You might also like
- OSTEOARTHRITISDocument53 pagesOSTEOARTHRITISRiza Umami100% (1)
- Impact of COVID-19 and Lockdown On Mental Health of Children and Adolescents: A Narrative Review With RecommendationsDocument10 pagesImpact of COVID-19 and Lockdown On Mental Health of Children and Adolescents: A Narrative Review With RecommendationsS. M. MUNAWAR MAHTAB 1603061100% (1)
- Journal of Affective Disorders: Maternal Psychological Distress & Mental Health Service Use During The COVID-19 PandemicDocument33 pagesJournal of Affective Disorders: Maternal Psychological Distress & Mental Health Service Use During The COVID-19 PandemicihlusfardanNo ratings yet
- Cameron 2020Document10 pagesCameron 2020S2-IKM ULMNo ratings yet
- Children and Youth Services ReviewDocument10 pagesChildren and Youth Services ReviewmissappleNo ratings yet
- An Investigation of Mental Health Status of Children and Adolescents in ChinaDocument7 pagesAn Investigation of Mental Health Status of Children and Adolescents in ChinaCECILIA BELEN FIERRO ALVAREZNo ratings yet
- The Impact of The Covid-19 Social and Physical Restrictive Measures On Cypriot Parents' and Children's' Well-BeingDocument19 pagesThe Impact of The Covid-19 Social and Physical Restrictive Measures On Cypriot Parents' and Children's' Well-BeingDemetris HadjicharalambousNo ratings yet
- Mental Health Needs During COVID-19: Responses in Pediatric Health CareDocument4 pagesMental Health Needs During COVID-19: Responses in Pediatric Health CareIndiana Family to FamilyNo ratings yet
- Conflict and Marital Satisfaction During CovidDocument11 pagesConflict and Marital Satisfaction During CovidCristiana OprișescuNo ratings yet
- Family Resilience During COVID-19 Pandemic: A Literature ReviewDocument7 pagesFamily Resilience During COVID-19 Pandemic: A Literature ReviewCorina PaicaNo ratings yet
- Impact of Covid 19 On Mental HealthDocument18 pagesImpact of Covid 19 On Mental HealthNada ImranNo ratings yet
- An Analysis of The Effects of Covid-19 and Lockdowns On Social and Psychological BehavioursDocument7 pagesAn Analysis of The Effects of Covid-19 and Lockdowns On Social and Psychological BehavioursRiezky AnrizaNo ratings yet
- Mark Lordson C. Rustria HUMMS D 3IS ImmersionDocument11 pagesMark Lordson C. Rustria HUMMS D 3IS ImmersionAra Lourise RustriaNo ratings yet
- Covid19 Singapore ParentingDocument35 pagesCovid19 Singapore Parentingkashish behlNo ratings yet
- RRL NotesDocument5 pagesRRL NotesAndrea LeonorNo ratings yet
- Preventive Medicine 146 (2021) 106465Document9 pagesPreventive Medicine 146 (2021) 106465shintasoloNo ratings yet
- Nguyen D. Health Disparities in Children & Adolescents During PandemicDocument3 pagesNguyen D. Health Disparities in Children & Adolescents During Pandemicjuliana.diaz06No ratings yet
- Challenges of Parents of Children With Special Needs in The New NormalDocument17 pagesChallenges of Parents of Children With Special Needs in The New NormalPsychology and Education: A Multidisciplinary JournalNo ratings yet
- BJHP 12450Document10 pagesBJHP 12450futboleditorNo ratings yet
- Article 2Document15 pagesArticle 2Yam Esor OsomrofNo ratings yet
- KFP Lit ReviewDocument11 pagesKFP Lit Reviewapi-719332888No ratings yet
- The Impact of The COVID-19 Pandemic On TheDocument13 pagesThe Impact of The COVID-19 Pandemic On TheSuzanne LauNo ratings yet
- Mental Health of Children and Adolescents Amidst COVID-19 and Past Pandemics: A Rapid Systematic ReviewDocument16 pagesMental Health of Children and Adolescents Amidst COVID-19 and Past Pandemics: A Rapid Systematic ReviewHeartgwea BuladacoNo ratings yet
