You might also like
- History Taking VisayaDocument4 pagesHistory Taking VisayaEmily Laurente100% (1)
- 100 Diseases Treated by Single Point of AcupunctureDocument209 pages100 Diseases Treated by Single Point of AcupunctureAgeng Rikhmawan100% (31)
- Neurology Ophthalmology Psychiatry Medical MasterclassDocument288 pagesNeurology Ophthalmology Psychiatry Medical MasterclassHaytham Ibrahim Kamel100% (2)
- Case Record FormDocument30 pagesCase Record FormVirag Patil100% (1)
- Elements of The Psychiatric AssessmentDocument5 pagesElements of The Psychiatric AssessmentdevNo ratings yet
- Journal of Neurology Volume 256 Issue 3 2009 (Doi 10.1007/s00415-009-0149-2) T. Lempert H. Neuhauser - Epidemiology of Vertigo, Migraine and Vestibular MigraineDocument6 pagesJournal of Neurology Volume 256 Issue 3 2009 (Doi 10.1007/s00415-009-0149-2) T. Lempert H. Neuhauser - Epidemiology of Vertigo, Migraine and Vestibular MigraineDevi Arnes SimanjuntakNo ratings yet
- Massage Therapy EffectsDocument12 pagesMassage Therapy EffectsEkalevi FahlepieNo ratings yet
- History Taking - Cheat SheetDocument1 pageHistory Taking - Cheat SheetANGELICA CLAIRE BARECUATRONo ratings yet
- Nursing Health History Assessment and Review of SystemsDocument2 pagesNursing Health History Assessment and Review of SystemsJohanna Recca MarinoNo ratings yet
- Complete Health History FormatDocument3 pagesComplete Health History FormatAngela jane MadristaNo ratings yet
- Clinical AssignmentDocument8 pagesClinical AssignmentLauren NeisentNo ratings yet
- English Worksheet 8 N3Document3 pagesEnglish Worksheet 8 N3Will MendozaNo ratings yet
- Diabetic Neuropathy 1Document16 pagesDiabetic Neuropathy 1Alejandro Daniel Landa MoralesNo ratings yet
- GuideDocument4 pagesGuideMia Grace GarciaNo ratings yet
- Family First Chiropractic Client Intake 03172Document6 pagesFamily First Chiropractic Client Intake 03172Trina AsterinoNo ratings yet
- Pediatric Health Assessment FormDocument3 pagesPediatric Health Assessment FormCabaddu AngieNo ratings yet
- Nursing Interview Guide - HA - VIOSDocument9 pagesNursing Interview Guide - HA - VIOSIra Velle ViosNo ratings yet
- History Taking and Mental State ExaminationDocument36 pagesHistory Taking and Mental State ExaminationadeshNo ratings yet
- Clinical Diagnostic AssessmentDocument7 pagesClinical Diagnostic Assessmentjirehcounseling83% (6)
- Interview Guide QuestionsDocument3 pagesInterview Guide QuestionsYam KayeNo ratings yet
- Extensive Nursing Assessment Mental Status QuestionsDocument4 pagesExtensive Nursing Assessment Mental Status QuestionsTauqeer AhmedNo ratings yet
- Lets Talk About HealthDocument3 pagesLets Talk About HealthsimonaNo ratings yet
- Soul Proof - If You Really Knew, How Would You LiveDocument1 pageSoul Proof - If You Really Knew, How Would You Livelindakop2528No ratings yet
- University of Professional Studies, Accra: Medical DirectorateDocument1 pageUniversity of Professional Studies, Accra: Medical DirectorateSage SkitoNo ratings yet
- Basic History Taking: Tim Communication Skill FKUBDocument30 pagesBasic History Taking: Tim Communication Skill FKUBnarulita_94No ratings yet
- Biographical Data 1Document7 pagesBiographical Data 1Maddi AlonzoNo ratings yet
- Medicine General HXDocument5 pagesMedicine General HXudazxfNo ratings yet
- Interviewing Patient GuideDocument2 pagesInterviewing Patient GuideArnold Janssen PascuaNo ratings yet
- History Taking and Mental State Examination 2Document35 pagesHistory Taking and Mental State Examination 2Noreen Choudhri100% (2)
- Mija Rimay - Questions For SDDocument4 pagesMija Rimay - Questions For SDYaz GhorlNo ratings yet
- NHH Questionnaire 1Document3 pagesNHH Questionnaire 1Laurente, Patrizja Ysabel B. BSN-2DNo ratings yet
- PSYCH - MBBS - (Use Outline To Create Other Templates) Anggelos NotesDocument26 pagesPSYCH - MBBS - (Use Outline To Create Other Templates) Anggelos NotesNariska Cooper100% (2)
