You might also like
- Bone Graft For Papilon Lefevre PatientDocument6 pagesBone Graft For Papilon Lefevre PatientMazenShbeebNo ratings yet
- Werm Ker 2014Document7 pagesWerm Ker 2014Alice EmailsNo ratings yet
- The Management of Palatally DisplacedDocument13 pagesThe Management of Palatally DisplacedFourthMolar.comNo ratings yet
- Functional Dental Occlusion An Antropological Perspective and Implications For PracticeDocument13 pagesFunctional Dental Occlusion An Antropological Perspective and Implications For PracticeDiana NietoNo ratings yet
- TRP Greene StrubOcclusioDocument9 pagesTRP Greene StrubOcclusiodea swastikaNo ratings yet
- Dental Occlusion A Critical Reflectionon Past Present and FutureDocument8 pagesDental Occlusion A Critical Reflectionon Past Present and FutureplsssssNo ratings yet
- Carlsson 1998Document7 pagesCarlsson 1998gbaez.88No ratings yet
- 3 Badr2016Document22 pages3 Badr2016Daniel Espinoza EspinozaNo ratings yet
- Anthropology and Its Relation To Orthodontics - Part 2Document4 pagesAnthropology and Its Relation To Orthodontics - Part 2Saumya SinghNo ratings yet
- Frankel Expansion de ArcoDocument13 pagesFrankel Expansion de ArcoLisdany BecerraNo ratings yet
- 2004-AJODO-Joondeph-Mandibular Midline Osteotomy For ConstrictionDocument3 pages2004-AJODO-Joondeph-Mandibular Midline Osteotomy For ConstrictionAlejandro RuizNo ratings yet
- Zachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationDocument5 pagesZachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationplsssssNo ratings yet
- Critical Reviews in Oral Biology & Medicine: Implantology and The Severely Resorbed Edentulous MandibleDocument10 pagesCritical Reviews in Oral Biology & Medicine: Implantology and The Severely Resorbed Edentulous MandibleRik ChatterjeeNo ratings yet
- A Longitudinal Evaluation of Extraction Versus Nonextraction Treatment With Special Reference To The Posttreatment Irregularity of The Lower IncisorsDocument11 pagesA Longitudinal Evaluation of Extraction Versus Nonextraction Treatment With Special Reference To The Posttreatment Irregularity of The Lower IncisorsBeatriz ChilenoNo ratings yet
- Orthodontic Therapy and Gingival Recession, A Systematic Review PDFDocument15 pagesOrthodontic Therapy and Gingival Recession, A Systematic Review PDFJose CollazosNo ratings yet
- 2003.john H. Warford JR - Prediction of Maxillary Canine Impaction UsingDocument5 pages2003.john H. Warford JR - Prediction of Maxillary Canine Impaction UsingLuis HerreraNo ratings yet
- Regenerative Endodontics Barriers and Strategies For Clinical Translation 2012 Dental Clinics of North AmericaDocument11 pagesRegenerative Endodontics Barriers and Strategies For Clinical Translation 2012 Dental Clinics of North AmericaCaioSelaimenNo ratings yet
- Papper PeriodDocument12 pagesPapper PeriodLoretoReyesMoralesNo ratings yet
- Afraccion PDFDocument9 pagesAfraccion PDFzayraNo ratings yet
- READINGDocument11 pagesREADINGThea DuoNo ratings yet
- Dahl ApplianceDocument8 pagesDahl Appliancesarah wilderNo ratings yet
- Rehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Document19 pagesRehabilitacion de La Denticion Desgastada - Johansson Et Al - JOR 2008Pablo BenitezNo ratings yet
- Occlusion in Implant DentistryDocument9 pagesOcclusion in Implant DentistrydrsmritiNo ratings yet
- Surgical Uprighting JCO 1Document8 pagesSurgical Uprighting JCO 1Amrita ShresthaNo ratings yet
- Wiens N Priebe - Occlusal StabilityDocument25 pagesWiens N Priebe - Occlusal Stabilitymoji_puiNo ratings yet
- An Alternative Solution For A Complex Prosthodontic Problem: A Modified Andrews Fixed Dental ProsthesisDocument5 pagesAn Alternative Solution For A Complex Prosthodontic Problem: A Modified Andrews Fixed Dental ProsthesisDragos CiongaruNo ratings yet
- Avulsions and Intrusions: The Controversial Displacement InjuriesDocument7 pagesAvulsions and Intrusions: The Controversial Displacement InjuriesJing XueNo ratings yet
- Chacon2012 Libro ImplantologíaDocument10 pagesChacon2012 Libro ImplantologíaJuliett González CerdánNo ratings yet
- Tissue Response To Dental CariesDocument24 pagesTissue Response To Dental CariesGabriel Miloiu100% (1)
