You might also like
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- Cardiology 7 - Arrhythmias: Lecture OutlineDocument6 pagesCardiology 7 - Arrhythmias: Lecture Outlineمحمد احمد محمدNo ratings yet
- Penyakit Kardiovaskular Yang Sering DijumpaiDocument121 pagesPenyakit Kardiovaskular Yang Sering Dijumpaiandikaagus13No ratings yet
- 02.emergency CardiologyDocument135 pages02.emergency Cardiologyapi-19916399No ratings yet
- IM CASE RTR - Myocardial InfarctionDocument47 pagesIM CASE RTR - Myocardial InfarctionTrisNo ratings yet
- Acute Lower Extremity Ischaemia (ALEXI) : Nadraj G NaidooDocument25 pagesAcute Lower Extremity Ischaemia (ALEXI) : Nadraj G NaidooVishad NaidooNo ratings yet
- Medicine Paper Number 1Document8 pagesMedicine Paper Number 1arvindNo ratings yet
- 41 Paediatric ArrhythmiasDocument4 pages41 Paediatric ArrhythmiasnasibdinNo ratings yet
- Kuliah Sinkop UntadDocument35 pagesKuliah Sinkop UntadMuhammad mukramNo ratings yet
- CardioDocument67 pagesCardiovkhen88No ratings yet
- Prof. Iwan - Kuliah RHD and VHD-1Document41 pagesProf. Iwan - Kuliah RHD and VHD-1delia rahmaNo ratings yet
- Fibrillazione AtrialeDocument66 pagesFibrillazione AtrialeRiccardo ArmellinNo ratings yet
- MCQ 2019 Part 1 UseDocument94 pagesMCQ 2019 Part 1 UseMimmey YeniwNo ratings yet
- Cardiac Arrhythmias 6th YearDocument108 pagesCardiac Arrhythmias 6th YearPhaimNo ratings yet
- Acute Coronay Syndrome - BACCDocument72 pagesAcute Coronay Syndrome - BACCYeyen Devyanti HandokoNo ratings yet
- ARITMIADocument47 pagesARITMIASarah JR Nur AzizahNo ratings yet
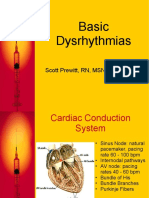
- Basic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCDocument42 pagesBasic Dysrhythmias: Scott Prewitt, RN, MSN, APRN-BCtuffie85No ratings yet
- New-Infective EndocarditisDocument30 pagesNew-Infective Endocarditisزياد سعيدNo ratings yet
- Approach To GI BleedDocument97 pagesApproach To GI BleedPankaj IngleNo ratings yet
- Robbi Zidnii Ilmaa, War Zuqnii Fahmaa, AamiinDocument109 pagesRobbi Zidnii Ilmaa, War Zuqnii Fahmaa, Aamiinfitrian amwaalunNo ratings yet
- Akut Limb IskemikDocument31 pagesAkut Limb IskemikLaluMuhammadSabarSetiawanNo ratings yet
- Acute Coronary Syndrome: Case PresentationDocument4 pagesAcute Coronary Syndrome: Case PresentationJunathan L. DelgadoNo ratings yet
- Eme CVDocument35 pagesEme CVJason LinNo ratings yet
- Hypertensive Krisis 23-10-18Document23 pagesHypertensive Krisis 23-10-18Shone NamNo ratings yet
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Document68 pagesSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- Atrial FibrillationDocument24 pagesAtrial FibrillationsatriaNo ratings yet
- Cardiac Arrythmias in The ED Menbeu Edited From AnaDocument106 pagesCardiac Arrythmias in The ED Menbeu Edited From AnaTemesgen Geleta100% (1)
- Emergency Medicine End of Rotation Exam 1Document79 pagesEmergency Medicine End of Rotation Exam 1Sidney SnyderNo ratings yet
- Medically ComprmisedDocument73 pagesMedically Comprmisedhaitham192002No ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- How To Detect and To Treat EarlierDocument59 pagesHow To Detect and To Treat EarlierFaisal ShaldyNo ratings yet
- Chapter 5 Cardiovascular EmergenciesDocument6 pagesChapter 5 Cardiovascular Emergenciesعلاء البناءNo ratings yet
- Supraventricular TachycardiaDocument22 pagesSupraventricular TachycardiaFaza KahfiNo ratings yet
- Approach To Diagnosis of Congenital Heart DiseasesDocument85 pagesApproach To Diagnosis of Congenital Heart DiseasesNirav CHOVATIYANo ratings yet
- Cerebrovascular Accidents: Stroke Versus TIADocument19 pagesCerebrovascular Accidents: Stroke Versus TIASagar ShahNo ratings yet
- VHDDocument102 pagesVHDPenuhTandaTanyaNo ratings yet
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- MCQ - Internal MedDocument2 pagesMCQ - Internal MedjennybongNo ratings yet
- Sinus Rhythm and Sinus and Atrial DysrhythmiasDocument41 pagesSinus Rhythm and Sinus and Atrial Dysrhythmiasclaudia brongNo ratings yet