- Intake FormDocument8 pagesIntake FormYusra EjazNo ratings yet
- Health Assessment GuideDocument10 pagesHealth Assessment GuideAriane CauanNo ratings yet
- Nursing Interview Guide To Collect Subjective Data From The ClientDocument10 pagesNursing Interview Guide To Collect Subjective Data From The ClientDawn EncarnacionNo ratings yet
- CaseperformaDocument7 pagesCaseperformaSandip VaghelaNo ratings yet
- Interview Fill Up FormDocument4 pagesInterview Fill Up FormMarichelle AbreganaNo ratings yet
- Case Record PDFDocument31 pagesCase Record PDFAmey JatharNo ratings yet
- AnamnesaDocument5 pagesAnamnesaShafira Alief RamadhaniyarNo ratings yet
- Patient'S ProfileDocument17 pagesPatient'S ProfileLucas JelmarNo ratings yet
- 1 Health History Woman PDFDocument3 pages1 Health History Woman PDFAhlem LahidhebNo ratings yet
- Intake Inventory: 730 Emerson Dr. NE Palm Bay, FL 32907Document11 pagesIntake Inventory: 730 Emerson Dr. NE Palm Bay, FL 32907joshua brathwaiteNo ratings yet
- Complete Health HistoryDocument22 pagesComplete Health HistorykhalidNo ratings yet
- New Patient Paperwork 10 2023Document7 pagesNew Patient Paperwork 10 2023María CristinaNo ratings yet
- DSM-IV Axis IDocument5 pagesDSM-IV Axis ISobiii BooksNo ratings yet
- Initial Interview TemplateDocument4 pagesInitial Interview TemplateJoan ChoiNo ratings yet
- Ryle S. Jacinto: 12-HumanityDocument6 pagesRyle S. Jacinto: 12-HumanityPauloXander LozanoNo ratings yet
- CNS History TakingDocument4 pagesCNS History TakingDuha B. Salim100% (1)
- Paeds History Taking - 210705 - 234722Document3 pagesPaeds History Taking - 210705 - 234722F ParikhNo ratings yet
- Health Assessment TAKE HOME ASSIGNMENT CH 4 The Complete Health History Name - Section - DateDocument5 pagesHealth Assessment TAKE HOME ASSIGNMENT CH 4 The Complete Health History Name - Section - DateAndy NguyenNo ratings yet
- Adult in TakeDocument9 pagesAdult in TakeNaura CorporationNo ratings yet
- Komunikasi Dalam Perawatan Paliatif: Maria A. WitjaksonoDocument61 pagesKomunikasi Dalam Perawatan Paliatif: Maria A. Witjaksonoputri utamiNo ratings yet
- COMMED History and PE ScriptDocument16 pagesCOMMED History and PE ScriptCW DyNo ratings yet
- Asthma PossibleDocument6 pagesAsthma PossiblecrcespNo ratings yet
- Station #: InstructionsDocument5 pagesStation #: InstructionscrcespNo ratings yet
- Medical Questionnaire & Program RegistrationDocument11 pagesMedical Questionnaire & Program RegistrationKenny LeeNo ratings yet
- Assessment For Duty 2Document19 pagesAssessment For Duty 2Kim TangoNo ratings yet
- PBH101Document63 pagesPBH101Emran HossainNo ratings yet
- Assessment of The Childbearing Woman: Nursing Health History FormatDocument12 pagesAssessment of The Childbearing Woman: Nursing Health History FormatJmy CoronadoNo ratings yet
- Clinical Interview AdultDocument12 pagesClinical Interview AdultPrince Arora100% (1)
- Golden Gate Colleges P. Prieto ST., Batangas City: College of NursingDocument7 pagesGolden Gate Colleges P. Prieto ST., Batangas City: College of NursingR Hornilla ArcegaNo ratings yet
- Interview QsDocument6 pagesInterview QsRaise RaiseNo ratings yet
- Confidential Client Case History and Intake FormDocument1 pageConfidential Client Case History and Intake FormlunaNo ratings yet
- The Everything Health Guide to OCD: Professional advice on handling anxiety, understanding treatment options, and finding the support you needFrom EverandThe Everything Health Guide to OCD: Professional advice on handling anxiety, understanding treatment options, and finding the support you needRating: 5 out of 5 stars5/5 (1)
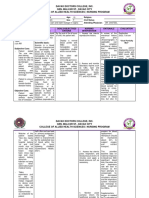
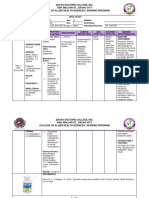
- Barecuatro - Module 2 - Nursing Care PlanDocument6 pagesBarecuatro - Module 2 - Nursing Care PlanANGELICA CLAIRE BARECUATRONo ratings yet