- Luecke 1992Document9 pagesLuecke 1992Kanchit SuwanswadNo ratings yet
- 1 s2.0 S0278239107016424 MainDocument11 pages1 s2.0 S0278239107016424 MainDANTE DELEGUERYNo ratings yet
- Fixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Document11 pagesFixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Nathawat PleumsamranNo ratings yet
- Prosthodontic Care For Patients With Cleft PalateDocument6 pagesProsthodontic Care For Patients With Cleft PalateShraddha AgarwalNo ratings yet
- Potential Mesenchymal and Dental Pulp Stem Cell Usage For Regeneration of Dentine and Its ComplicationsDocument10 pagesPotential Mesenchymal and Dental Pulp Stem Cell Usage For Regeneration of Dentine and Its ComplicationsAthenaeum Scientific PublishersNo ratings yet
- The Dahl Concept Past Present and FutureDocument9 pagesThe Dahl Concept Past Present and FuturevivigaitanNo ratings yet
- Diogenes2017.PDF Regenerative EndoDocument15 pagesDiogenes2017.PDF Regenerative Endodrmezzo68No ratings yet
- FMR of Worn Out DentititonDocument6 pagesFMR of Worn Out Dentititonrayavarapu sunilNo ratings yet
- Complete Dentures: Bone Resorption and ProsthodonticsDocument7 pagesComplete Dentures: Bone Resorption and ProsthodonticsPriyanka GandhiNo ratings yet
- Orthodontics and Periodontal Therapy (Vandarshall)Document18 pagesOrthodontics and Periodontal Therapy (Vandarshall)Priya SJNo ratings yet
- Management of Highly Resorbed Mandibular RidgeDocument11 pagesManagement of Highly Resorbed Mandibular RidgeAamir BugtiNo ratings yet
- 6-Year-Follo Up. 3 Steps Techniques. Francesca Valati-1 PDFDocument25 pages6-Year-Follo Up. 3 Steps Techniques. Francesca Valati-1 PDFAdriana CoronadoNo ratings yet
- Berlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarDocument7 pagesBerlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarISAI FLORES PÉREZNo ratings yet
- Comm Dent Oral Epid - 2006 - Fejerskov - Concepts of Dental Caries and Their Consequences For Understanding The DiseaseDocument9 pagesComm Dent Oral Epid - 2006 - Fejerskov - Concepts of Dental Caries and Their Consequences For Understanding The DiseaseDian MartínezNo ratings yet
- ContentServer (1) .Asp-16Document14 pagesContentServer (1) .Asp-16ERIKA BLANQUETNo ratings yet
- Occlusal Onlay As Mordern RX PDFDocument13 pagesOcclusal Onlay As Mordern RX PDFSMART SMARNo ratings yet
- Davis 2014Document11 pagesDavis 2014Monica JohanaNo ratings yet
- Root Resorption A 6-Year Follow-Up Case ReportDocument3 pagesRoot Resorption A 6-Year Follow-Up Case Reportpaola lopezNo ratings yet
- Stem Cells in OrthodonticsDocument4 pagesStem Cells in OrthodonticsInternational Journal of Innovative Science and Research Technology100% (1)
- Asds 02 0215Document3 pagesAsds 02 02156mf9jf6h99No ratings yet
- DT Sept 14 NPR West FNLDocument11 pagesDT Sept 14 NPR West FNLKranti PrajapatiNo ratings yet
- The Role of Occlusion in Implant Therapy - A Comprehensive Updated ReviewDocument10 pagesThe Role of Occlusion in Implant Therapy - A Comprehensive Updated ReviewFrancisca Dinamarca LamaNo ratings yet
- 5-Management of Space ProblemsDocument10 pages5-Management of Space ProblemsMuhammad UzairNo ratings yet
- Longterm Prognosis of Tooth Autotransplantation A Systematic Review and MetaanalysisDocument8 pagesLongterm Prognosis of Tooth Autotransplantation A Systematic Review and MetaanalysisJonathan Omar Cristobal VelazquezNo ratings yet
- Ghafari (1997) Emerging Paradigms in Orthodontics - An EssayDocument8 pagesGhafari (1997) Emerging Paradigms in Orthodontics - An EssayMaja Maja BułkaNo ratings yet
- Removable Partial Dentures: ReferencesDocument5 pagesRemovable Partial Dentures: ReferencesKakak AdekNo ratings yet
- Dental Update 2010. Consequences of Tooth Loss 2. Dentist Considerations Restorative Problems and ImplicationsDocument5 pagesDental Update 2010. Consequences of Tooth Loss 2. Dentist Considerations Restorative Problems and ImplicationsJay PatelNo ratings yet
- Development of OcclusionDocument17 pagesDevelopment of OcclusionIJAR JOURNALNo ratings yet
- ArticlesDocument7 pagesArticlesAnukrity PathakNo ratings yet
