Professional Documents
Culture Documents
2003 - Muscle and Nerve - Origins and Early Descriptions of Duchenne Muscular Dystrophy
Uploaded by
CZ. FANGOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
2003 - Muscle and Nerve - Origins and Early Descriptions of Duchenne Muscular Dystrophy
Uploaded by
CZ. FANGCopyright:
Available Formats
MEDICAL HISTORY ABSTRACT: One of the seminal events in the history of neurology was the
identification of primary diseases of muscle and their separation from dis-
eases in which muscle weakness was secondary to injury involving the
anterior horns of the spinal cord (“progressive muscular atrophy”). Not
surprisingly, one of the first groups of primary muscle diseases to be satis-
factorily characterized belonged to what would today be classified as mus-
cular dystrophies. Pride of place in this group belongs to Duchenne muscu-
lar dystrophy (DMD). DMD’s primacy as the first well-characterized muscular
dystrophy was due both to the fact that it is relatively common, as well as to
the clinically striking feature, apparent in many cases, of apparent paradox-
ical enlargement of severely weakened muscles (“pseudo-hypertrophy”).
This review traces the historical roots of DMD in the 19th century, from the
early papers by Conte, Bell, Partridge, and Meryon through the classic
monographs by Duchenne and Gowers. In addition, the first American
contributions to DMD are reviewed, including those by Pepper, Hammond,
and S. Weir Mitchell. Many of the original papers describing this disease are
now unavailable outside of major medical libraries, and several important
contributions, excepting those of Duchenne, which are recognized epony-
mously, are now virtually forgotten.
Muscle Nerve 28: 402– 422, 2003
ORIGINS AND EARLY DESCRIPTIONS OF
“DUCHENNE MUSCULAR DYSTROPHY”
KENNETH L. TYLER, MD
Department of Neurology B-182, University of Colorado Health Sciences Center
and Neurology Service, Denver Veterans Affairs Medical Center,
4200 East 9th Avenue, Denver, Colorado 80262, USA
Accepted 28 April 2003
Isolated cases of what almost certainly represent and arms, are strong. There is no defect percepti-
Duchenne muscular dystrophy (DMD) were initially ble in the evacuation of the bladder or of the
bowels. . . .The paralytic debility of the muscles
described in the first half of the 19th century.2,14,21,22 came on gradually; he was first sensible of it at a
These early depictions generally present patients public school, about eight years ago. It began with
with childhood onset of slowly progressive weakness a weakness in the thighs, which disabled him from
beginning typically in the legs, and occurring in the rising; and it is now curious how he will twist and
absence of associated sensory findings or other signs jerk his body to throw himself upright from his
seat.4
to suggest spinal cord disease. For example, in 1830,
the eminent English physician Charles Bell (1774 – At nearly the same time, a series of physicians in
1842) briefly described a Case of Partial Paralysis of the Italy described two brothers with progressive weak-
Lower Extremities (Case LXXXIX).4 The patient was a ness, but emphasized for the first time the associated
man of 18 in whom: finding of striking enlargement of affected muscles,
and the development of contractures as the disease
All the muscles of the lower extremities, the hips, progressed. In 1836, Gaetano Conte (1798 –1858)
and the abdomen, are debilitated and wasted. . . .
He has no defect of sensibility in the lower extrem- and L. Gioja in the Annali Clinici dell’Ospedale degli
ities. The upper part of the body, the shoulders, Incurabili di Napoli (The Clinical Annals of the Hos-
pital for Incurables of Naples) reported on these
brothers in a paper entitled “Scrofola del sistema
Abbreviations: DMD, Duchenne muscular dystrophy muscolare”(Scrofula of the muscular system).10,11
Key words: Becker muscular dystrophy; Duchenne muscular dystrophy;
Gowers’ sign; historical aspects; muscular dystrophy; pseudohypertrophic This paper was almost certainly not reviewed in its
muscular dystrophy original form by later authors on the subject, who
Correspondence to: K.L. Tyler; e-mail: ken.tyler@uchsc.edu
typically referenced a synopsis of its contents pre-
© 2003 Wiley Periodicals, Inc.
pared in a widely circulated yearbook which ab-
stracted foreign medical proceedings,50 or an even
402 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
later mention in another case synopsis.3 Unfortu- to be “somewhat larger than normal . . .[and]
nately, the errors in the yearbook citation, which seemed to want to stick out of the mouth as it did not
were perpetuated by later authors in reviews, and the have enough room.” Nicola had difficulty with
inaccessibility of the original Italian article, virtually speech, swallowing, and chewing, “augmented by the
guaranteed that Conte and Gioja’s contribution enlarged size of the masseters.” His tendons seemed
would become lost to posterity. Inspired by Dubo- “thinner and harder” than normal and he had flex-
witz’s lament about the lost article,14 Giovanni Nigro, ion contractures so that,
whose father had been a Department Head at the
Ospedale degli Incurabli in Naples, was able to lo- The forearm was in semiflexion over the arm and
cate the original paper,45 and have it republished in the fingers over the palm so that he could not
the Italian journal Cardiomyology (1986).11 Unfortu- bend nor extend the arm to bring it close to his
nately, this journal ceased publication in 1988, and chest. The thighs were in flexion over the abdo-
men and the legs over the thighs, which formed a
was never indexed by Medline/PubMed, so the pa-
very acute angle so that the heels touched the
per again lapsed into obscurity. glutei. The feet were also distorted so that the
Conte and Gioja describe two brothers who de- dorsum was on the same line with the external
veloped progressive muscular hypertrophy particu- malleolus and the plantar aspect was in line with
larly localized in the calves and deltoids.10,11 They the internal malleolus so that it seemed they were
mention that the two brothers had previously been reversed.
briefly described by another Italian physician, Gio-
vanni Semmola (1793–1865) in 1829, with their dis- In summarizing the case, Conte and Gioja noted:
ease described as “Ipertrofia muscolare” (muscular “We should remember that the main problem con-
hypertrophy), in a report to the Accademia Pontani- sists in a disease that primarily consists of a patho-
ana in Naples. Unfortunately, we have not yet been logical increase in size of the neuromuscular system
able to locate this report, which if presented in 1829 with a change in. . .the relationship of muscles, of
would have antedated Bell’s description by a year, their tendons, and the bones.”
and made these two brothers the first reported cases They felt that the hypertrophy was not due to
of DMD. Alan and Marcia Emery located a paper by changes in nonmuscular components (e.g., blood
Semmola published in 1834, but not the earlier 1829 vessels), nor was it due simply to contraction or
report,21 so the chronology and priority remain un- rigidity of muscles, as this would not be expected to
settled. increase muscle volume. They speculated that it was
The two described brothers developed a syn- caused by a change in the “nutritional process” lo-
drome of progressive leg weakness. Beginning at cally (i.e., in the muscle itself). They also stressed
about the age of 8 –10 years, the boys “found them- that hypertrophy alone was not the only factor in the
selves victims of a strange disease manifested by the disease, as this would not explain the associated
muscles, especially those of the lower extremities finding of loss of the “natural plasticity” of the in-
growing in size without, however causing any discom- volved muscles. Nor was the process simply akin to
fort.” The older of the two boys was more severely continuous muscle contraction as seen in tetany, as
afflicted and died “with signs of an enlarged heart” tetanic spasms did not result in increase in muscle
as a teenager. By age 17, the younger brother
volume. They lamented the unfortunate fact that no
(Nicola Caruso) was “unable to carry out any volun-
autopsy was available, “as an autopsy would have
tary movement and in this state he presented himself
helped us in determining if the connective intramus-
at this hospital [Hospital for Incurables in Naples].”
cular tissue was increased. . .as we see in people who
He was found to have hypertrophy of several muscle
groups including especially the deltoids; the right have paralysis.” They speculated that if the muscles
one being enlarged “approximately three times the contained an “accumulation of extraneous sub-
normal volume.” He had lesser enlargement of the stances” that this might stretch the fiber beyond its
biceps, triceps, brachialis, and other arm muscles, normal range, making it “lose its irritability and con-
which were noted “to have a certain hardness about tractile force.”11
them.” His abdominal and paraspinal muscles were These early cases must be considered suggestive
also enlarged and seemed “hard and rigid.” In the rather than definitive, for the clinical descriptions
legs, the glutei and quadriceps “had grown three are sparse and there is no description of pathology.
times the normal size. Also the gastrocnemii muscles Both these objections would be overcome in the
were triple in size.” Hypertrophy was also seen in the next decade with the reports of the English physi-
tibialis anterior. Interestingly, the tongue was noted cians Partridge and Meryon.
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 403
FIRST PATHOLOGICAL EXAMINATIONS OF CASES: terial from two of the cases that prompted Meryon to
PARTRIDGE AND MERYON present a detailed report to the Society in 1851,
The first pathological examination of a patient with based on patients he had first seen in November
DMD was probably that of Richard Partridge (1805– 1848. His first patient, the oldest brother, was the
1873), who described a case to the Pathological So- Honorable George P (Honorable being a title of
ciety of London at the meeting on November 15th, respect denoting the patient’s membership in a no-
1847.46,47 It would be almost impossible from his ble family). As a young child, it was noted that “he
brief description of the clinical features to be sure of walked heavily” and that when lifted from the
the diagnosis, but the same case and his affected ground by his nurse “he seemed to be a dead weight,
siblings were described a few years later by both having no power of assisting or jumping from the
Edward Meryon38,39 and William Little.37 Partridge’s ground.” Despite these early symptoms, he was still
patient (corresponding to Case E.H. of Meryon,39 able at age 6 or 7 to walk a mile without resting. By
see below), was a 14-year-old boy who, along with his the age of 8, his condition began to deteriorate. At
brother, developed weakness beginning in the prox- that time,
imal muscles of the arms and legs. As Meryon later He ascended stairs with the greatest difficulty, by
noted, “He could not stand when he was two and a holding the balusters and dragging the leg which
half years old. . ..he was, however, always conspicu- was furthest from them after him: this latter diffi-
culty increased more rapidly than that of walking
ously weak, as was also his brother, and in both it was
on a level surface. He was always disposed to trip,
observed that they never ran, jumped, or played with and could never make the slightest effort to re-
other children.”39 The brothers had great difficulty cover himself.39
going up stairs, “laying hold of the balusters with A local surgeon suspected this his difficulties were
both hands, then leaning the head on the hands and due to “deficient elongation of the spinal cord” and
fixing themselves in that bent attitude, they dragged prescribed a “procrustean plan of treatment” that
their legs after them.” Meryon later (see below) ob- included use of a spinal “stretching-board.” By the
tained additional information from the boys’ father, age of 11, the child could no longer walk even a step
“Who informed me that just before the loss of power and could scarcely stand. An operation to divide his
became apparent, the limbs grew thick and heavy; Achilles tendons and those of four other muscles,
from him I also ascertained, that he had two daugh- and the use of mechanical supports (“irons”) ap-
ters. . .who were perfectly free of the disease in ques- plied to the feet and legs, resulted in transient im-
tion.” The oldest boy died of pneumonia complicat- provement. In 1850, at the age of 16, the boy died of
ing measles and was autopsied. The muscles were a febrile upper respiratory illness. Meryon was noti-
not examined microscopically, but grossly: fied by telegraphic dispatch and was able to perform
The deltoid and sternomastoid muscles had under- an autopsy.
