You might also like
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- MEDACS ReferenceDocument3 pagesMEDACS ReferencejahangirealamNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Advanced Life Support Questions - Answers PaperDocument5 pagesAdvanced Life Support Questions - Answers Paperjahangirealam50% (10)
- List of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2Document12 pagesList of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2jahangirealam100% (1)
- Application SummaryDocument3 pagesApplication SummaryjahangirealamNo ratings yet
- Acute Stridor in Children CA1080 v.8Document13 pagesAcute Stridor in Children CA1080 v.8jahangirealamNo ratings yet
- Applied IM & FM Programs 2018Document269 pagesApplied IM & FM Programs 2018jahangirealamNo ratings yet
- Fibreoptic Intubation Update 2011Document8 pagesFibreoptic Intubation Update 2011jahangirealamNo ratings yet
- Intubation Checklist 45 060219Document2 pagesIntubation Checklist 45 060219jahangirealamNo ratings yet
- Rjad 147Document3 pagesRjad 147jahangirealamNo ratings yet
- Specialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustDocument20 pagesSpecialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustjahangirealamNo ratings yet
- Dla1a Child PrintDocument61 pagesDla1a Child PrintjahangirealamNo ratings yet
- Find Multiples of 2Document1 pageFind Multiples of 2jahangirealamNo ratings yet
- Cam PDFDocument13 pagesCam PDFjahangirealamNo ratings yet
- I FoundationsDocument7 pagesI FoundationsjahangirealamNo ratings yet
- Support Staff Employment Application Form September 2017.122288453Document10 pagesSupport Staff Employment Application Form September 2017.122288453jahangirealamNo ratings yet
- Obstructive Sleep Apnoea and AnaesthesiaDocument21 pagesObstructive Sleep Apnoea and AnaesthesiajahangirealamNo ratings yet
- 426-288-18DD-A - Job Description Specialty Doctor August 2018Document11 pages426-288-18DD-A - Job Description Specialty Doctor August 2018jahangirealamNo ratings yet
- Baromtric (89 Pages)Document89 pagesBaromtric (89 Pages)jahangirealamNo ratings yet
- Dress Up As... : The GruffaloDocument4 pagesDress Up As... : The GruffalojahangirealamNo ratings yet
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDocument8 pagesBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamNo ratings yet
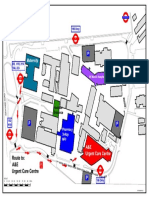
- NPHNew Wayfinding V6Document1 pageNPHNew Wayfinding V6jahangirealamNo ratings yet
- Duplicate Copy: Balance Due 123001.08Document2 pagesDuplicate Copy: Balance Due 123001.08jahangirealamNo ratings yet
- NHS Lothian Medical Application FormDocument17 pagesNHS Lothian Medical Application FormjahangirealamNo ratings yet
- Acute: Renal Failure Management in The NeonateDocument8 pagesAcute: Renal Failure Management in The NeonatejahangirealamNo ratings yet