- Investigations Management Notes For FinalsDocument138 pagesInvestigations Management Notes For FinalsThistell ThistleNo ratings yet
- Curs RJ Endoc EnglishDocument62 pagesCurs RJ Endoc EnglishArleen MatincaNo ratings yet
- CME Cyanotic Heart DiseaseDocument38 pagesCME Cyanotic Heart DiseaseTan Zhi HongNo ratings yet
- How To Deal With Acute Dyspneu in ER: Acute Heart Failure OR Pulmonary Problem?Document36 pagesHow To Deal With Acute Dyspneu in ER: Acute Heart Failure OR Pulmonary Problem?tyasNo ratings yet
- Acute Coronary Syndrome: Deske Muhadi Departemen Penyakit Dalam Fak - Kedokteran USU/RS HAM/RS PMDocument71 pagesAcute Coronary Syndrome: Deske Muhadi Departemen Penyakit Dalam Fak - Kedokteran USU/RS HAM/RS PMsebastian1207No ratings yet
- Approach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemDocument79 pagesApproach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemLajel S. LachicaNo ratings yet
- 5-Approach To PalpitationsDocument103 pages5-Approach To PalpitationsEverythingNo ratings yet
- CVS1 - K25 - Cardiac EmergencyDocument34 pagesCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idNo ratings yet
- EmergencyDocument47 pagesEmergencymedstudy123No ratings yet
- MCQ 2019 Part 1 UseDocument94 pagesMCQ 2019 Part 1 UseWanny WattakavanichNo ratings yet
- Department of Internal Medicine Iii Tricuspid Valve DiseasesDocument57 pagesDepartment of Internal Medicine Iii Tricuspid Valve DiseasesSuba Saravanan 12No ratings yet
- Hypertension: Fadillah MaricarDocument30 pagesHypertension: Fadillah MaricarLucky CloverNo ratings yet
- IM Case PresentationDocument97 pagesIM Case PresentationManuel Timothy Jude LoNo ratings yet
- Ventricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaDocument31 pagesVentricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaChintya Fidelia MontangNo ratings yet
- Infective Endocarditis: Akriti DahalDocument79 pagesInfective Endocarditis: Akriti DahalAkriti100% (1)
- PericarditisDocument120 pagesPericarditis18sn02nr059No ratings yet
- Acs CCS 2021 KLDocument52 pagesAcs CCS 2021 KLPitchya WangmeesriNo ratings yet
- Cardiology In-Training ObjectivesDocument18 pagesCardiology In-Training ObjectiveshectorNo ratings yet
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Valvular Heart DiseaseDocument5 pagesValvular Heart DiseaseElyas MehdarNo ratings yet
- Pleural EffusionDocument1 pagePleural EffusionElyas MehdarNo ratings yet
- Hematology UQU 2022Document94 pagesHematology UQU 2022Elyas MehdarNo ratings yet
- Diabetes MellitusDocument2 pagesDiabetes MellitusElyas MehdarNo ratings yet
- Memory Processes and Learning Theory DR Abeer Almarzouki MD, PHD 2017-2018Document32 pagesMemory Processes and Learning Theory DR Abeer Almarzouki MD, PHD 2017-2018Elyas MehdarNo ratings yet
- SCA + ThalassemiaDocument2 pagesSCA + ThalassemiaElyas MehdarNo ratings yet
- Asthma Davidson + Osmosis + Step Up MedicineDocument2 pagesAsthma Davidson + Osmosis + Step Up MedicineElyas MehdarNo ratings yet
- Principles of Infectious Diseases - 2018-2019 - AlbugamiDocument33 pagesPrinciples of Infectious Diseases - 2018-2019 - AlbugamiElyas MehdarNo ratings yet
- Copd Davidson + OsmosisDocument3 pagesCopd Davidson + OsmosisElyas MehdarNo ratings yet
- Acute Respiratory FailureDocument38 pagesAcute Respiratory FailureElyas MehdarNo ratings yet
- Heart Failure DavidsonDocument3 pagesHeart Failure DavidsonElyas MehdarNo ratings yet
- How To Take Medical History SheetDocument4 pagesHow To Take Medical History SheetElyas MehdarNo ratings yet
- Elective-Internship-Training-Program-2021 KSA Johns Hopkins AramcoDocument3 pagesElective-Internship-Training-Program-2021 KSA Johns Hopkins AramcoElyas MehdarNo ratings yet
- Pemanfaatan Kartu Kontrol Sebagai Upaya Self MonitDocument8 pagesPemanfaatan Kartu Kontrol Sebagai Upaya Self MonitRisa PrimeNo ratings yet