gone fatty degeneration. The calves (which were He noted that the body was generally emaciated,
larger than natural, and had, during the progress “more especially the lower extremities. . .there was
of the paralysis, become permanently contracted) great lateral curvature of the spine. The knees and
presented a greater degree of fatty degeneration in hip-joints were rigidly fixed in a bent position.” The
their muscular structure than the upper extremi-
ties, the soleus and gastrocnemius being more af- brain, spinal cord, and nerves were all essentially
fected than the flexor longus pollicis; neither the normal in appearance, but the muscles showed
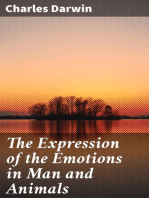
nerves nor the tendons had undergone marked abnormalities (Fig. 1).
change.39,46,47
The chief structural change existed in the system
of voluntary muscles, which was throughout the
Credit for the first unequivocal clinical and patho-
entire body atrophied, soft, and almost bloodless;
logical depiction of DMD goes to Edward Meryon and, although the muscular fibres appeared to exist,
(1807–1880) who submitted a paper entitled, “On yet they were not of that deep red colour as seen in
granular and fatty degeneration of the voluntary the natural state. When the muscular tissue was
muscles” on November 28th, 1851 (read on Decem- examined under the microscope, the striped ele-
mentary primitive fibres were found to be com-
ber 9th) to the Royal Medical and Chirurgical Soci-
pletely destroyed, the sarcous element being dif-
ety of London.38,39 Meryon’s paper contains descrip- fused, and in many places converted into oil
tions of three families, “P,” “H,” and “Tyrrel.” The globules and granular matter, while the sarco-
“P” family included 10 children in which all 4 of the lemma or tunic of the elementary fibre was broken
brothers aged 2 to16 years (and none of 6 girls aged down and destroyed.39
5 to17 years) were afflicted by progressive muscular At the time Meryon was performing his examina-
weakness. It was the availability of pathological ma- tions, microscopy of pathological specimens, such as
404 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
FIGURE 1. Photographs of the muscle biopsy from Meryon’s cases of DMD.39
muscle tissue, was still in its infancy. Meryon was a history of Meryon’s “P” family, and a series of illus-
founding member of the Microscopical Society of trations that were almost identical to Gowers’ own
London in 1839,21 and was apparently assisted in his (see below).
studies by a fellow member, the Honorable and Rev- Had his initial patient occurred in isolation,
erend Lord Sidney Goldolphin Osborne (see Meryon told his audience,
Meryon, 1864, who refers to “my friend” Osborne as, I should not have presumed to occupy your time
“an accomplished microscopist, [who] has for many and attention with the details which I have given;
years taken a lively interest in these cases of granular but a second son, the Hon. G. Wr. P--, four years
degeneration of the voluntary muscles, and has younger than the former, exhibited precisely the
spent much time in examining the different tissues same physical condition and the same symptoms as
did his brother at the same age.
obtained at the post-mortem investigation” [of
“W.P.” (Case 86)].40 Gowers would later refer to an A third son (Honorable Wm. P.) born in 1845 was
unpublished pamphlet by Reverend Osborne enti- also “much in the same condition as were his broth-
tled “The construction of voluntary muscle with ref- ers at that age.” This child is likely the case Meryon
erence to muscular degenerative disease, as seen in described in more detail in 1864 as “W.P.” (Case
certain cases with observations on that disease, by a 86).40 He died of pneumonia at the age of 14. Au-
member of the Microscopical Society.”27 In this pam- topsy showed that the brain and spinal cord ap-
phlet, Osborne provided additional details about the peared healthy, a point Meryon later reemphasized
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 405
in response to Duchenne’s accusations that his pa- [The boys] began to lose the muscular power in
tients were in reality simply cases of progressive mus- their legs when they were about twelve years of age,
from which epoch they became gradually worse,
cular atrophy rather than Duchenne’s own disease and when they were twenty their legs were useless;
(see below). As Meryon noted in response, their arms then began to fail them, and at the age
of twenty five both legs and arms were totally dis-
I may here state, that in the examination I made of
abled.39
the spinal cord of G.P... I traced the nerve-fibres of
many of the anterior nerves into the anterior cor- Meryon felt that “defective nutrition” of the muscles
nua; therefore I should have noticed an atrophied was important in the pathogenesis of the disease and
state of the anterior roots had it existed.40
directed his treatments to restoring what he felt was
In distinction to this normal result, Meryon noted likely an unhealthy condition of the blood, for which
(Fig. 1): purposes he used iron and a fibrin-rich diet. To
enhance circulation to the muscles, he felt that “ex-
The chief structural change existed in the system
of voluntary muscles, some of which, especially ercise of all the muscles is of paramount importance,
those of the lower extremities, were ochery in co- and when the disease is far advanced, artificial exer-
lour, and when examined under a microscope, in cise should be substituted.” He also utilized electrical
many places the striped elementary primitive fibres stimulation to try to reproduce the electrical cur-
were found to be completely destroyed, the sar- rents normally produced by “molecular interchanges
cous element being diffused about in the form of
granular matter, whilst the sarcolemma or tunic of in the muscles themselves” and which “exert a
the elementary fibre was broken up and de- healthy influence on the nervous system by main-
stroyed.40 taining its function.”
Meryon initially felt that the weakness in his pa-
Meryon placed particular emphasis on the “breaking
tients was due to disease of the spinal cord, and he
up of the sarcolemma” which he saw in these cases,
was not dissuaded from this viewpoint until he had
noting that it differed from, “the atrophy of muscles
an opportunity to perform a careful gross and mi-
which supervenes on lesions of the nervous centres
croscopic examination of George P.’s spinal cord
or on simple disuse.”40
and nerves, which revealed “not the slightest trace of
The “H” family included two boys. The older
disease.”
(“E.H.”) “could not stand when he was two and a half
years old” and was always conspicuously weak, as was I was therefore wrong in my diagnosis, for the
also his brother, and in both it was observed that nervous tissues had preserved their integrity; and
they never ran, jumped, or played with other chil- the only structural change observed was that which
presented itself in the muscular fibres, which were
dren. broken down, and converted into granular and
fatty matter.
When between eight and nine years of age they
both manifested the same kind of muscular weak- He also noted astutely that this fatty degeneration
ness which I have described in the other cases, did not simply insinuate itself between or displace
except that the arms were affected before the legs.
In both the diminution of power was most marked muscular fibers but rather filled the sheath of what
in going up stairs, which was affected by laying was formerly muscular fiber. Meryon went on to
hold of the balusters with both hands, then leaning review what was then known about different types of
the head on the hands, then fixing themselves in fatty deposition and their etiologies. He did not feel
that bent attitude they dragged their legs after that the changes he had seen were similar to those
them.39
found in disuse following paralysis or other “defalca-
As Meryon noted, it was this child (E.H.), who died tion of nervous energy” but rather due to some
of measles pneumonia, in whom autopsy showed intrinsic “deficiency of the elements” in muscle itself
that “all the voluntary muscles were wasted, retaining that somehow prevented its necessary consumption
a fibrous appearance, but were flabby and of a yel- [metabolism] and healthy assimilation.
lowish colour.”39 Meryon then went on to describe In 1864,40 1866,41,42 and again in 1870,43 Meryon
the pathological appearance of the muscles in detail, described additional cases of progressive muscular
quoting from Partridge’s earlier report.46,47 weakness under the title of “granular degeneration
Meryon’s final family (Tyrrel) is of interest for of the voluntary muscles,” clearly grouping them as
their later onset of illness, and are likely to have examples of the same disorder he had originally
represented the first description of what would later described in 1851.38,39 Unfortunately, several of
be called the Becker variant of DMD. All three broth- these later cases are less straightforward and differ in
ers in the family were affected, though their sister many ways from the originals. These later reports
remained entirely well. undoubtedly contributed to Duchenne’s subsequent
406 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
claim that Meryon had not described cases of LITTLE’S CASES
“pseudohypertrophic muscular paralysis” but rather In 1853, the year after Meryon’s description, William
of “progressive muscular atrophy,” a point that J. Little (1810 –1894), an English orthopedic sur-
Meryon went to great lengths to refute.40 – 43 In sup- geon who would achieve fame for his early descrip-
port of his argument, Meryon quoted no less an tions of cerebral palsy, published a monograph en-
authority than Jean Cruveilhier, the great French titled, On the Nature and Treatment of Deformities of the
pathologist who had first noted atrophy of the ante- Human Frame, which was based on lectures he had
rior roots in cases of atrophic paralysis. Cruveilhier delivered a decade earlier at the Royal Orthopedic
had told the members of the French Academy of Hospital.1,37 In a 3-page footnote, he described two
Medicine (after reviewing the illustrations of the siblings with DMD, noting the characteristic
muscle pathology in Meryon’s papers) that this was a pseudohypertrophy, and providing the third (after
form of paralysis, “non encore decrite” (not previ- Partridge and Meryon) gross and microscopic de-
ously described).41,42 scription of the muscle pathology. His patients were
The sparse clinical descriptions and lack of sup- two brothers, aged 12 and 14, whom he had seen in
porting pathological material in many of Meryon’s consultation in September 1847. Little saw his first
later case reports makes it impossible to identify patient 14 months before Meryon saw his original
their exact nature, although several patients had case, but did not publish his description until a year
forms of limb-girdle dystrophy similar to what would after Meryon’s original report. As noted by the
later be described by Leyden and Mobius. For exam- Emerys,21 the family described by Little was almost
certainly the same one described by both Partridge
ple, in 1866, Meryon described a woman aged 24 and
in November 1847 and Meryon in 1851 (Case E.H.).
a man aged 22 from a group of nine siblings.41,42
Both boys had “abnormal increase of bulk of muscle,
Both patients developed weakness in the legs and a
combined with contraction and adipose degenera-
waddling gait, then difficulty ascending stairs and
tion.” This was accompanied by “very general paral-
flexing their thigh muscles, followed by weakness in ysis, of the neck, trunk, the upper and lower extrem-
the feet and toes. Ultimately both patients also de- ities.” The older boy (“A.”) had delayed motor
veloped arm weakness. The woman eventually “lost milestones and had “never crawled” and had only
all voluntary motions of her arms and hands.” Nei- “walked alone weakly from table to chair at age of
ther patient had pain, nor did they experience the nineteen months.” Later acquiring the ability to
“quivering or starting” (fasciculations) of the dis- walk, he progressively deteriorated and by age 9 was
eased muscles, which Cruveilhier had previously de- unable to stand unassisted. He developed progres-
scribed in the case of Prosper Lecomte, the first sive contractures of the heel which made him stand
autopsied case of motor neuron disease. No new on his toes. At age 11, it was noted that “the muscles
pathological studies were available from either case, of his calf were as large as those of a well-grown
although Meryon accompanied his report with re- man.” His arms “showed atrophy generally of both
productions of the muscle biopsy from one of his shoulders and upper arms. . . except the deltoids. . .
