as FertilizerDocument18 pagesUsing Coffee Grounds as FertilizerKyle BARRIOSNo ratings yet
- Chapter2 AligningSelectionProjectsDocument36 pagesChapter2 AligningSelectionProjectsZeynep SenerNo ratings yet
- Agile Final Exam - Answer TranscriptDocument12 pagesAgile Final Exam - Answer TranscriptMehwish GauriNo ratings yet
- Namma Kalvi 12th Maths Book Back and Creative Questions em 219383Document185 pagesNamma Kalvi 12th Maths Book Back and Creative Questions em 219383TharaneshNo ratings yet
- Determination of Equilibrium Constant (KeqDocument0 pagesDetermination of Equilibrium Constant (KeqPablo BernalNo ratings yet
- MRCP EthicsDocument33 pagesMRCP EthicstaherNo ratings yet
- Mnemonics Anatomy 1st SemDocument4 pagesMnemonics Anatomy 1st SemNastassja Callmedoctor Douse67% (3)
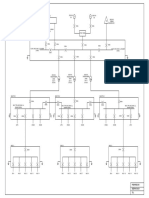
- Conceptual SLDDocument1 pageConceptual SLDakhilNo ratings yet
- Read Online Here: Bronto Skylift F32Document3 pagesRead Online Here: Bronto Skylift F32Randu WatangNo ratings yet
- Pages From 0625 - s16 - QP - 42 - 01Document2 pagesPages From 0625 - s16 - QP - 42 - 01lelon ongNo ratings yet
- Fault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)Document5 pagesFault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)zacarias NiquiceNo ratings yet
- Building Schedule 050721Document6 pagesBuilding Schedule 050721Parth DaxiniNo ratings yet
- Mktech PDFDocument7 pagesMktech PDFAlexander WieseNo ratings yet
- Guidelines in The Evaluation of Comprehensive Land Use PlanDocument8 pagesGuidelines in The Evaluation of Comprehensive Land Use PlanPa Rian Rho DoraNo ratings yet
- What Are The Different Types of PollutionDocument9 pagesWhat Are The Different Types of PollutionPatricia DurandNo ratings yet
- Asme Section II A Sa-435 Sa-435mDocument4 pagesAsme Section II A Sa-435 Sa-435mAnonymous GhPzn1xNo ratings yet
- Standard Operating Procedure: Title: Materials Control - Work in Process (WIP) ApprovalsDocument2 pagesStandard Operating Procedure: Title: Materials Control - Work in Process (WIP) ApprovalsRAHUL YADAV100% (1)
- Press 2017 Fagioli enDocument2 pagesPress 2017 Fagioli enÁlvaro Rodríguez BNo ratings yet
- DATASHEET Transistor 13003ADDocument4 pagesDATASHEET Transistor 13003ADCarlos MoraNo ratings yet
- Group 3 Safety Issues in ICTDocument15 pagesGroup 3 Safety Issues in ICTRoseAnnNo ratings yet
- Cuban Puerco Asado - Petit PorciniDocument2 pagesCuban Puerco Asado - Petit PorciniDra. Carmen DittelNo ratings yet
- Water Transport Studies in Stone Masonry With Soil Cement MortarDocument10 pagesWater Transport Studies in Stone Masonry With Soil Cement MortarTJPRC PublicationsNo ratings yet
- Vivo Device Log File with Input Method and Networking DetailsDocument133 pagesVivo Device Log File with Input Method and Networking DetailsSheilaNo ratings yet
- Material Cost - EOQDocument16 pagesMaterial Cost - EOQSimranNo ratings yet