- COVID 19 Pandemic and Lockdown Cause of Sleep Disruption Depression Somatic Pain and Increased Screen Exposure of Office Workers and Students of IndiaDocument11 pagesCOVID 19 Pandemic and Lockdown Cause of Sleep Disruption Depression Somatic Pain and Increased Screen Exposure of Office Workers and Students of IndiaAntonio GarcíaNo ratings yet
- JURNALDocument20 pagesJURNALDewi SunnnNo ratings yet
- SWK 3910 Research Proposal M TuttleDocument18 pagesSWK 3910 Research Proposal M Tuttleapi-638567777No ratings yet
- Transforming Practice With HOPE (Healthy Outcomes From Positive Experiences)Document6 pagesTransforming Practice With HOPE (Healthy Outcomes From Positive Experiences)Catarina GrandeNo ratings yet
- Shared Goals For Mental Health Research What Why and When For The 2020sDocument10 pagesShared Goals For Mental Health Research What Why and When For The 2020saimeejacobs370No ratings yet
- The Impact of COVID 19 Pandemic On Mental Health Amp Wel 2020 Journal of ADocument8 pagesThe Impact of COVID 19 Pandemic On Mental Health Amp Wel 2020 Journal of AlucianoNo ratings yet
- Influence of COVID-19 Social Distancing Preventive Measure On The Psychological Well-Being of Kenya Certificate of Secondary Education (KCSE) 2021 Candidates in Mombasa County, KenyaDocument10 pagesInfluence of COVID-19 Social Distancing Preventive Measure On The Psychological Well-Being of Kenya Certificate of Secondary Education (KCSE) 2021 Candidates in Mombasa County, KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impacts of The COVID-19 Pandemic On Children: An Ethical Analysis With A Global-Child LensDocument10 pagesImpacts of The COVID-19 Pandemic On Children: An Ethical Analysis With A Global-Child LensTiwi QiraNo ratings yet
- Neill2021 Article MediaConsumptionAndMentalHealtDocument9 pagesNeill2021 Article MediaConsumptionAndMentalHealtKhadijaNo ratings yet
- Willner 2020Document11 pagesWillner 2020Sonny TehNo ratings yet
- The Problems Encountered During Covid-19 Pandemic Among Criminology Students in Pimsat Colleges, San Carlos Campus An AssessmentDocument14 pagesThe Problems Encountered During Covid-19 Pandemic Among Criminology Students in Pimsat Colleges, San Carlos Campus An Assessmentrochelle posadasNo ratings yet
- Prevalence of Depression, Anxiety and Stress During The COVID-19 Pandemic: A Cross-Sectional Study Among Palestinian Students (10-18 Years)Document12 pagesPrevalence of Depression, Anxiety and Stress During The COVID-19 Pandemic: A Cross-Sectional Study Among Palestinian Students (10-18 Years)aissa ijaponNo ratings yet
- The Relationship Between Academic vs. Family/ Personal Role Conflict and Malaysian Students' Psychological Wellbeing During COVID-19 LockdownDocument14 pagesThe Relationship Between Academic vs. Family/ Personal Role Conflict and Malaysian Students' Psychological Wellbeing During COVID-19 LockdownAde CameliaNo ratings yet
- Mental Health Effects of School Closures During COVID-19: ReflectionsDocument1 pageMental Health Effects of School Closures During COVID-19: ReflectionsStefenie Katrin SibosNo ratings yet
- A Correlational Study: Quality of Life and Mental Health of Psychology Students Amidst The PandemicDocument9 pagesA Correlational Study: Quality of Life and Mental Health of Psychology Students Amidst The PandemicPsychology and Education: A Multidisciplinary JournalNo ratings yet
- India and Covid 19.Document2 pagesIndia and Covid 19.Shubha DiwakarNo ratings yet
- Related Review of LiteratureDocument3 pagesRelated Review of LiteratureRhealyn IglesiaNo ratings yet