1851 cases (Wm. P.). In 1870, Meryon described are larger in proportion to the remainder of the
another family in which two girls (ages 10 and 14) shoulder and upper arms; these muscles, however,
and their 3-year-old brother developed progressive do not possess any voluntary power.” He had slight
weakness beginning in the muscles of the legs and contractures at the elbows and of the pronators of
then progressing “centrifugally.”43 The oldest child the arms.
was the most severely affected: “She can no longer
stand, and her arms are beginning to be implicated He possesses very slight power in shoulders or
elbows, more in wrist and fingers. . .The muscles of
in the disease.” Her younger sister had a “waddling the calf are at present larger than those of a
gait” associated with, “gradually increasing weakness healthy boy of the same age; he possesses power of
of the muscles of the back and legs.” Weakness oc- volition in them; slight volition also apparent in
curred in the absence of pain or “any indication of anterior tibial, long and short extensor muscles of
nervous disturbance” and without, “the quivering or the toes, although these muscles are overcome by
contracture of the calf.
starting of the diseased muscles which Cruveilhier
has remarked in the cases he has described as “atro- His younger brother (“B.”) had a similar but milder
phie musculaire progressive.”43 As noted, although affliction. Neither boy had any intellectual deficits.
exact diagnosis is problematic, these children may Interestingly, the older boy did have some transient
have had limb girdle dystrophy of the type later sensory signs and symptoms and “has complained of
described by Leyden and Mobius. sensation of ‘pins and needles’; at one period the
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 407
FIGURE 2. Duchenne’s original patient (Case I, Joseph Sarrazin) from a photograph (A) taken by Duchenne,16 and as reproduced in
drawings (B) based on these photographs.15,17–19
legs and feet could be pinched without his being scribed the disease in the second edition of his De
aware of it.” However, Little noted that “sensation is L’Electrisation Localisee. . . (1861),15 under the head-
now perfect.” ing of “Paraplegie hypertrophique de l’enfance de
Shortly after Little examined the boys, the older cause cerebrale” (Hypertrophic paraplegia of in-
one died and came to autopsy. “At the autopsy the fancy of cerebral origin). The first case (Joseph Sar-
gastrocnemii and solei were found to be uncom- razin, Observation LXVIII, Case I) appeared under
monly large, colour whitish yellow; traces only of the heading, “Paraplegia cerebrale, congenitale, hy-
muscular tissue; the mass being composed of adi- pertrophique” (Cerebral paraplegia, congenital, hy-
pose matter.” The deltoid, sternomastoid, posterior pertrophic). Duchenne personally photographed Jo-
tibial, and hand muscles were involved to a milder seph Sarrazin, and included drawings made from
degree. “The degenerated muscles exhibited abun- these photographs in several of his papers (Fig.
dance of fat cells, with few traces of muscular fibre;
2).15–19 It was not until 1865 that he had his first
in some fibrillae the transverse markings were
opportunity to examine “muscular fibres removed
scarcely distinguishable.” There was no abnormality
during life from different parts of one of my little
in the interior of the brain or “medulla spinalis.”
There can be little doubt that the families de- patients” utilizing an instrument he had specially
scribed by Partridge, Meryon, and Little exhibited all designed for intra vitam muscle biopsy (his “emporte
the cardinal features of DMD, and from a modern piece histologique,” often more colorfully referred
perspective it would be difficult to deny Meryon’s to in England as a “histologic harpoon”). He later
claim to priority in providing the “first” comprehen- provided expanded and detailed analysis of 13 of his
sive descriptions of DMD. own cases.17–19,49,54
Duchenne was clearly aware of Meryon’s cases,
and referred repeatedly to Meryon’s original paper39
CLASSIC DESCRIPTIONS BY DUCHENNE
but insisted that these earlier cases represented ex-
Duchenne (1806 –1875)14,21,35,36 saw his first case of amples of progressive muscular atrophy and not of
DMD in his private clinic in 1858, and briefly de- his disease.17,18 Essentially all subsequent authorities,
408 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
including Gowers (see below), felt that the disorders tached to the disorder.27,29 In England, Gowers, the
described by Meryon and Duchenne were identical, leading authority on the disease (see below) ac-
a conclusion endorsed by modern experts and hard knowledged (but was somewhat piqued by) this ten-
to dismiss.21 After Meryon presented one of his cases dency, noting that Duchenne’s name was also com-
to the Royal Medical and Chirurgical Society in Feb- monly applied to glosso-labial paralysis and that,
ruary 186642 and reiterated his claim to priority, one “The increasing number of diseases and structures
of those present noted: called after men’s names constitutes a serious diffi-
culty for the student, and a frequent cause of confu-
In reference to the author’s statement regarding a
recent speaker at the Paris Academy of Medicine sion in medical writings, especially abroad.”28
[Duchenne], who had claimed the merit of being As noted, Duchenne saw his first patient (Case I),
the first to notice the malady now under discus- Joseph Sarrazin, in early 1858, when the patient was
sion, it should be remembered that French medi- 7 years old (Fig. 2). Joseph had difficulty in learning
cal men rarely read English periodicals and seldom
to stand and walk, and weakness in his legs was first
speak the language; hence no one ought to be
surprised if professional questions occupying at- noted when he was 8 to10 months old. He began to
tention in England do not always become known walk much later than his siblings. At age 21⁄2 years,
beyond the Channel. In proof of this, he would “He could not walk except with legs spread apart for
mention that at the library of the learned body just lateral balance (swinging gait) and somewhat
named no English medical journal is accessible for
arched.”17,18 By the age of 3 years,
perusal. . ..Therefore Dr. Meryon need not deem it
strange whenever any French observer thinks him- . . .his mother noted that his lower extremities
self an original discoverer, seeing the circum- grew in volume. Her attention was first drawn to
stances above related may furnish a satisfactory this by the enlargement of his calves which entered
explanation of the assumption narrated.42 his stockings with difficulty. . .the excessive devel-
This explanation may have been comforting to opment of the lower extremities had progressed
during 2 years.17,18
Meryon, but by 1868 was clearly incorrect, as Du-
chenne devoted several pages of his monograph to Duchenne noted that the gastrocnemius and lumbar
reviewing the symptomatology of Meryon’s cases and spinal muscles seemed to bulge through the skin, com-
then another section to arguing that the pathological menting: “I was not a little surprised to learn that these
features of the cases indicated that they were better athletic appearing muscles had been lacking power
subsumed as examples of progressive muscular atro- since birth and had hardly been exercised.”17,18 All the
phy.17,18 Duchenne conceded that the clinical features movements of the legs were very feeble. Despite this
of Meryon’s cases were in fact typical of pseudohyper- enfeeblement, all the muscles initially responded per-
trophic muscular paralysis, but felt that the “fatty de- fectly to electrical stimulation, although he subse-
generation of muscle fibres” illustrated were typical of quently found that this, too, would disappear in ad-
that seen in a variant of progressive muscular atrophy. vanced disease. The patient’s condition deteriorated,
Duchenne then also claimed priority for this observa- with the weakness ultimately spreading to the upper
tion, noting that he had first described similar cases in extremities. The child was bedridden by age 12 despite
a communication to the Academy of Sciences under treatment with electrotherapy, hydrotherapy, and mas-
the name “muscular atrophy with fatty transformation” sage. He died of tuberculosis (“phthisis”) at age 14.
in 1849, and hence, “The honor of this discovery be- Unfortunately, there was no autopsy.
longs completely to France.” Another notable patient that Duchenne de-
In his descriptions in 186817,18 and 1872,19 Du- scribed in 186817,18 was Case XII. Duchenne also
chenne replaced his initial suggested name for the photographed this 10-year-old boy, and drawings
disease (hypertrophic paraplegia of infancy) with a made from these photographs appeared in many of
revised clinical name, “pseudo-hypertrophic muscu- his papers and were widely reproduced (Fig. 3). The
lar paralysis,” to reflect the fact that further observa- boy had not walked until the age of 26 months, and
tion of his early cases made it clear that weakness and even then did so in a “clumsy manner.” Up until age
muscular changes were not just limited to the legs, 8, he was quite ambulatory, walking a kilometer each
but spread as the disease advanced to involve the day to school. However,
back and arms, and that pathological studies had not
supported a cerebral etiology. He also suggested an . . .little by little walking became more difficult, to
alternative name, “myo-sclerotic paralysis,” more re- the degree which the limbs, always very volumi-
nous, took on an unwanted development, then
flective of the disease’s pathology. However, it was after a time movements became almost impossible,
the name pseudo-hypertrophic muscular paralysis, at this point, every time the child fell he was inca-
along with Duchenne’s eponym, that became at- pable of getting up.
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 409
FIGURE 3. Duchenne’s Case XII is in the center (F. 11), “showing atrophy of the pectorals. Almost all the other muscles have a
hypertrophic appearance.” The surrounding images are muscle specimens “from subjects affected with pseudohypertrophic paralysis of
differing severity; showing the considerable quality of connective and fibrous interstitial tissue.” Muscle biopsy specimens from patients
with DMD at 45⫻ magnification illustrate the “considerable quantity of connective and fibrous interstitial tissue” (F. 12–F. 14). The same
specimens at 200⫻ magnification (F. 15–F. 18). A normal muscle specimen (F. 19). “Different degrees of fatty degeneration of the muscle
fiber” (F. 20 –22). “Necrosis of the muscle fiber” (F. 23a) and “proliferation of elements of fibrous tissue” (F. 23b).17
Duchenne noted: “On my first examination, I was development to that of the famous Farnese Hercules
struck, not only by the extraordinary volume of the (Fig. 4), and to the muscles seen in some of Mich-
muscles, but also by their firmness, even when relaxed. elangelo’s paintings. However, as Duchenne noted:
This child was the patient of Bergeron, a col- The Farnese Hercules is the ideal of physical
league of Duchenne’s, who compared his muscle strength in antique statuary. . . . It would be a mis-
410 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
FIGURE 4. The Farnese Hercules (A), widely considered in the 19th century to represent the ideal body form. The original marble statue
was widely reproduced, and copies exist in various sizes of plaster and bronze, as well as in a number of engravings including those by
Jacob Bos (c. 1520) (B), and Hendrik Goltzius (c. 1592) (C). The artist was the Roman sculptor Glykon who made the statue for the Baths
of Caracalla in the 3rd century A.D., probably using an earlier statue by the Greek sculptor Lysippus (325 B.C.E.) as a model. The statue
was discovered in 1546, and was displayed in the courtyard of the Farnese Palace, from which it acquired its name. Interestingly, the legs,
which apparently caught the attention of Duchenne and others as an example of extreme muscular development, were originally missing
and were replaced by copies made by a pupil of Michelangelo, until the originals were located.
