You might also like
- Controlling Microbial Growth in VitroDocument65 pagesControlling Microbial Growth in VitroCarl Elexer Cuyugan Ano100% (15)
- Speis Tradia Neo ReviewDocument18 pagesSpeis Tradia Neo ReviewGunther OrosNo ratings yet
- Lesson PlanDocument16 pagesLesson Plansingh2manish100% (4)
- Covid 19 & VaccinationDocument23 pagesCovid 19 & VaccinationclordNo ratings yet
- Wunner 2014Document19 pagesWunner 2014César VidezNo ratings yet
- RETROVIRIDAEDocument1 pageRETROVIRIDAEjcpacate1178qcNo ratings yet
- Hiv in Pregnancy FinalDocument73 pagesHiv in Pregnancy Finalapi-3797079No ratings yet
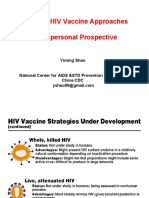
- Novel Vaccine Approaches (Yiming Shao)Document29 pagesNovel Vaccine Approaches (Yiming Shao)National Press Foundation100% (1)
- Hepatitis CCRN KFSH&RC Asma AlshehriDocument33 pagesHepatitis CCRN KFSH&RC Asma AlshehriasmashNo ratings yet
- Ese Hiv Flyer 04308 Low 0Document2 pagesEse Hiv Flyer 04308 Low 0Naveenan ChidambaramNo ratings yet
- Virus Hepatitis CDocument10 pagesVirus Hepatitis CAna Paola Ramírez LópezNo ratings yet
- Global Tuberculosis Report 2018 (WHO) PDFDocument277 pagesGlobal Tuberculosis Report 2018 (WHO) PDFRevan Radit-ya Emperor-Genk'zNo ratings yet
- Global Tuberculosis Report 2018 PDFDocument243 pagesGlobal Tuberculosis Report 2018 PDFDudungNo ratings yet
- Antiviral therapy, a lot has been achieved, yet far to goDocument39 pagesAntiviral therapy, a lot has been achieved, yet far to goThiago SantosNo ratings yet
- 1 3 Lab-Diagnosis TROP-DIS Total (April 22) PDFDocument92 pages1 3 Lab-Diagnosis TROP-DIS Total (April 22) PDFMartin BravoNo ratings yet
- 21 HPV GenoArray Diagnostic KitDocument8 pages21 HPV GenoArray Diagnostic KitYosinee PatrungsiNo ratings yet
- RetrovirusDocument5 pagesRetrovirusferdudz schneiderNo ratings yet
- Progress in Basic Research (Gary J. Nabel, M.D., PH.D.)Document56 pagesProgress in Basic Research (Gary J. Nabel, M.D., PH.D.)National Press FoundationNo ratings yet
- ShyFoundry Freeware EULADocument20 pagesShyFoundry Freeware EULANicolas YayaNo ratings yet
- Mammoth: Chapter 36: HIV & AIDSDocument14 pagesMammoth: Chapter 36: HIV & AIDSBreeanne GallonNo ratings yet
- Global TB ReportDocument277 pagesGlobal TB ReportTirza StevanyNo ratings yet
- Day 2 TB diagnostics_MacalaladDocument45 pagesDay 2 TB diagnostics_MacalaladRye CalderonNo ratings yet
- Chapter 6 Polyomaviruses SV40Document11 pagesChapter 6 Polyomaviruses SV40zahidNo ratings yet
- Viral Hepatitis PDFDocument4 pagesViral Hepatitis PDFNina BracyNo ratings yet
- Oxygen 2222Document75 pagesOxygen 2222Salim AlmetewtyNo ratings yet
- MVI: Accelerating Development of Malaria VaccinesDocument18 pagesMVI: Accelerating Development of Malaria VaccinesIbrahim HashimNo ratings yet
- AIDS Causes, Symptoms and TreatmentDocument48 pagesAIDS Causes, Symptoms and TreatmentMuhammad RidwanNo ratings yet
- MEDICAL VIROLOGY: VIRUSES CAN BE USEFULDocument82 pagesMEDICAL VIROLOGY: VIRUSES CAN BE USEFULBaydaa Hameed Al Abdali100% (1)
- Viruses Without 4th Shift VirusesDocument4 pagesViruses Without 4th Shift VirusesLyka MahrNo ratings yet
- Httpasttmoh - VNWP Contentuploads201505Tai Lieu Dao Tao HIV - Aids Trung Cap Y PDFDocument211 pagesHttpasttmoh - VNWP Contentuploads201505Tai Lieu Dao Tao HIV - Aids Trung Cap Y PDFhiep582008No ratings yet
- 2022 CHAI HIV Market Report 12.8.22Document45 pages2022 CHAI HIV Market Report 12.8.22Rakesh KumarNo ratings yet
- COVID-19: Nucleic Acid Diagnosis KitDocument26 pagesCOVID-19: Nucleic Acid Diagnosis KitEduward Paitan UrbinaNo ratings yet
- Introduction to Medical Virology BasicsDocument88 pagesIntroduction to Medical Virology BasicsSutapa PawarNo ratings yet