- Knowledge, Attitudes, Anxiety, and Coping Strategies of Students During COVID-19 PandemicDocument9 pagesKnowledge, Attitudes, Anxiety, and Coping Strategies of Students During COVID-19 PandemicAindre AmeliaNo ratings yet
- The Impact of Post Covid 19 On Youth's Mental IllnessDocument10 pagesThe Impact of Post Covid 19 On Youth's Mental Illness23005583No ratings yet
- Yohana Ratrin Hestyanti, DKK - Life Changes, Stress, and Coping Stress - Undergraduate Students - During PandemicDocument12 pagesYohana Ratrin Hestyanti, DKK - Life Changes, Stress, and Coping Stress - Undergraduate Students - During Pandemicppg.adriyanrahman01630No ratings yet
- Impact of CovidDocument36 pagesImpact of CovidLuis FonbuenaNo ratings yet
- 2021 Viviana HuDocument19 pages2021 Viviana Hu4B Ade IrfanNo ratings yet
- Challenges Encountered by Post-COVID 19 ClientsDocument15 pagesChallenges Encountered by Post-COVID 19 ClientsPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Chung2020 Article MediatingEffectsOfParentalStreDocument12 pagesChung2020 Article MediatingEffectsOfParentalStreSamuel DeveloperNo ratings yet
- Journal Format Mental Health Well Being and Coping Strategies of ECE During COVID 19 PandemicDocument13 pagesJournal Format Mental Health Well Being and Coping Strategies of ECE During COVID 19 PandemicJan Carl OrtilanoNo ratings yet
- A Community Perspective of COVID 19 and Obesity in Children 2021 Obesity MedDocument6 pagesA Community Perspective of COVID 19 and Obesity in Children 2021 Obesity MedpangaribuansantaNo ratings yet
- Psychiatry Research 289 (2020) 113098Document6 pagesPsychiatry Research 289 (2020) 113098Argonne Robert AblanqueNo ratings yet
- Estres ParentalDocument12 pagesEstres ParentalMargel Alejandra Parra FernándezNo ratings yet
- The Effects of Mental Health To Academic PerformanceDocument24 pagesThe Effects of Mental Health To Academic PerformancesimonetobeschuvanesNo ratings yet
- Preventive MedicineDocument7 pagesPreventive MedicineNeni Tri Zulyana UlfahNo ratings yet
- Coronavirus ThesisDocument4 pagesCoronavirus Thesisdnr68wp2100% (2)
- Published May 22 2020 Erick T. Baloran Knowledge Attitudes Anxiety and Coping Strategies of Students During COVID 19 PandemicDocument10 pagesPublished May 22 2020 Erick T. Baloran Knowledge Attitudes Anxiety and Coping Strategies of Students During COVID 19 PandemicReign SeptemberNo ratings yet
- RM Literature ReviewDocument23 pagesRM Literature Reviewayush sachdevNo ratings yet
- Covid-19: Psychological Aspect On Health of The AdoloscentDocument5 pagesCovid-19: Psychological Aspect On Health of The AdoloscentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 10 53424-Balikesirsbd 1056775-2187961Document9 pages10 53424-Balikesirsbd 1056775-2187961obenimNo ratings yet
- Aspects of Well-Being and Academic Achievement of College Students During Covid-19Document8 pagesAspects of Well-Being and Academic Achievement of College Students During Covid-19IJAR JOURNALNo ratings yet
- 2020-Improving Mental Health PRI 41385-113065-2-PBDocument8 pages2020-Improving Mental Health PRI 41385-113065-2-PBTria WidyastutiNo ratings yet
- The Austerity Cure: The Impact of Benefit Sanctions on Mental HealthFrom EverandThe Austerity Cure: The Impact of Benefit Sanctions on Mental HealthNo ratings yet
- Warm Referrals Trauma Violence Approach Community ServicesDocument27 pagesWarm Referrals Trauma Violence Approach Community ServicesTreyNo ratings yet
- Beyond Basic Active ListeningDocument27 pagesBeyond Basic Active ListeningTreyNo ratings yet
- From Breast Is BestDocument23 pagesFrom Breast Is BestTreyNo ratings yet