understanding of its esthetic beauty to compare it 6. Absence of fever, sensory disturbance, and im-
with the monstrous musculature of hypertrophic pairment of the functions of the bladder and
paralysis. . . .Current pathological study reveals
that this excessive development of the musculature
intestine during the entire course of the dis-
is a sign of weakness. Pathological anatomy will ease.17,18
show that these muscle contours, in appearance so
formidable, are formed principally by muscles
Cognizant of criticism that he often failed to
stuffed with interstitial connective tissue and inter-
stitial fibrosis.17,18 obtain pathological support when he described
“new” diseases, he provided only a limited account in
Summarizing this original case and 12 others, Du- the second edition (1861)15 of De L’Electrisation locali-
chenne noted that there were six principal diagnos- see. . . . As he noted in the 3rd edition (1872):
tic features of pseudohypertrophic paralysis:
I have been much blamed abroad for having, in
1. Decrease in strength, at the beginning of the the different pathological investigations which I
disease, usually in the muscles of the lower limbs. have published, neglected and despised patholog-
ical anatomy, that branch of science inseparable
2. Lordosis and spreading of the lower limbs on from all good clinical work. I recognized the re-
standing and walking. proach, and wished to expose myself to it no
3. Excessive development of volume, during a sec- longer. I waited in vain for an autopsy to furnish me
ond stage, either of some or all of the weakened with an opportunity of examining the condition of
muscles. the muscles whose size has increased so excessively,
and seeking for an explanation of the two contradic-
4. Progressive course of the disease, during a third tory facts co-existing in my little patients, viz., paresis
stage, with worsening of the paralysis and with its or paralysis and muscular hypertrophy.19,49
generalization if it was limited to the inferior
members. It was to overcome this dependence on autopsy ma-
5. Decrease or abolition of electromuscular contrac- terial that Duchenne developed his “histological har-
tility in an advanced stage of the disease. poon” (Fig. 5). “Thanks to this instrument I have
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 411
of the disease, free from fear of criticism17,18 (see Fig.
3 for examples of muscle biopsy specimens from
Duchenne’s cases). He found that “hyperplasia of
the interstitial connective tissue, with the production
of more or less fibrous tissue, is the fundamental
anatomical lesion of the muscles in pseudohypertro-
phic paralysis.”17,18,49 It was this increase in non-
muscle tissue that “produces the considerable and
sometimes monstrous increase in muscle volume,
which is in direct proportion to the quantity of hy-
perplastic interstitial connective and fibrous tis-
sue.”17,18 He also observed, “slight or moderate num-
bers of fatty vesicles,” especially in advanced
cases.17,18 The transverse striations of muscle fibers
could become extremely fine, or even disappear in
some affected areas, followed by similar obliteration
of the longitudinal striations until ultimately the
“sarcolemma seems to contain fatty vesicles.”17,18
Obtaining an autopsy in a DMD patient was of
critical importance as, although the muscular
changes seemed unequivocal, it was essential to de-
termine whether there would be changes in the
anterior horns of the spinal cord, analogous to those
seen in cases of infantile atrophic paralysis. Meryon,
FIGURE 5. Duchenne’s histologic harpoon (emporte piece his-
tologique), the first instrument designed specifically for perform-
whose case was the first autopsied, had not found
ing muscle biopsy.17 The cavity for collecting the muscle speci- such changes, as mentioned earlier.39 In 1865,
men is clearly seen in the two right-hand illustrations. Cohnheim added a second autopsy on a patient of
Eulenberg’s,23 clearly showing that the spinal cord
been able to complete my clinical observations by was normal. Duchenne was not able to obtain an
research into the pathological condition of the mus- autopsy on a case until 1871, when the second child
cles of living patients.”19,49 Griesinger, in Germany, he had biopsied (Case XII, see above) died.20 After
had performed the first biopsy during life from the fixing some muscle specimens in chromic acid, “Be-
deltoid muscle of a 13-year-old boy with DMD in ing desirous of giving additional value to their histo-
186432 (Fig. 6), but the procedure was difficult, re- logical examination, I requested my friend M. Char-
quired ether anesthesia, and was complicated by an cot to be good enough to assist me in it” (see
infection that lasted several weeks. Nonetheless, this Charcot5). Duchenne gave additional pieces of mus-
early effort and its associated case report often led to cle to Lockhart Clarke, probably the foremost expert
German authors assigning Griesinger equivalent pri- on microscopic neuroanatomy in England (see be-
ority to Duchenne in the description of DMD. low).
Duchenne developed his “histological harpoon” The microscopic examination of these specimens
to simplify intra vitam muscle biopsy, and to avoid showed the muscular changes of pseudo-hypertro-
the pain, obviate the need for ether anesthesia, and phic paralysis in an extreme degree, i.e., the mus-
decrease the risk of infection (which could become cular fibres smaller than usual, but still preserving
as a rule faint striation, and separated from each
a fatal complication in the pre-antibiotic era). By
other by a large quantity of fatty tissue, mixed with
1865, Duchenne had used his tissue punch to obtain fibrous tissue and wavy fibres in small quantity.19,49
fragments of the gemellus and deltoid muscles in an
8-year-old boy with pseudohypertrophic paralysis As Charcot himself noted (Fig. 7):
(1868, Case VII), noting that “from that moment I With respect to the state of the spinal cord, our
possessed all the necessary elements for a complete observations were made on transverse sections, co-
depiction of pseudohypertrophic paralysis.”49 In loured with carmine. . ..These sections have, be-
1867, he was able to add details based on micro- sides, been very numerous, and were taken from
different parts of the cervical and dorsal regions of
scopic analysis of a second biopsied case, which con- the cord. I should here notice that the muscles
firmed his previous observations, allowing him fi- which receive their nerves from the cervical en-
nally to provide the long-delayed detailed depiction largement were, for the most part affected to a
412 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
that the spinal roots, both anterior and posterior,
appeared also perfectly sound.6,7
There can be no question of the magnitude of Du-
chenne’s contribution. In his books and mono-
graphs, he managed to outline virtually all the car-
dinal clinical features of DMD, save only its heredi-
tary component. He identified the key pathological
findings, and clearly recognized that DMD repre-
sented a primary disease of muscle rather than the
secondary effects of disease within the spinal cord or
brain. Although Duchenne was not the first to rec-
ognize the uniqueness of muscular dystrophy as a
separate clinical species, the clarity and quality of his
observations justify his eponymous recognition. It
would remain for Duchenne’s contemporary, the
great British neurologist, Sir William Richard Gow-
ers, to put the final touches on the clinical picture
based on a large series of both personal and re-
ported cases, and to clearly identify DMD as an
inherited disorder with a striking predilection for
males.
GOWERS AND THE ENGLISH CONTRIBUTION
In England, Sir William Richard Gowers
(1845–1915),12,51 one of the greatest neurological
clinicians of the era, developed an early and abiding
interest in DMD, and even had an opportunity to
examine relatives of Meryon’s original cases.29 Gow-
ers saw his first cases of DMD (Cases 19 –22 from
Gowers 27) “very early in his medical work,” probably
between 1860 –1863 while he was serving as a medi-
cal apprentice, as these patients all lived in the
neighborhood where he worked at that time.12,27 His
first cases were members of a family of 10 children in
which 3 of the 7 boys and none of the 3 girls were
affected. Gowers reported his first case of DMD in
1874, a boy in whom he was able to obtain a
FIGURE 6. (A) Griesinger’s case. A 13-year-old boy with DMD,
the first patient to undergo muscle biopsy during life (July necropsy8(Case 17 in his later monograph27). He
1864).32 (B) Drawings of the muscle biopsy from this patient.32 subsequently discussed and presented 21 personal
cases in lectures delivered at the National Hospital
for the Paralysed and Epileptic and to medical stu-
high degree, and that the deltoids, among others, dents at University College (1879).26 These lectures
exhibited most markedly the characteristics of hy- were published in the The Lancet, and later expanded
pertrophy by fatty substitution. If, in this case, the into a monograph entitled Pseudo-Hypertrophic Mus-
muscular lesions had been connected with spinal cular Paralysis (1879),27 which became the definitive
lesions the latter should not have failed to show
themselves well marked in the cervical enlarge- English-language account of the disease. Near the
ment of the spinal cord. Now, the result was abso- end of his active career, Gowers returned to the
lutely negative. . .the grey substance, which was the subject of DMD in lectures he delivered at the Na-
subject of a very special investigation, presented no tional Hospital in 1902 30 and 1908.31 The last of
trace of alteration. The anterior cornua were nei- these lectures was unfortunately only published in
ther atrophied nor deformed. . .and the motor
cells, normal in number, did not present, in the Pitman shorthand, in a long defunct and vanishingly
several parts which go to constitute them, any de- obscure journal known as the Phonographic Record of
viation from the normal type. Let us remember Clinical Teaching and Medical Science.53
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 413
FIGURE 7. (Right) Transverse section of a muscle from a patient with DMD from Charcot.6 “G” indicates ‘adipose cells,’ “M,”
cross-sections of muscular fascicles, and “I,” islets of connective tissue. (Left) Longitudinal section from a more advanced case showing
isolated muscle fibers, deprived of their fibrillary envelope, and put in immediate contact with cells of the adipose tissue. The muscle
fascicles, even the smallest, have preserved their transverse striations (note variation in size of muscle fibers).6,7
Gowers’ poignantly noted: dence of the disease. Harvey S. did not have obvious
muscular wasting or enlargement, but was already
The disease is one of the most interesting, and at
the same time most sad, of all those with which we experiencing difficulty in rising from the floor. Gow-
have to deal: interesting on account of its peculiar
features and mysterious nature; sad on account of
our powerlessness to influence its course, except in
slight degree, and on account of the conditions in
which it occurs. It is a disease of early life and early
growth. Manifesting itself commonly at the transi-
tion from infancy to childhood, it develops with
the child’s development, grows with his
growth—so that every increase in stature means an
increase in weakness, and each year takes him a
step further on the road to hopeless infirmity, and
in most cases to an early and inevitable death.26,27
Gowers publicly presented early cases of this disor-
der to audiences at the National Hospital in 1879.