- HIV and Retroviruses: Transmission, Infections, and Oral ManifestationsDocument5 pagesHIV and Retroviruses: Transmission, Infections, and Oral ManifestationsArshu Shaik812No ratings yet
- 2018 KSU Shrimp Workshop - DharDocument31 pages2018 KSU Shrimp Workshop - DharRaju RamaiahNo ratings yet
- Human Papillomavirus Detection in Head and Neck Squamous Cell CarcinomaDocument8 pagesHuman Papillomavirus Detection in Head and Neck Squamous Cell CarcinomaDr Monal YuwanatiNo ratings yet
- HIV Prevention PresentationsDocument27 pagesHIV Prevention PresentationsAiman ButtNo ratings yet
- Virus Patho-ImmunologyDocument8 pagesVirus Patho-ImmunologySirwan SalmanNo ratings yet
- Antiretroviral Therapy: BasicsDocument46 pagesAntiretroviral Therapy: BasicsStrawberry ShortcakeNo ratings yet
- Farmakologi III (Antivirus)Document44 pagesFarmakologi III (Antivirus)candhawidiya santikaNo ratings yet
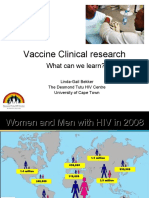
- Progress in Clinical Research (Linda-Gail Bekker MBCHB, DTMH, DCH, FCP (SA), PHD.)Document171 pagesProgress in Clinical Research (Linda-Gail Bekker MBCHB, DTMH, DCH, FCP (SA), PHD.)National Press FoundationNo ratings yet
- WVC Europe - Recombinant Nanoparticle COVID-19 Vaccine Platform Technology For EIDDocument28 pagesWVC Europe - Recombinant Nanoparticle COVID-19 Vaccine Platform Technology For EIDtheskeptic21No ratings yet
- SamDocument3 pagesSamAirell Takinan DumangengNo ratings yet
- GENE THERAPY ADVANCEMENTS BEYOND IMAGINATIONDocument17 pagesGENE THERAPY ADVANCEMENTS BEYOND IMAGINATIONJagtendra IndoliaNo ratings yet
- Covid PanelDocument66 pagesCovid PanelJoshua RuizNo ratings yet
- Summary of virology & immunologyDocument19 pagesSummary of virology & immunologyElaf NaifNo ratings yet
- Antiviral ChemotherapyDocument13 pagesAntiviral ChemotherapyCaleb MutugiNo ratings yet
- Viral OncogenesisDocument36 pagesViral OncogenesisyuanlupeNo ratings yet
- Togaviruses: FindingsDocument4 pagesTogaviruses: Findingsحسين محمد مطرود كاظمNo ratings yet
- HIV/AIDS: The Human Immunodeficiency Virus and Acquired ImmunoDeficiency SyndromeDocument53 pagesHIV/AIDS: The Human Immunodeficiency Virus and Acquired ImmunoDeficiency SyndromeCristian RusuNo ratings yet
- HivDocument29 pagesHivSUTHAN100% (2)
- 3 - Vaccine Composition and Role of Adjuvants - Isabel Leroux-RoelsDocument50 pages3 - Vaccine Composition and Role of Adjuvants - Isabel Leroux-RoelsqNo ratings yet
- Download Handbook Of Epigenetics The New Molecular And Medical Genetics 3Rd Edition Trygve O Tollefsbol full chapterDocument67 pagesDownload Handbook Of Epigenetics The New Molecular And Medical Genetics 3Rd Edition Trygve O Tollefsbol full chapterdarrell.sesler392100% (1)
- Terapia Vih SidaDocument15 pagesTerapia Vih SidaEmmanuel Zótico Orellana JiménezNo ratings yet
- Our Last Microbiology SheetDocument12 pagesOur Last Microbiology SheetosaidistyleNo ratings yet
- Lec 6Document32 pagesLec 6Ghadi AbdalazizNo ratings yet
- COVID-19: the roles of vaccine and treatment developmentDocument27 pagesCOVID-19: the roles of vaccine and treatment developmentEndru AngelNo ratings yet
- Full download book Handbook Of Epigenetics The New Molecular And Medical Genetics Pdf pdfDocument41 pagesFull download book Handbook Of Epigenetics The New Molecular And Medical Genetics Pdf pdfjoe.vela382100% (19)
- TB Global 2Document297 pagesTB Global 2fackswellNo ratings yet
- HIV/AIDS: Biology and Treatment: Learning ObjectivesDocument10 pagesHIV/AIDS: Biology and Treatment: Learning Objectiveschrispine ochiengNo ratings yet
- Chapter 3 Virus Life CycleDocument15 pagesChapter 3 Virus Life CycleBernardo Ba HerNo ratings yet