- Barecuatro - Module 2 - Drug Study (Folic Acid)Document2 pagesBarecuatro - Module 2 - Drug Study (Folic Acid)ANGELICA CLAIRE BARECUATRONo ratings yet
- Barecuatro Module1 FdarDocument1 pageBarecuatro Module1 FdarANGELICA CLAIRE BARECUATRONo ratings yet
- Barecuatro - Module 2 - Drug Study (Folic Acid)Document2 pagesBarecuatro - Module 2 - Drug Study (Folic Acid)ANGELICA CLAIRE BARECUATRONo ratings yet
- Barecuatro - Module 2 - Nursing Care PlanDocument6 pagesBarecuatro - Module 2 - Nursing Care PlanANGELICA CLAIRE BARECUATRONo ratings yet
- 50 Item Medical-Surgical Nursing Test DrillDocument17 pages50 Item Medical-Surgical Nursing Test DrillFilipino Nurses CentralNo ratings yet
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- Proofreading: Headaches: Sample Paragraph With Clear Support Sentences HeadachesDocument2 pagesProofreading: Headaches: Sample Paragraph With Clear Support Sentences Headachesice queenNo ratings yet
- 111 BBBDocument99 pages111 BBBjoelrequenaNo ratings yet
- 2014-2015 World Predictions by Terry & Linda Jamison, The Psychic Twins. Broadcast LIVE On Jan 6th 2014Document49 pages2014-2015 World Predictions by Terry & Linda Jamison, The Psychic Twins. Broadcast LIVE On Jan 6th 2014PsychicPredictions100% (2)
- Occipital NeuralgiaDocument12 pagesOccipital NeuralgiaStudentNo ratings yet
- Management of Patients With Neurologic DisordersDocument9 pagesManagement of Patients With Neurologic DisordersJames Felix Gallano GalesNo ratings yet
- Huang PsychologicalEffectsBrainwaveEntrainment PDFDocument12 pagesHuang PsychologicalEffectsBrainwaveEntrainment PDFSiva Gnanam KNo ratings yet
- Headache: Paul G. Mathew, M.D., and Ivan Garza, M.DDocument13 pagesHeadache: Paul G. Mathew, M.D., and Ivan Garza, M.DElizabeth PedruezaNo ratings yet
- Nature's Pathways Apr 2012 Issue - Northeast WI EditionDocument108 pagesNature's Pathways Apr 2012 Issue - Northeast WI EditionNature's PathwaysNo ratings yet
- Gingko BilobaDocument6 pagesGingko BilobaSamson RajNo ratings yet
- De Thi KSCL Tieng Anh 12 Lan 1 Nam 2019 Truong Phan Dinh Phung Ha TinhDocument10 pagesDe Thi KSCL Tieng Anh 12 Lan 1 Nam 2019 Truong Phan Dinh Phung Ha TinhTú VõNo ratings yet
- STROKE Mimic and Chameleons EDDocument34 pagesSTROKE Mimic and Chameleons EDMohammad LouayNo ratings yet
- Disorders of The Nervous System2Document20 pagesDisorders of The Nervous System2Ian Rizavi Villamor AntopinaNo ratings yet
- Clinical Examination of Patients With Headache ComplaintsDocument157 pagesClinical Examination of Patients With Headache ComplaintsrapannikaNo ratings yet
- 54750174Document3 pages54750174Rouwi DesiatcoNo ratings yet
- Neurology NotesDocument87 pagesNeurology Notessuggaplum100% (2)
- Dafpus ArisDocument2 pagesDafpus ArisRobin CastilloNo ratings yet
- Plab 2 Recall 5Document137 pagesPlab 2 Recall 5Sadiya IslamNo ratings yet
- Lampiran 155 Penyakit Dan Kode ICD 10Document9 pagesLampiran 155 Penyakit Dan Kode ICD 10Estiani NingsihNo ratings yet
- How Bio-Frequencies Can Help YouDocument10 pagesHow Bio-Frequencies Can Help YouGintaras SabulisNo ratings yet
- Icd-10-Cm Coding Guidance For Traumatic Brain Injury: Medical Provider Screening and Diagnostic Coding Dod Tbi DefinitionDocument3 pagesIcd-10-Cm Coding Guidance For Traumatic Brain Injury: Medical Provider Screening and Diagnostic Coding Dod Tbi DefinitionchaandNo ratings yet
- Imam MCQDocument16 pagesImam MCQAsem Shadid100% (1)
- Chapter 35. Headache, Self-Assessment QuestionsDocument5 pagesChapter 35. Headache, Self-Assessment Questionstsegaab yosephNo ratings yet
- Arnadottir & Sigurdardottir, 2013 - Is Craniosacral Therapy Effective For Migrane - Tested With HIT - QuestionnaireDocument4 pagesArnadottir & Sigurdardottir, 2013 - Is Craniosacral Therapy Effective For Migrane - Tested With HIT - QuestionnaireFlávio GuimarãesNo ratings yet
- Does Klonopin (Clonazepam) Work For MigrainesDocument4 pagesDoes Klonopin (Clonazepam) Work For MigrainesTooba SiddiquiNo ratings yet