For several years, he had followed a family with six
afflicted members in two generations. In the second
generation, four of the six brothers were afflicted,
including a 12-year-old (Arthur S., Case 5), a 7-year-
old (William S., Case 4), a 4-year-old (Harvey S., Case
3), and a 3-year-old (name not specified, no case
number) (Fig. 8). Two brothers aged 4 and 10 were
apparently healthy. Gowers was intrigued by the fact
that one of the apparently normal brothers was the
FIGURE 8. Two brothers aged 4 (Harvey S, Case 3) and 7
twin of Harvey S., who was clearly severely afflicted. (William S, Case 4) from Gowers. “The youngest. . .would not
Neither of their parents appeared affected, although suggest to you the idea of disease. There is no obvious muscular
the mother’s only brother and one of her four sisters wasting or enlargement, and yet. . .his movements were greatly
had both died of an apparently similar illness, each impaired. He could only just succeed in rising from the
at the age of 15. This latter case, in a girl, repre- floor. . ..The other boy. . .as his photograph indicates, [has] very
distinct enlargement of the calves. His thighs are small, the back
sented one of only three females afflicted with the thin, hollow in the lumbar region, the angles of the scapulae
disease in his personal series of 21 cases. None of the prominent, the muscles of the upper limbs thin, except the del-
children of the unaffected sisters had shown evi- toids, which are rather large.”27
414 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
his thighs higher and higher, and so by. . .climbing
up his thighs he apparently pushes his trunk up. I
wish to call your special attention to this peculiar
action, because it is probably pathognomonic of
the disease. Attention was called to it by Duch-
enne, and I have never seen it absent in a case so
long as the patient possessed the necessary muscu-
lar power. I have never seen it in any other disease,
and every doubtful case in which it was present
ultimately proved to be an example of the affec-
tion. Its diagnostic importance is thus very great.26,27
This peculiar method of arising from the floor (Figs.
9 and 10) would subsequently be referred to as
“Gowers’ sign,”52 although as Gowers himself ac-
knowledged,26,27 Duchenne had described the phe-
nomena previously, as had other earlier observers
(see below).
In addition to describing the changes in muscle
size and power, Gowers noted that several patients
had absent patellar reflexes (an aspect of the clinical
examination that was first described in 1875, and for
which Gowers himself had previously suggested the
term knee-jerk). Gowers also emphasized the aspects
of the clinical examinations that were spared in
DMD. Patients such as David W had a clear and
sharp intellect, no evidence of involvement of either
general or special sensibility, and no involvement of
the sphincters.
In both David W and Arthur S (Cases 1 and 5),
Gowers noted that the Achilles tendon seemed
“tight,” hindering the ability of David W to place his
heels flatly on the ground when standing, and, in the
case of the more severely afflicted Arthur S, the
associated calf contraction was so extreme “that the
FIGURE 9. Gowers’ sign.27 “He helps himself up in a very pecu- heels are drawn up and the feet are in a line with the
liar way— by putting his hands upon his knees, and grasping his legs.” A third patient illustrating this point (Edward
thighs higher and higher, and so by. . .climbing up his thighs he
pushes his trunk up.”
Gloster, E.G., Case 10) was also presented (Fig. 11)
allowing Gowers to comment that he had not seen
this “extreme shortening of enlarged muscles” in any
ers noted that “He could only just succeed in rising other disease. In contrast to these changes at the
from the floor, getting first his toes upon the ankle, which could occur early in the disease, other
ground, then placing first one hand upon his knee, contractures tended to be late manifestations.29 For
then the other, and so working himself up.” William example, contraction of the knee flexors often led to
was more seriously affected. He had distinct enlarge- fixation of the knee-joint, and contraction of the
ment of his calves (Fig. 8), small, thin thighs and biceps in the presence of a weakened triceps could
back, an obvious lumbar lordosis, and prominent have the same effect at the elbow. Exaggerated an-
angled scapulae. His arms were also thin, except for tero-posterior curvature of the spine also often oc-
the deltoids, which seemed enlarged. He also had curred early, followed later by exaggerated lateral
wasting of his sternocleidomastoid muscles. curvature (Fig. 11).
In addition to presenting members of the S fam- Gowers was not fooled by the apparent enlarge-
ily, Gowers also presented a 9-year-old boy (David W) ment of some muscles, and clearly noted that these
(Case 1) to his audience, and described his similarly muscles were always weaker than normal. He noticed
affected brother. Noting again: that the disease had a predilection for particular
. . .he helps himself up in a very peculiar way— by muscles. Enlargement, which was not invariably
putting his hands upon his knees, and then grasping present, was generally greatest in the calf, and one
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 415
FIGURE 10. Gowers’ sign as it actually appeared in a child of 12 with muscular dystrophy seen at the Bicetre Hospital in Paris in 1891,
as illustrated by Dejerine.13 “These nine figures represent the different positions taken for passing from the lying to the standing position.”
12-year-old boy in his care had a calf circumference fected muscles to electrical stimulation. Using both
of 141⁄2 inches!29 After the calf, the next most com- faradic and galvanic currents, he found that weak-
monly enlarged muscles were the infraspinati and ened muscles had diminished excitability. As noted,
the deltoids. Other muscles that were often enlarged he was able to examine both the gross and micro-
included the quadriceps and the glutei, and less scopic pathology in one of his patients8 (Case 17 of
commonly the triceps and biceps. Weakness was gen- ref. 27), and he made several astute pathological
erally most marked in the hip flexors and extensors observations. For example, he noted upon section-
and quadriceps,29 a fact that contributed to postural ing the muscle in one case that “it was difficult to
instability, led most patients to stand with their feet believe that the section was that of a muscle,”26 it
far apart, and resulted in frequent falls induced by appeared rather more like a “fatty tumour” or a
even slight disturbance of balance. The pattern of “mass of adipose tissue.”8 Microscopically he found
muscle involvement also led to a peculiar “oscillat- isolated groups of thin muscular fibers in the midst
ing” gait26,27,29 in which the body “inclined from side of “cells distended with homogenous fat” and “fi-
to side” as the patient walked. brous tissue containing many nuclei and elongated
Although few diagnostic tests were available in cells” (Fig. 12). Gowers’ colleague, Lockhart-Clarke,
Gowers’ era, he did examine the reactions of af- probably the premier nervous system microscopist of
416 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
FIGURE 11. Gowers’ patient, Edward Gloster (E.G., Case 10).27
his era, assisted with the examination of the spinal
cord. Although some pathological changes were
noted, they found that with rare exceptions the “an-
terior cornua [horns] were conspicuously healthy,”
the cells corresponding perfectly in size, sharpness,
length, and distinctness of processes to those found
in healthy spinal cords. Gowers emphasized how
strikingly this finding contrasted with the abnormal
state of the spinal cord in patients with progressive
muscular atrophy, in whom similar, severe muscular
wasting was invariably associated with virtually com-
plete loss of anterior horn cells. Despite some con-
fusing abnormalities present in the spinal cord in
some areas in his DMD cases, Gowers concluded that
“pseudohypertrophic paralysis of early life is not a
disease of the spinal cord.” He also concluded that
there was no real evidence supporting ideas that the
muscle disease resulted indirectly as the conse-
quence of involvement of either sympathetic or tro-
phic nerves.
In 1879,26,27 Gowers reviewed evidence support-
ing the view that that DMD was a primary disease of
the muscular tissue, and approvingly quoted Fried-
reich’s conclusion that it represented “a congenital
nutritive and formative weakness of the striated mus-
cle substance.”24 By 1888, having had an opportunity
to analyze more pathological specimens, he was un-
equivocal: “The significance of the pathological FIGURE 12. Muscle specimen from Gowers (Case 17)27 (Figs. 1
anatomy is that the malady is a primary disease of the and 2 originally appeared as Figs. 7 and 8 in ref. 8). “Under the
microscope the resemblance to a fatty tumour was also strikingly
muscles.” Gowers felt, like his contemporary Du-
close. Cells distended with homogenous fat covered the field.
chenne, that the fibrous changes in muscle, rather Passing among the fat-cells, however, were narrow bands, which
than the muscle atrophy itself, was likely to be the consisted of fibrous tissue and muscular fibres.”
primary pathological process in DMD. He hypothe-
sized that the wasting of the muscular fibers was
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 417
secondary to an overgrowth of the interstitial con- ered.” He cautioned that the prognosis “must be
nective tissue elements.29 Gowers felt that fatty re- influenced by the period at which the disease com-
placement was responsible for the enlargement of mences, and by its observed rate of progress” with
the muscles and that the interstitial fibrous tissue both early onset and rapid progression heralding a
might be responsible for the shortening and contrac- worse prognosis. He also noted that the prognosis
tion of muscles that he had frequently observed. was generally less grave in girls than boys. Death was
Gowers summarized the “special characters of not the result of the disease itself, but from intercur-
the disease” based on his experience with 21 cases. rent illness, notably pneumonia caused by weakness
“The first fact which deserves notice is its remarkable and wasting of thoracic muscles and impaired respi-
relation to sex. It commonly affects boys, very rarely ratory power, events that led to death in 13 of the 19
girls.” He noted that sex influenced not only the personal cases for which he had information.
frequency but the severity of the disease, with the Treatment, as noted, was of little avail. Gowers
presentation in girls often seeming to be milder and noted:
of later onset. “The next important fact in the con-
As a congenital developmental malady, pseudo-
ditions of the origin of the disease is its tendency to
hypertrophic paralysis is one of those diseases in
affect several members of the same family.” He which medicine is necessarily powerless to cope
noted that he had seen families with up to six af- with the essential elements of the process. As may
fected members in a single sibship and that Meryon’s be, therefore, expected, no drug has been found
original family, whose collateral relatives he had to exert an influence on the course of the affec-
tion.29
later examined, had eight affected brothers (and no
affected daughters). This led him to conclude that Among the agents he tried were arsenic, phospho-
“It might naturally be expected that a disease which rus, iron, strychnine, and cod-liver oil. Electrical
thus evidently depends on conditions which are con- stimulation of the muscles had “disappointed the
genital, and not acquired, should be distinctly he- expectations which had been formed of it,” a con-
reditary, and the facts I have just mentioned show clusion also shared by Duchenne. Muscular exercise
that it is so in some cases.” He noted that “the disease did seem to have some effect in retarding the weak-
is never to be heard of on the side of the father; ness.29 He felt that patients benefited from “carefully
always when antecedent cases have occurred, they planned gymnastic exercises, so arranged as to call
have been on the side of the mother,” a “very re- into action the muscles that most need help.”29 Rub-
markable fact in the etiological conditions” that he bing and passive movements of the limbs partially
referred to as unilateral inheritance.26,27 It was this counteracted the tendency to contracture and defor-
interesting pattern that later led him to conclude mity.26,27,29 Section of the Achilles tendon occasion-
that “thus the congenital tendency is exclusively due ally resulted in improvement in a patient’s ability to
to the maternal element in the embryo,”29 a fact that stand or walk,26,27,29 and “mechanical appliances”
he felt was “also shown by a fact many times observed enabled patients to use their legs for a longer time
that the children of the same women, by different than would otherwise be possible.
husbands, suffer in the same way.”29 Later he refined The contributions of Duchenne, Gowers, and
this idea to conclude that the “developmental ten- others firmly established the basic clinical and patho-
dency which constitutes the malady comes from the logical features of DMD, and lead to its acceptance
ovum and not from the male element in the germ.”31 as a unique clinicopathological entity in Europe.