- Compartment SyndromeDocument4 pagesCompartment SyndromePravina PospanathanNo ratings yet
- Sleep: Dr. John BergmanDocument42 pagesSleep: Dr. John BergmanAndrew FongNo ratings yet
- Padhle 10th - Respiration (Life Processes) NotesDocument11 pagesPadhle 10th - Respiration (Life Processes) NotesSANDHYA KUMARI100% (2)
- Chapter 24: Alterations of Cardiovascular Function Power-Kean Et Al: Huether and Mccance'S Understanding Pathophysiology, Second Canadian EditionDocument20 pagesChapter 24: Alterations of Cardiovascular Function Power-Kean Et Al: Huether and Mccance'S Understanding Pathophysiology, Second Canadian EditionmonicaNo ratings yet
- Physiology, Catecholamines: Stephen Paravati Alan Rosani Steven J. WarringtonDocument2 pagesPhysiology, Catecholamines: Stephen Paravati Alan Rosani Steven J. WarringtonVincent Paul SantosNo ratings yet
- Dissection of The Amphibian Respiratory System and Mammalian Excretory SystemDocument6 pagesDissection of The Amphibian Respiratory System and Mammalian Excretory System门门No ratings yet
- DR Amsalu Bekele Ass - Professor of Medicine Head of Chest Unit Department of Internal Medicine Addis Ababa University, School of Medicine Addis Ababa, EthiopiaDocument81 pagesDR Amsalu Bekele Ass - Professor of Medicine Head of Chest Unit Department of Internal Medicine Addis Ababa University, School of Medicine Addis Ababa, EthiopiaBethelhem BirhanuNo ratings yet
- Diagnosis of Dyspnea 2011 VTDocument77 pagesDiagnosis of Dyspnea 2011 VTRovanNo ratings yet
- Essential HypertensionDocument13 pagesEssential HypertensionAhmad UlwanNo ratings yet
- Perubahan Fisiologi KehamilanDocument32 pagesPerubahan Fisiologi Kehamilandmandatari7327No ratings yet
- Crps AbstractDocument32 pagesCrps AbstractroooNo ratings yet
- Diagnostik Dan Tatalaksana Stable CAD - CCSDocument38 pagesDiagnostik Dan Tatalaksana Stable CAD - CCSIno HajrinNo ratings yet
- Al-Shifa Hospital Cardiac Cath. Department: Labetalol Hydrochloride 5mg/ml Solution For InjectionDocument2 pagesAl-Shifa Hospital Cardiac Cath. Department: Labetalol Hydrochloride 5mg/ml Solution For InjectionIyas JehadNo ratings yet
- Long QT SyndromeDocument6 pagesLong QT SyndromeJ M NoronhaNo ratings yet
- Blood Pressure PosterDocument1 pageBlood Pressure Posterapi-385956544No ratings yet
- Block C OSPE BPDocument2 pagesBlock C OSPE BPIrum RafeeqNo ratings yet
- 01 GRAT - ANS PharmDocument4 pages01 GRAT - ANS PharmjuanNo ratings yet
- Cardiology - Echo Fate Card-2Document4 pagesCardiology - Echo Fate Card-2Mateen Shukri100% (2)
- HaemorrhageDocument19 pagesHaemorrhageSrishti SrivastavaNo ratings yet
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 pagesAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNo ratings yet
- Respiratory SystemDocument36 pagesRespiratory SystemLovejoy TiñaNo ratings yet
- G - 3 - Chapter - 5 - Answer - Key - Human - Body (Expanded Universal Science)Document3 pagesG - 3 - Chapter - 5 - Answer - Key - Human - Body (Expanded Universal Science)GeetikaNo ratings yet
- Chapter 41, Pages 527-537: Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsDocument46 pagesChapter 41, Pages 527-537: Transport of Oxygen and Carbon Dioxide in Blood and Tissue FluidsAlia HaiderNo ratings yet
- Arterial Line Waveform Interpretation UHL Childrens Intensive Care GuidelineDocument5 pagesArterial Line Waveform Interpretation UHL Childrens Intensive Care GuidelineDhony100% (1)
- Assignment in NCM 112: Pilar College of Zamboanga CityDocument7 pagesAssignment in NCM 112: Pilar College of Zamboanga CityCake ManNo ratings yet
- CalciuDocument80 pagesCalciuAleks_88No ratings yet
- Booktree - NG Introduction To Anatomy and Physiology For Healthcare StudentsDocument325 pagesBooktree - NG Introduction To Anatomy and Physiology For Healthcare StudentsMohammedMujahedNo ratings yet
- DR Atif Afzal FcpsDocument48 pagesDR Atif Afzal FcpsHamza Niaz100% (1)
- Circadian RhythmsDocument4 pagesCircadian Rhythmsapi-642709499No ratings yet