- Measuring Climate Resilience Health SystemsDocument39 pagesMeasuring Climate Resilience Health SystemsTreyNo ratings yet
- 10-07-2013Document20 pages10-07-2013cn_cadillacmiNo ratings yet
- Malignant Otitis Externa: A Retrospective Analysis and Treatment OutcomesDocument5 pagesMalignant Otitis Externa: A Retrospective Analysis and Treatment OutcomesiinknisaNo ratings yet
- Lecture 1-Introduction-Rationale For Corrective ExercisesDocument50 pagesLecture 1-Introduction-Rationale For Corrective ExercisesGreg RoeNo ratings yet
- Lukoff - Mysticism and PsychosisDocument27 pagesLukoff - Mysticism and Psychosiscurfexxx100% (1)
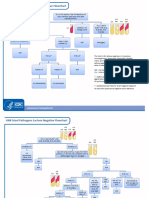
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- EAR First AidDocument4 pagesEAR First Aidr_lakshmi2722No ratings yet
- HMM1414 Chapter 5 Part 1Document56 pagesHMM1414 Chapter 5 Part 1Luqman Al-Bashir FauziNo ratings yet
- Pembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyDocument11 pagesPembrolizumab Plus Pemetrexedplatinum For Metastatic Nonsquamous NSCLC KEYNOTE 189 Japan StudyasdffdsaNo ratings yet
- Delivery Nurses NotesDocument2 pagesDelivery Nurses NotesRS Buenavista67% (3)
- Ospe Prep: Question 2 of 20 2.5 PointsDocument7 pagesOspe Prep: Question 2 of 20 2.5 PointsJaden Monique JamesNo ratings yet
- Distribution of ABO and RH-D Blood Group Antigens Among Blood Donors in The Amhara Regional State, EthiopiaDocument11 pagesDistribution of ABO and RH-D Blood Group Antigens Among Blood Donors in The Amhara Regional State, EthiopiaSely wulan widya ningsihNo ratings yet
- Low Flow Vascular Malformations ManagementDocument23 pagesLow Flow Vascular Malformations ManagementVedarth DashNo ratings yet
- Medical Terminology Chapter 3Document5 pagesMedical Terminology Chapter 3Gregg ProducerNo ratings yet
- KERENDIA Doctor Discussion Guide - FINALDocument2 pagesKERENDIA Doctor Discussion Guide - FINALajaygajaNo ratings yet
- RADIOTHERAPHYDocument20 pagesRADIOTHERAPHYMuhammad Hafiz KarimNo ratings yet
- Tataamalan HIRARC 2020Document42 pagesTataamalan HIRARC 2020Khaty JahNo ratings yet
- The Family Addict: A Review of The LiteratureDocument11 pagesThe Family Addict: A Review of The Literaturemiksi7906No ratings yet
- Normal Hemodynamic Parameters and Lab Values - Reference CardDocument4 pagesNormal Hemodynamic Parameters and Lab Values - Reference Cardblanquishem100% (1)
- 155 Latest Drugs - Neet PG Next PG Ini Cet FmgeDocument16 pages155 Latest Drugs - Neet PG Next PG Ini Cet FmgeSamikshya NayakNo ratings yet
- Sono PDFDocument3 pagesSono PDFJeyarajasekar TtrNo ratings yet
- Nutrition - Ginseng and BacopaDocument10 pagesNutrition - Ginseng and BacopaSynapgen ArticlesNo ratings yet
- Assessment of Renal and Urinary Tract FunctionDocument40 pagesAssessment of Renal and Urinary Tract FunctionBjorn Francisco100% (1)
- Acid Reflux Home RemedyDocument72 pagesAcid Reflux Home RemedySuresh UmadiNo ratings yet
- A Brief History of Mental Health CareDocument3 pagesA Brief History of Mental Health Carexiang jinNo ratings yet
- Christian Medical College VelloreDocument167 pagesChristian Medical College VelloreElisa 1209No ratings yet
- IPC M8 BloodbanksLabs PDFDocument54 pagesIPC M8 BloodbanksLabs PDFMaryam AimanNo ratings yet
- Feldenkrais Method Empowers Adults With Chronic.4Document13 pagesFeldenkrais Method Empowers Adults With Chronic.4Yvette M Reyes100% (1)
- Correspondence Codes May 2011Document208 pagesCorrespondence Codes May 2011Eric KohnkeNo ratings yet
- Hiv/Aids Stadium Iii With Opportunistic Infection: (Laporan Kasus)Document4 pagesHiv/Aids Stadium Iii With Opportunistic Infection: (Laporan Kasus)yantiNo ratings yet