This, in turn, led him to the interesting speculation The basic features of DMD were summarized in lead-
that, since the disease affected the ovum and appar- ing American medical journals, and lead rapidly to
ently only those ova destined to become males, this the first reports of similar cases in the United States.
made it, “probable that the sex of the future embryo
is also determined in the ovum”!31
EARLY AMERICAN CONTRIBUTIONS
Age of onset represented a third important etio-
logical fact of the disease. Gowers recognized that In contrast to the seminal contributions made by
DMD was a disease of early life, commencing in the French, English, and German physicians, American
majority of his cases before the age of 6. He noted, contributions to the early history of DMD were quite
“As a rule (to which there are exceptions), the more modest. In 1868 and again in 1870, Meredith Clymer
severe the disease the earlier does it commence.” provided competent reviews of DMD based on the
Gowers recognized the dire prognosis of the dis- literature, but gave no indication he had actually
ease, noting, “it is doubtful whether any case in seen a case.9 The first American patient described in
which the symptoms were well marked has recov- the literature was a child (J.S.) seen by Ingalls and
418 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
Webber at the Boston Children’s Hospital in Sep-
tember 1870.34 Like Clymer’s paper, this report is
more notable for its review of published literature on
DMD than for its rather sparse case report. At the
age of 3, J.S.
. . .began to move and act as though he had less
strength than usual. . .this condition increased and
the spinal column became very weak, and the “in-
ward crook” of it was noticed. . ..We asked him to
stand upon the floor, and he walked a few steps in
a tottling or shambling manner.
It was noted that Duchenne’s illustrations of his
cases were also a “perfect picture” of J.S. and that,
“the muscles of the calves were largely developed.”
The paper by Ingalls and Webber was followed in
the next year by additional cases from eminent
American physicians, including William Pepper,48 S.
Weir Mitchell,44 (see also Gerhard25 for a later de-
scription of the same patient), and William Ham-
mond.33 In contrast to that of Ingalls and Webber,34
the report by Pepper,48 based on a case he had seen
in the Philadelphia Hospital in April 1871, was re- FIGURE 13. Pepper’s original case (W.E.)48 of DMD (probable
markably detailed and comprehensive. Pepper was Becker variant) at age 20. W.E. was one of the first American
cases illustrated, and one of the first American patient’s to un-
correct when he noted that “it is the first case of this dergo muscle biopsy (1871).
disease that has been carefully studied and described
in this country.” He commented in a footnote: “Un-
fortunately and unavoidably, the report of the case action is perfect.” He noted in particular that “the
[by Ingalls and Webber], which serves as the intro- calves appear as large as those of a vigorous man,
duction to the[ir] paper, is very meagre.” Pepper contrasting very strangely with the wasted thighs.
provided an original illustration of his patient (Fig. They feel quite firm, even when relaxed.” Foreshad-
13), where Ingalls and Webber34 had simply repro- owing Gowers, but not Duchenne who had already
duced one of Duchenne’s. noted a similar phenomena, Pepper noted:
Pepper’s case was unusual, as it likely represented When about to stand up, he throws his body for-
what would today be considered an example of the ward till it almost rests on his thighs, and then,
Becker variant of DMD. His patient (W.E.) was 20 placing his hands on his knees and rising a little
when first seen. At age 14, he had noticed “gradually from his seat, he slowly raises his body by sliding his
increasing loss of strength in the legs, which pro- hands up his thighs; and when he has raised him-
self as far as possible this way, he places one hand
gressed so slowly that for eighteen months he was after the other on a chair-back or edge of a table,
still able to run about, though not so actively as other and leans forward. He then, by jerks of the alter-
boys.” By age 18, he began to use a cane. During the nate sides of the body, draws his legs forward, thus
first 3 years of symptoms, the patient had noted assuming more and more nearly an erect posi-
atrophy beginning in the muscles of the calves, then tion.48
progressing to the thighs, back, and later the shoul- Pepper and his Philadelphia colleague, William
ders and arms. Hammond, were the first American physicians to
perform a muscle biopsy in DMD. As Pepper noted,
About two years ago [age 18], after the atrophy of
the muscles of the calves had become very marked, “I obtained a small scrap of muscular tissue, by
he noticed that they began to increase in size, and means of an ‘emporte piece’ from both gastrocnemii
this growth had continued until they have ac- and the left deltoid muscles. These have been sub-
quired a size much greater than they ever had jected to careful microscopic study.” In the gastroc-
previously. . .during all this time his weakness has nemii, he found:
steadily increased.
A few fibrils presented streaks of minute fatty gran-
Pepper also noted that his intellect was intact, that ules along their centres, and a very small number
he had no sensory or bladder impairment, and that were decidedly fatty. The muscular fibres varies
the “muscles of the face are not involved, and their greatly in size also. . ..There was a large excess of
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 419
that the legs are those of an infant athlete sur-
mounted by a body of ordinary dimensions. . . .I
have been tempted, like other describers, into
speaking of the overdeveloped limbs as being like
those of an athlete; but, in fact, both in this and the
two other cases seen by me, the calves are not
symmetrical, and in the present case they are en-
larged too low down, and on the inside of the calf
there is some flattening, so they fail to offer the
appearance of overgrown, but well-formed limbs.
The whole of both legs, including the glutei, are
enlarged and hard. . . .The muscles attacked are
very firm. . . .The father of the lad declined to
permit me to examine the muscular tissue by Du-
chenne’s instrument for removing morsels of tis-
sue for microscopic study, so that I can only infer
as probable the existence of that form of hyperpla-
FIGURE 14. S. Weir Mitchell’s case,44 Robert Payne, the first sia of the muscular connective structures which
American patient with DMD to be photographed. gives to these cases the false appearance of muscu-
lar hypertrophy.44
Mitchell, like Pepper, also noted the patient’s pecu-
interstitial tissue, in places taking the form of long,
liar method of rising.44
narrow, wavy bands of pure white fibrous tis-
sue. . ..There was a considerable amount of inter- In the first edition of his textbook, William Ham-
stitial fat, existing as scattered globules, or ar- mond was able to describe and illustrate a single
ranged in patches of large, closely aggregated fat-
globules. In places isolated muscular fibrils lay
imbedded in this fibrous tissue so as to be scarcely
visible.48
At virtually the same time as Pepper saw his first
patient, his Philadelphia colleague, S. Weir Mitchell,
the dean of American neurologists, also saw his first
cases of DMD.44 In October 1871, Mitchell described
an 8-year-old boy (R.P., Robert Payne) that he saw a
month earlier at his clinic at the Orthopedic Hospi-
tal and Infirmary for Nervous Diseases. He noted
that he had also seen two other cases, suggesting that
he might have also seen the patient described by
Pepper. Unfortunately, he does not provide details
of these patients, but does describe R.P., and pro-
vides the first photographic illustration of an Amer-
ican patient with DMD (Fig. 14). R.P. was one of six
children, the others all apparently healthy. As Mitch-
ell noted:
When stripped, and examined, his posture and
external appearance presented some notable pe-
culiarities. While standing, the shoulders are
thrown back, the blades project, the belly is thrust FIGURE 15. Hammond’s original case of DMD.33 This patient,
forward, the feet four inches apart, and the spine along with the one shown in Figure 12, were the first American
curved forward in the dorso-lumbar region without cases of DMD to be illustrated, and the first American patients to
lateral deviation. . .above the waist, there is, with undergo muscle biopsy.33,48. The patient was a 7-year-old boy
one exception, nothing remarkable about the mus- with a “disinclination to learn to walk.” “At three years of age he
cular developments, which are such as belong to a could not stand longer than a few seconds, and even for this time
person of his age. Both deltoid muscles are unusu- he was obliged to spread the legs apart and to hold on to some
ally large and hard, and certainly much more con- article of furniture.” Hypertrophy was noted at age 5, first in the
spicuous than they should be. They alone, of all right calf, then left calf followed by the glutei. After removing the
the muscles of the upper extremities, seem to have muscle with the trocar of Duchenne, Hammond noted disintegra-
shared in all the pathological changes which have tion of muscle fibrillae with disappearance of their transverse
affected the lower limbs. Below the pelvic brim the striae, and the presence of large amounts of connective tissue
muscles are seemingly developed enormously; so (inset).
420 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
personal case first seen in March 1871.33 He saw a 6. Charcot JM. Lecons sur les maladies du systeme nerveux faites
a la Salpêtrière. Bourneville (editor), Vol. 2. Paris: Adrien
second child later that same year (May 1871) (Fig. Delahaye; 1877. p 258 –267.
15). This second patient may have been the first 7. Charcot JM. Lectures on diseases of the nervous system deliv-
American case to undergo muscle biopsy (Fig. 15). ered at La Salpetriere (2nd series). Sigerson G (translator).
London: The New Sydenham Society; 1881. p 217–224.
As Hammond noted, 8. Clarke L, Gowers WR. On a case of pseudo-hypertrophic
In the case under my care I have made repeated muscular paralysis. Medico-Chirurgical Transactions of the
examinations, removing the muscle with the trocar Royal Medical and Chirurgical Society of London 1874;57:
247–259.
of Duchenne.. . .The transverse striae are seen to
9. Clymer M. Lectures on the palsies and kindred disorders of
have disappeared, the fibrillae are in a state of the nervous system. Lecture III. Progressive myo-sclerosic
disintegration, and the connective tissue is present palsy. The Medical Record 1870;5:217–222.
in large amount.33 10. Conte G, Gioja L. Scrofola del sistema muscolare. Annali
Clinici dell’Ospedale degli Incurabili di Napoli 1836;2:66 –79.
The years that followed would see further enumera- 11. Conte G, Gioja L. Scrofola del sistema muscolare. Cardiomy-
tion of various subtypes of muscular dystrophy and ology 1986;5:15–28.
refinement of both electrophysiological and his- 12. Critchley M. Sir William Gowers 1845–1915: a biographical
appreciation. London: Heinemann; 1949.
topathological diagnostic testing for muscle disease. 13. Dejerine J. Trouble de la motilitie. In: Semiologie des affec-
The identification of specific gene defects in a vari- tions du systeme nerveux. Paris: Masson; 1914.
ety of dystrophies would usher in a new molecular 14. Dubowitz V. History of muscle disease. In: Rose FC, Bynum
WF, editors. Historical aspects of the neurosciences. New
era for understanding and classifying these disor- York: Raven Press; 1982. p 13–222.
ders. All these contributions, in turn, developed 15. Duchenne GBA. De l’electrisation localisee et de son appli-
from the astute observations of a small group of cation a la pathologie et a la therapeutique, 2nd ed. Paris:
Bailliere; 1861. p 353–356
clinicians, in Italy, England, France, Germany, and 16. Duchenne GBA. Album de photographes pathologiques.
the United States, who recognized the uniqueness of Paris: Bailliere; 1862.
a set of clinical cases and were able to separate out 17. Duchenne GBA. Recherches sur la paralysie musculaire pseu-
do-hypertrophique ou paralysie myo-sclerosique. Archives Ge-
these inaugural examples of a hereditary primary nerales de Medicine 1868; 6th series, 11:5–25, 179 –209, 305–
dystrophic process affecting muscle from the con- 321, 421– 443, 552–588.
founding surround of cases of inherited and ac- 18. Duchenne GBA. Recherches sur la paralysie musculaire pseu-
do-hypertrophique ou paralysie myo-sclerosique. Paris: P. As-
quired “spinal” muscular atrophies and other causes selin; 1868.
of progressive weakness. 19. Duchenne GBA. De l’electrisation localisee et de son appli-
cation a la pathologie et a la therapeutique, 3rd ed. Paris:
This review was presented in part at the annual meeting of the Bailliere; 1872. p 595– 616.