- Nonviral Vectors for Gene TherapyFrom EverandNonviral Vectors for Gene TherapyMien-Chie HungNo ratings yet
- Interferon Gamma Release Assays Plourde SlidesDocument18 pagesInterferon Gamma Release Assays Plourde SlidesMoch Abdul RokimNo ratings yet
- NCM 16: Medical Surgical Nursing: Maricar Adelan BSN IiiaDocument3 pagesNCM 16: Medical Surgical Nursing: Maricar Adelan BSN Iiiakrizzia raymundoNo ratings yet
- Northwestern University College of Health Sciences Department of Nursing Laoag CityDocument12 pagesNorthwestern University College of Health Sciences Department of Nursing Laoag CitycchariekotNo ratings yet
- Papers FinalDocument24 pagesPapers FinalAldous Pax ArcangelNo ratings yet
- 1628172537BS-Curriculum-GEB 2019-2020 OnwordDocument113 pages1628172537BS-Curriculum-GEB 2019-2020 OnwordLuminous AudioBooksNo ratings yet
- CatalogueDocument23 pagesCatalogueAravinth ArumugamNo ratings yet
- Infectious Disease Epidemiology1Document67 pagesInfectious Disease Epidemiology1Anusha VergheseNo ratings yet
- (1980) Approved Lists of Bacterial NamesDocument196 pages(1980) Approved Lists of Bacterial NamesLeonardo LopesNo ratings yet
- Read The Passage Given Below and Write The Option That You Consider The Most Appropriate in Your Answer Sheet: (5 Marks)Document3 pagesRead The Passage Given Below and Write The Option That You Consider The Most Appropriate in Your Answer Sheet: (5 Marks)SuparnaNo ratings yet
- Case Presentation On GastroenteritisDocument17 pagesCase Presentation On GastroenteritisSafoora RafeeqNo ratings yet
- Apha 2012Document1 pageApha 2012ririn677No ratings yet
- Surgery SyllabusDocument23 pagesSurgery SyllabusNajmul Hassan MubarakNo ratings yet
- Air Microbiology 2009Document13 pagesAir Microbiology 2009Dr. SHIVA AITHAL100% (9)
- Surgical Prophylaxis and Antibiotic Selection Guide /TITLEDocument37 pagesSurgical Prophylaxis and Antibiotic Selection Guide /TITLEAbanoub Nabil100% (1)
- 2019 AUG 7 Phe Epidemiological Update MeaslesDocument10 pages2019 AUG 7 Phe Epidemiological Update MeaslesJENIFFER NATALY ALVAREZ GALINDONo ratings yet
- N11 Chan Chloe Micropara 103 Compilation of Microbial Diseases Final RequirementDocument46 pagesN11 Chan Chloe Micropara 103 Compilation of Microbial Diseases Final RequirementCHLOE CATHERINE CHANNo ratings yet
- 2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthDocument11 pages2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthCARLOTA DIAZ AGUILARNo ratings yet
- Jurnal Pencegahan KecacinganDocument5 pagesJurnal Pencegahan KecacinganBinterBarapadangNo ratings yet
- HandDocument5 pagesHandKabang MoaNo ratings yet
- Pneumonia: Meningococcal Pneumonia: A ReviewDocument13 pagesPneumonia: Meningococcal Pneumonia: A ReviewRizki Handayani SiregarNo ratings yet
- File Jurnal Infeksi NosokomialDocument12 pagesFile Jurnal Infeksi Nosokomialirmayani channelNo ratings yet
- Grand Case Presentation PrepDocument2 pagesGrand Case Presentation PrepYessamae JinangNo ratings yet
- Plasmodium. Leishmania, TripanosomaDocument48 pagesPlasmodium. Leishmania, TripanosomaStefan SaerangNo ratings yet
- Case Study: The Origins and Evolution of HIVDocument15 pagesCase Study: The Origins and Evolution of HIVBruno CasimiroNo ratings yet
- Medical Certificate ExampleDocument1 pageMedical Certificate ExampleMOHAMMAD NAZMUL ISLAMNo ratings yet
- Biological StandardizationDocument11 pagesBiological StandardizationJames UgbesNo ratings yet
- SEd 323 Lesson 1 - Introduction To Microbiology and ParasitologyDocument18 pagesSEd 323 Lesson 1 - Introduction To Microbiology and ParasitologySheilla Mae MacalaladNo ratings yet