- X-Radius Trio Plus: Every Diagnostic Dimension Direct ConversionDocument12 pagesX-Radius Trio Plus: Every Diagnostic Dimension Direct Conversionhatem elkilaniNo ratings yet
- Halitosis JournalDocument9 pagesHalitosis JournalnicolasbriansNo ratings yet
- The Name of The Teeth Beatrice CioroiuDocument3 pagesThe Name of The Teeth Beatrice CioroiuBeatrice CioroiuNo ratings yet
- NBDE Part 2 RQ 2017 Very ImportantDocument55 pagesNBDE Part 2 RQ 2017 Very ImportantSkAliHassan100% (3)
- Early Childhood Caries Epidemiology, Aetiology, Risk Assessment, Societal Burden, Management, Education, and Policy: Global PerspectiveDocument11 pagesEarly Childhood Caries Epidemiology, Aetiology, Risk Assessment, Societal Burden, Management, Education, and Policy: Global PerspectiveAbdul RasheedNo ratings yet
- Periodontium NotesDocument12 pagesPeriodontium NotesClarisse Mendoza100% (1)
- Dental Science - Modified Sheffield Test GBDocument2 pagesDental Science - Modified Sheffield Test GBCazanNo ratings yet
- KuDocument8 pagesKuEmily JonesNo ratings yet
- Maxillofacial ProstheticsDocument7 pagesMaxillofacial ProstheticsAmar Bhochhibhoya100% (1)
- Opalescence Tooth Whitening Systems: At-Home Whitening InstructionsDocument1 pageOpalescence Tooth Whitening Systems: At-Home Whitening InstructionsPande NandaNo ratings yet
- Ahead Adc MCQDocument12 pagesAhead Adc MCQSOMVIR KUMARNo ratings yet
- Hand Instruments: Thursday, March 18, 2021 02:23 PMDocument2 pagesHand Instruments: Thursday, March 18, 2021 02:23 PMjunquelalaNo ratings yet
- Dental Diagnostic: InstrumentsDocument19 pagesDental Diagnostic: InstrumentsErdeli StefaniaNo ratings yet
- Implant Dentistry - The Most Promising Discipline of Dentistry PDFDocument488 pagesImplant Dentistry - The Most Promising Discipline of Dentistry PDFnaresh sharmaNo ratings yet
- Brushing and Flossing The Teeth of Conscious and Unconscious Client Procedure ChecklistDocument6 pagesBrushing and Flossing The Teeth of Conscious and Unconscious Client Procedure ChecklistGLORY MI SHANLEY CARUMBANo ratings yet
- Ijcrims 1Document9 pagesIjcrims 1smritiNo ratings yet
- 004 Articulo Estetica NishimuraDocument29 pages004 Articulo Estetica NishimuraJesusCordoba100% (1)
- Simon P. Hullihen and The Origin of Orthognathic Surgery: Special ContributionDocument5 pagesSimon P. Hullihen and The Origin of Orthognathic Surgery: Special ContributionRulo NarvaNo ratings yet
- Responsiveness of Oral Health-Related Quality of Life Questionnaires To Dental Caries Interventions: Systematic Review and Meta-AnalysisDocument14 pagesResponsiveness of Oral Health-Related Quality of Life Questionnaires To Dental Caries Interventions: Systematic Review and Meta-AnalysisQuenntanaNo ratings yet
- Brochure MI VarnishDocument8 pagesBrochure MI VarnishIka KusumawatiNo ratings yet
- Skeletal Anchorage For Orthopedic Correction of Growing Class III PatientsDocument14 pagesSkeletal Anchorage For Orthopedic Correction of Growing Class III PatientsIslam ShakerNo ratings yet
- Retention and Stability of Complete DentureDocument7 pagesRetention and Stability of Complete Denturemanishpankaj123No ratings yet
- C SpeeDocument4 pagesC SpeeCynthia AlfaroNo ratings yet
- Denture RepairDocument21 pagesDenture RepairDianne Mamaid0% (1)
- CH 3Document51 pagesCH 3LuJain Al-ShaikhNo ratings yet
- Preview 18041 Romano Lingual and Esthetic OrthodonticsDocument21 pagesPreview 18041 Romano Lingual and Esthetic OrthodonticsThang Nguyen TienNo ratings yet
- Intraoral Radiography With RINN XCP /Xcp-Ds InstrumentsDocument16 pagesIntraoral Radiography With RINN XCP /Xcp-Ds InstrumentsARNo ratings yet
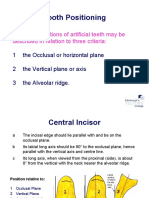
- Tooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaDocument19 pagesTooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaCherine SnookNo ratings yet
- Implant Procedures Atlas of The Oral and Maxillofacial Surgery Clinics of North AmericaDocument135 pagesImplant Procedures Atlas of The Oral and Maxillofacial Surgery Clinics of North Americafarcasiu90% (10)
- Arrangement of Teeth For Functional Harmony - PPTX 1Document102 pagesArrangement of Teeth For Functional Harmony - PPTX 1ChaithraNo ratings yet