American Academy of Neurology, Honolulu, Hawaii, in April 20. Duchenne GBA. Note sur l’etat anatomique des muscles et de
2003. Dr. Tyler is supported by the Ruler-Lewin Family Professor- la moelle epiniere dans un case de paralysie pseudo-hypertro-
ship of Neurology. Assistance with German translations was pro- phique. Arch Physiol Norm Pathol 1872;4:228.
vided by Dr. Rolf Malessa, Chefarzt, Klinik fur Neurologie, So- 21. Emery AEH, Emery MLH. The history of a genetic disease:
phien-und Hufeland Klinik, Weimar, Germany, and with Italian Duchenne muscular dystrophy or Meryon disease. London:
translations by Dr. Piero Antuono, Professor of Neurology, De- Royal Society of Medicine; 1995.
22. Engel AG. Duchenne dystrophy. In: Engel AG, Banker BQ,
partment of Neurology, Medical College of Wisconsin, Milwau-
editors. Myology. Basic and clinical. New York: McGraw-Hill;
kee, Wisconsin. Mr. Ronald Bouchard helped with preparation of 1986. p 1185–1240.
illustrations. The author also gratefully acknowledges the assistant 23. Eulenberg A, Cohnheim R. Ergebnisse der anatomischen
of the staffs of the Dennison Medical Library at the University of untersuchung eines falles von sogenannter muskelhypertro-
Colorado School of Medicine, and of the Becker Medical Library phie. Berliner Medizinische Gesellschaft 1865;1:191–205 and
(Tyler collection) of the Washington University School of Medi- 1866;2:191–210.
cine in St. Louis. 24. Friedreich N. Uber progressive muskelatrophie, uber wahre
und falsche muskelhypertrophie. Berlin: Hirschwald; 1873. p
291.
25. Gerhard GS. Pseudo-hypertrophic paralysis. Philadelphia
REFERENCES Medical Times 1875:29 –32.
1. Accardo PJ. An early case report of muscular dystrophy. A 26. Gowers WR. Clinical lecture on pseudo-hypertrophic muscu-
footnote to the history of neuromuscular disorders. Arch lar paralysis. Lancet 1879;2:1–2, 37–39, 73–75, 113–116.
Neurol 1981;38:144 –146. 27. Gowers WR. Pseudo-hypertrophic muscular paralysis. Lon-
2. Adams RD. Diseases of muscle, 3rd ed. Hagerstown, MD: don: Churchill; 1879.
Harper & Row; 1975. p 262–265. 28. Gowers WR. Pseudo-hypertrophic paralysis. Br Med J 1880;1:
3. Barwinkel. Ueber muskellahmung in foge von hypertrophie 771.
des interstitiellen fett- und bindegewebes; von Dr. Sigmundt 29. Gowers WR. A manual of diseases of the nervous system.
in Tubungen (Arch f. klin. Med. I. 6. p. 630, 1866.) Schmidt’s Pseudo-hypertrophic muscular paralysis (muscular pseudo-
Jahrbucher der in-und Auslandischen Gesamten Medicin. hypertrophy, lipomatous muscular atrophy, etc.). Philadel-
Bonn, Germany: Marcus and Weber; 1866;130:285–286. phia: Blakiston; 1888. p 378 –393.
4. Bell C. The nervous system of the human body. London: 30. Gowers WR. A lecture on myopathy and a distal form. Br
Longman, Rees, Orme, Brown, and Green; 1830:clxiii. Med J 1902;2:89 –92.
5. Charcot JM. Note sur l’etat anatomique des muscles et de la 31. Gowers WR. Short lecture on pseudo-hypertrophic paralysis.
moelle epiniere dans un cas de paralysie pseudo-hypertro- Phonographic Record of Clinical Teaching and Medical Sci-
phique. Arch Physiol Norm Pathol 1872;4:228 –239. ence 1908;14:89 –92.
History of Duchenne Dystrophy MUSCLE & NERVE October 2003 421
32. Griesinger W. Ueber muskelhypertrophies. Archiv der Heil- 43. Meryon E. Case of granular degeneration of the voluntary
kunde 1865;6:1–15. muscles. Br Med J 1870;2:32–33.
33. Hammond WA. A treatise on diseases of the nervous system. 44. Mitchell SW. Pseudo-hypertrophic muscular paralysis. The
New York: Appleton; 1871. p 699 –705. Photographic Review of Medicine and Surgery 1871;2:1– 4.
34. Ingalls W, Webber SG. A case of progressive muscular sclero- 45. Nigro G. Conte or Duchenne? Cardiomyology 1986;5:3– 6.
sis, with a paper on the same. Boston Med Surg J 1870;6:321– 46. Partridge R. Fatty degeneration of voluntary muscle. Transac-
325. tions of the Pathological Society of London 1846 –1848;1:334.
35. Kennedy C. Guillaume Benjamin Amand Duchenne. In: Ash- 47. Patridge R. Fatty degeneration of muscle. Med Times Gaz
wal S, editor. The founders of child neurology. San Francisco: 1847;5:944.
Norman Publishing; 1990. p 227–237. 48. Pepper W. Clinical lecture. On a case of progressive muscular
36. Lhermitte J. Duchenne de Boulogne en son temps. Bull Acad sclerosis (pseudo-hypertrophic muscular paralysis of Du-
Med (Paris) 1946;130:745–755. chenne). Med Times (Philadelphia) 1871;1:329 –332, 349 –
352.
37. Little WJ. On the nature and treatment of deformities of the
49. Poore GV. Selections from the clinical works of Dr. Duchenne
human frame: being a course of lectures delivered at the
(de Boulogne). Chapter VI. Pseudo-hypertrophic paralysis, or
Royal Orthopedic Hospital in 1843: with numerous notes and
myo-sclerotic paralysis. London: The New Sydenham Society;
additions to the present time. London: Longman, Brown,
1883. p 173–191.
Green, and Longmans; 1853. p 14 –16.
50. Schmidt CC. Krankhafte hypertrophie des muskelsystems.
38. Meryon E. On fatty degeneration of the voluntary muscles. Mittheilung von den D Dr. Coste u. Gioja. Jahrbucher der
Lancet 1851;2:588 –589. in-und Auslandischen Gesamten Medicin. Leipzig, Germany:
39. Meryon E. On granular and fatty degeneration of voluntary O. Wigand; 1839;24:176.
muscles. Medico-Chirurgical Transactions of the Royal Med- 51. Tyler KL. Gowers, William Richard. In: Aminoff MJ, Daroff
ical and Chirurgical Society of London 1852;35:73– 84. RB, editors. Encyclopedia of the neurological sciences. San
40. Meryon E. Practical and pathological researches on the vari- Diego, CA: Academic Press; 2003. p 481– 484.
ous forms of paralysis. London: John Churchill & Sons; 1864. 52. Tyler KL, McHenry LC Jr. Fragments of neurologic history:
p 200 –215. pseudohypertrophic muscular dystrophy and Gowers’ sign.
41. Meryon E. On granular degeneration of the voluntary mus- Neurology 1983;33:88 – 89.
cles. Lancet 1866;1:258 –260. 53. Tyler KL, Roberts D, Tyler HR. The shorthand publications of
42. Meryon E. On granular degeneration of the voluntary mus- Sir William Richard Gowers. Neurology 2000;55:289 –293.
cles. Medico-Chirurgical Transactions of the Royal Medical 54. Wilkins RH, Brody IA. Duchenne’s muscular dystrophy. Arch
and Chirurgical Society of London 1866;49:45–50. Neurol 1968:18:628 – 636.
422 History of Duchenne Dystrophy MUSCLE & NERVE October 2003
You might also like
- The History of Spinal Surgery For Disc Disease An Illustrated TimelineDocument6 pagesThe History of Spinal Surgery For Disc Disease An Illustrated TimelineRashmi ShriNo ratings yet
- 1989 - The Duchenne Dystrophy StoryDocument11 pages1989 - The Duchenne Dystrophy StoryCZ. FANGNo ratings yet
- 53-Article Text-259-1-10-20190910Document7 pages53-Article Text-259-1-10-20190910Moe HeyNo ratings yet
- Thoracic Outlet Syndrome: A 50-Year Experience at Baylor University Medical CenterDocument12 pagesThoracic Outlet Syndrome: A 50-Year Experience at Baylor University Medical CentermerlyNo ratings yet
- Articulo 2Document11 pagesArticulo 2Erick Johan Otálvaro BermúdezNo ratings yet
- Spondylolysis and Spondylolisthesis: Costs and Adaptations of BipedalismDocument28 pagesSpondylolysis and Spondylolisthesis: Costs and Adaptations of BipedalismPancho ReyesNo ratings yet
- Functional Limb Weakness and ParalysisDocument16 pagesFunctional Limb Weakness and Paralysis955g7sxb8pNo ratings yet
- Models of Vertebral Subluxation - A ReviewDocument8 pagesModels of Vertebral Subluxation - A ReviewCambriaChicoNo ratings yet
- Spasmodic Torticollis - Review of 220 Patients: P. Rondot, M.P. Marchand and G. DellatolasDocument9 pagesSpasmodic Torticollis - Review of 220 Patients: P. Rondot, M.P. Marchand and G. Dellatolastiffanybell04No ratings yet
- Watson 2010Document10 pagesWatson 2010Oscar OsorioNo ratings yet
- Delirium Fogel MaldonadoDocument70 pagesDelirium Fogel MaldonadoNatalia Martinez CastroNo ratings yet
- Bonica Chapter 35 Myofascial PainDocument61 pagesBonica Chapter 35 Myofascial PainiqraNo ratings yet
- Reversed CoarctationDocument11 pagesReversed Coarctationdr sarangNo ratings yet
- A Circular Depression at The Spinoglenoid Notch of A Prehistoric Andean Scapula Titelbaum2019Document6 pagesA Circular Depression at The Spinoglenoid Notch of A Prehistoric Andean Scapula Titelbaum2019Girafa ElefanteNo ratings yet
- 01 Definition Sec1Document44 pages01 Definition Sec1Sindy Tatiana Valbuena Casallas0% (1)
- Accelerating research on language and cognition in motor neuron diseaseDocument10 pagesAccelerating research on language and cognition in motor neuron diseaseLlamadme ImanolNo ratings yet
- Dementia On The Byzantine Throne (330-1453) : Originalarticle:Epidemiology, ClinicalpracticeandhealthDocument8 pagesDementia On The Byzantine Throne (330-1453) : Originalarticle:Epidemiology, ClinicalpracticeandhealthIvanovici DanielaNo ratings yet
- The History of Osteoarthritis-Osteoarthrosis: J Dequeker, F P LuytenDocument7 pagesThe History of Osteoarthritis-Osteoarthrosis: J Dequeker, F P LuytenAggelos TrontzosNo ratings yet
- Kennedy Medico Legal AspectsDocument27 pagesKennedy Medico Legal Aspectsaswari putraNo ratings yet
- Phenomenology and Classification of Dystonia - A Consensus Update (2013)Document11 pagesPhenomenology and Classification of Dystonia - A Consensus Update (2013)mysticmdNo ratings yet
- Vilensky 2001Document5 pagesVilensky 2001Jean VictorNo ratings yet
- Physician's Call for Weather Bureau Collaboration on Studying Atmospheric Conditions' Impact on HealthDocument5 pagesPhysician's Call for Weather Bureau Collaboration on Studying Atmospheric Conditions' Impact on Health_Junz_No ratings yet
- Tatu 2014Document12 pagesTatu 2014Meysam KarmaNo ratings yet
- History of Miofascial SyndromeDocument5 pagesHistory of Miofascial SyndromeJorge LucasNo ratings yet
- A Longitudinal Study of Back Pain and RadiologicalDocument5 pagesA Longitudinal Study of Back Pain and RadiologicalSumanta KamilaNo ratings yet
- Presentation, Etiology, Diagnosis, and Management of CamptocormiaDocument9 pagesPresentation, Etiology, Diagnosis, and Management of CamptocormiaDianaKhasanovaNo ratings yet
- Historical Note: Marie Jean Pierre Flourens (1794-1867) : An Extraordinary Scientist of His TimeDocument1 pageHistorical Note: Marie Jean Pierre Flourens (1794-1867) : An Extraordinary Scientist of His TimeElelmoduNo ratings yet
- Vesalius Nervous System ImageDocument6 pagesVesalius Nervous System ImageXavier Guell ParadisNo ratings yet
- The History of PDDocument15 pagesThe History of PDMoileon2011No ratings yet
- 30-Second Anatomy: The 50 most important structures and systems in the human body each explained in under half a minuteFrom Everand30-Second Anatomy: The 50 most important structures and systems in the human body each explained in under half a minuteRating: 2 out of 5 stars2/5 (1)
- Alzheimer Disease Including Focal Presentations PDFDocument14 pagesAlzheimer Disease Including Focal Presentations PDFpiedrahitasaNo ratings yet
- Frozen Shoulder - Loss of Scapulohumeral RhythmDocument9 pagesFrozen Shoulder - Loss of Scapulohumeral RhythmWasemBhatNo ratings yet
- Triada de CharcotDocument1 pageTriada de Charcotdanitza pilcoNo ratings yet
- Aspectos Históricos de La Esclerosis MúltipleDocument6 pagesAspectos Históricos de La Esclerosis MúltipleMac Perez LopezNo ratings yet
- Clinical Progress: The CirculationDocument11 pagesClinical Progress: The CirculationFirdaus che matNo ratings yet
- The Lucid Interval Associated With Epidural Bleeding: Evolving UnderstandingDocument7 pagesThe Lucid Interval Associated With Epidural Bleeding: Evolving UnderstandingyosiaputraNo ratings yet
- ReviewDocument4 pagesReviewisisjadidNo ratings yet
- 227 FullDocument15 pages227 FullJ HL SanzNo ratings yet
- Perspectives: Ideas About Pain, A Historical ViewDocument10 pagesPerspectives: Ideas About Pain, A Historical ViewMarlyGabrielaSosaRojasNo ratings yet
- Schnecken Becken DysplasiaDocument4 pagesSchnecken Becken Dysplasiadr sutjiNo ratings yet
- Typhoid Spine: Somatic Versus Psychosomatic Diagnosis in Osler's TimeDocument10 pagesTyphoid Spine: Somatic Versus Psychosomatic Diagnosis in Osler's Timeaji gumelarNo ratings yet
- The Veterinary JournalDocument10 pagesThe Veterinary JournalJessica MerloNo ratings yet
- Clin Anat 07 Spinal Segmental Bone InnervationDocument5 pagesClin Anat 07 Spinal Segmental Bone InnervationOchiMataNo ratings yet
- DMP Distrophy Muscular ProgressivaDocument24 pagesDMP Distrophy Muscular ProgressivaDevi SiswaniNo ratings yet
- Patel 2013Document8 pagesPatel 2013joantyy 1No ratings yet
- The History of Me Arch of NeurolDocument6 pagesThe History of Me Arch of NeurolNEuRoLoGisT CoFFeeCuPNo ratings yet
- Earlyhistoricalliteraturefor Post-Traumaticsymptomatology: StressandhealthDocument10 pagesEarlyhistoricalliteraturefor Post-Traumaticsymptomatology: StressandhealthclinicapsicNo ratings yet
- Revisiting The Vertebral Venous Plexus BatsonDocument15 pagesRevisiting The Vertebral Venous Plexus BatsonMorteza Mazloom Farsi BafNo ratings yet
- 2004 History of Fibromyalgia - Past To PresentDocument10 pages2004 History of Fibromyalgia - Past To PresentJulian Caro MorenoNo ratings yet
- The Science of Signs and Symptoms: In Relation to Modern Diagnosis and Treatment: A Textbook for General Practitioners of MedicineFrom EverandThe Science of Signs and Symptoms: In Relation to Modern Diagnosis and Treatment: A Textbook for General Practitioners of MedicineRating: 5 out of 5 stars5/5 (1)
- Innervation The Human Shoulder Joint and Its Implications For SurgeryDocument6 pagesInnervation The Human Shoulder Joint and Its Implications For SurgerymitroisergiuNo ratings yet
- Degenerative Disc Disease of The Spine - From Anatomy To Pathophysiology and Radiological Appearance With Morphological and Functional ConsiderationsDocument14 pagesDegenerative Disc Disease of The Spine - From Anatomy To Pathophysiology and Radiological Appearance With Morphological and Functional ConsiderationswenhsiaochuanNo ratings yet
- The Prague School of Rehabilitation: Alena Kobesova, Neil OsborneDocument3 pagesThe Prague School of Rehabilitation: Alena Kobesova, Neil OsborneJoséGalindoMuñisNo ratings yet
- Frontotemporal DementiaDocument52 pagesFrontotemporal DementiaCarolina PradoNo ratings yet
- Human Rights DefinitionDocument2 pagesHuman Rights DefinitionFathiah MhNo ratings yet
- Ode To The Spell Checker TCHDocument1 pageOde To The Spell Checker TCHCamila PaulucciNo ratings yet
- Corporate History: World BankDocument3 pagesCorporate History: World BankPramod KhanvilkarNo ratings yet
- Part of Speech QuestionsDocument4 pagesPart of Speech QuestionsNi Luh Ari Kusumawati0% (1)
- Zanussi ZBF 569 Oven ManualDocument24 pagesZanussi ZBF 569 Oven ManualJoohlsNo ratings yet
- 2005 Mapex CatalogDocument20 pages2005 Mapex Cataloggiftsvav100% (1)
- Philips NTRX505Document28 pagesPhilips NTRX505EulerMartinsDeMelloNo ratings yet
- Lecture 1 (Introductory Class)Document23 pagesLecture 1 (Introductory Class)Amara SoOmroNo ratings yet
- Romanticism Day 1 LessonDocument5 pagesRomanticism Day 1 Lessonapi-312902028No ratings yet
- 01.shurangama Mantra - 1st VerseDocument1 page01.shurangama Mantra - 1st Versetrung tranNo ratings yet
- Gold V Essex CCDocument11 pagesGold V Essex CCZACHARIAH MANKIRNo ratings yet
- Introduction To Business ManagementDocument24 pagesIntroduction To Business ManagementZintle Mini0% (1)
- Report For Court, Sale of Dowling College Brookhaven CampusDocument26 pagesReport For Court, Sale of Dowling College Brookhaven CampusRiverheadLOCALNo ratings yet
- SCC800-B2 SmartSite Management System V100R002C00 Installation GuideDocument190 pagesSCC800-B2 SmartSite Management System V100R002C00 Installation GuideHamza OsamaNo ratings yet
- Welcome To HDFC Bank NetBankingDocument1 pageWelcome To HDFC Bank NetBankingrajeshNo ratings yet
- Russell Vs Vestil 304 SCRA 738Document2 pagesRussell Vs Vestil 304 SCRA 738Joshua L. De JesusNo ratings yet
- News TIA Portal V15 and V15 1 enDocument43 pagesNews TIA Portal V15 and V15 1 enjohanNo ratings yet
- Sensory Evaluation of FoodDocument38 pagesSensory Evaluation of FoodKHOZA SBUSISIWENo ratings yet
- Trust Law: Common Law Property Settlor Trustees Beneficiary FiduciaryDocument8 pagesTrust Law: Common Law Property Settlor Trustees Beneficiary FiduciaryDekweriz100% (1)
- Icon-Architects Executive Profile - For HealthcareDocument14 pagesIcon-Architects Executive Profile - For HealthcareMuhammad Noshad RizviNo ratings yet
- Me Project MHRDMDocument36 pagesMe Project MHRDMYatinMhapankarNo ratings yet
- Access 2013 Beginner Level 1 Adc PDFDocument99 pagesAccess 2013 Beginner Level 1 Adc PDFsanjanNo ratings yet
- 555 and 556 Timer CircuitsDocument16 pages555 and 556 Timer Circuitssiddharthmohta100% (2)
- MM Im Pi PiDocument19 pagesMM Im Pi Pim0use-outNo ratings yet
- Fatima! Through The Eyes of A ChildDocument32 pagesFatima! Through The Eyes of A ChildThe Fatima Center100% (1)
- CIMA Financial Accounting Fundamentals Past PapersDocument107 pagesCIMA Financial Accounting Fundamentals Past PapersAnonymous pwAkPZNo ratings yet
- Maceda Vs Energy Reg BoardDocument4 pagesMaceda Vs Energy Reg BoardJay Mark Esconde100% (1)
- G3335-90158 MassHunter Offline Installation GCMSDocument19 pagesG3335-90158 MassHunter Offline Installation GCMSlesendreNo ratings yet
- FentonTech Wastewater Ghernaout 2020Document29 pagesFentonTech Wastewater Ghernaout 2020BrankNo ratings yet
- Cut Nyak Dhien: Aceh's Legendary Resistance LeaderDocument5 pagesCut Nyak Dhien: Aceh's Legendary Resistance LeaderKhoerudin KhoerudinNo ratings yet