You might also like
- Transportation Infrastructure and Cargo Logistics Master Plan For The Interoceanic Zone of The Panama Canal (PMZIC)Document38 pagesTransportation Infrastructure and Cargo Logistics Master Plan For The Interoceanic Zone of The Panama Canal (PMZIC)Pakkus ChNo ratings yet
- Cancer PrehabitationDocument13 pagesCancer PrehabitationAna Carolina Soares EstevesNo ratings yet
- Navigating and Communicating About Serious Illness and End of LifeDocument7 pagesNavigating and Communicating About Serious Illness and End of LifeMatheus RibeiroNo ratings yet
- Cancer Rehabilitation AssessmentDocument21 pagesCancer Rehabilitation AssessmentLiliana Carolina Guzman RiosNo ratings yet
- Mindfulness and Expressive Arts Therapies in Cancer CareDocument27 pagesMindfulness and Expressive Arts Therapies in Cancer Caremchirayath23No ratings yet
- Analysis: Palliative Care From Diagnosis To DeathDocument5 pagesAnalysis: Palliative Care From Diagnosis To DeathFernanda FerreiraNo ratings yet
- 2 PBDocument19 pages2 PBPralhad TalavanekarNo ratings yet
- Katz M, 2015 HahhaDocument2 pagesKatz M, 2015 HahhaRebecca DiasNo ratings yet
- Patient Centric Oral Dosage Form.Document13 pagesPatient Centric Oral Dosage Form.Snehal Suresh100% (1)
- Abeni Et Al-2014-Cancer MedicineDocument10 pagesAbeni Et Al-2014-Cancer MedicineVICTOR AUGUSTO SANTILLAN GARCÍA BLÁSQUEZNo ratings yet
- CNCR 29939Document9 pagesCNCR 29939alvarooNo ratings yet
- HHS Public AccessDocument14 pagesHHS Public AccessIsabella SánchezNo ratings yet
- The Role of Rehabilitation in Cancer Treatment: Internet Journal of Allied Health Sciences and PracticeDocument9 pagesThe Role of Rehabilitation in Cancer Treatment: Internet Journal of Allied Health Sciences and PracticeMarden OcatNo ratings yet
- Curroncol 29 00551 PDFDocument9 pagesCurroncol 29 00551 PDFMAYERLY NOVOA LEURONo ratings yet
- 21.policy Palliative CareDocument3 pages21.policy Palliative CareCaio CandidoNo ratings yet
- Cancer - 1 October 1994 - Given - The Impact of Age Treatment and Symptoms On The Physical and Mental Health of CancerDocument11 pagesCancer - 1 October 1994 - Given - The Impact of Age Treatment and Symptoms On The Physical and Mental Health of Cancervyhnl.psyNo ratings yet
- Cancer Survivorship Research State of Knowledge Challenges and OpportunitiesDocument17 pagesCancer Survivorship Research State of Knowledge Challenges and OpportunitiesM_LXNo ratings yet
- Lash Brook 2017Document17 pagesLash Brook 2017EvertonResendeNo ratings yet
- Determinants of Caregiving Experiences and MentalDocument12 pagesDeterminants of Caregiving Experiences and MentalanasenNo ratings yet
- Case Report Dewi Rahmita SariDocument10 pagesCase Report Dewi Rahmita SaridewilalalaNo ratings yet
- J Ijgo 2015 06 015Document3 pagesJ Ijgo 2015 06 015Remona RemoraNo ratings yet
- Embedded Palliative Care For Patients With Metastatic Colorectal Cancer: A Mixed-Methods Pilot StudyDocument17 pagesEmbedded Palliative Care For Patients With Metastatic Colorectal Cancer: A Mixed-Methods Pilot StudyAnatha ChrisciliaNo ratings yet
- Effect of Acceptance and Commitment Group Therapy On Quality of Life and Resilience of Women With Breast CancerDocument7 pagesEffect of Acceptance and Commitment Group Therapy On Quality of Life and Resilience of Women With Breast CancerCláudia SilvaNo ratings yet
- Older Patients' and Their Caregivers' Understanding of Advanced Care PlanningDocument5 pagesOlder Patients' and Their Caregivers' Understanding of Advanced Care PlanningGretell HenriquezNo ratings yet
- Withholding & Withdrawing Life-Sustaining TreatmentDocument11 pagesWithholding & Withdrawing Life-Sustaining TreatmentDr. Liza Manalo100% (1)
- Cancer Treatment Reviews: General and Supportive CareDocument14 pagesCancer Treatment Reviews: General and Supportive CareLoyd TuvillaNo ratings yet
- Caregiver Experience During Advanced Chronic Illness and Last Year of LifeDocument9 pagesCaregiver Experience During Advanced Chronic Illness and Last Year of LifeSiti lestarinurhamidahNo ratings yet
- Local Theories Abaquin and LaurenteDocument27 pagesLocal Theories Abaquin and LaurenteGlebin ArguezaNo ratings yet
- Clinical Preventive Medicine 2Document10 pagesClinical Preventive Medicine 2hydra89No ratings yet
- Improving Health Outcomes Through Patient Education and Partnerships With PatientsDocument3 pagesImproving Health Outcomes Through Patient Education and Partnerships With Patientsmanishms1No ratings yet
- RHB en Cancer, GeneralidadesDocument12 pagesRHB en Cancer, GeneralidadesDaniela Fernanda Cruz GómezNo ratings yet
- Fitch 2020Document7 pagesFitch 2020salvatore.sara323No ratings yet
- Living With Incurable Cancer What Are The Rehabilitation Needs in A Palliative SettingDocument10 pagesLiving With Incurable Cancer What Are The Rehabilitation Needs in A Palliative SettingLiyun ChenNo ratings yet
- 2012 - Shared Decision Making - The Pinnacle of Patient-Centered CareDocument2 pages2012 - Shared Decision Making - The Pinnacle of Patient-Centered CareDaniel MeloNo ratings yet
- Diabetes MellitusDocument5 pagesDiabetes MellitusniyaNo ratings yet
- La Dieta Mediterranea (Psycologia y Ntrucion) PDFDocument15 pagesLa Dieta Mediterranea (Psycologia y Ntrucion) PDFAle De La FuenteNo ratings yet
- Care of Clients With Acute and Chronic Health ProblemsDocument5 pagesCare of Clients With Acute and Chronic Health ProblemsJhevey ValdezNo ratings yet
- Funda LecDocument8 pagesFunda LecKimberly Anne Capiral NunogNo ratings yet
- ArikDocument14 pagesArikArditya Romy Stay CoolNo ratings yet
- The Effect of Progressive Muscle Relaxation On Cancer Patients' Self-EfficacyDocument8 pagesThe Effect of Progressive Muscle Relaxation On Cancer Patients' Self-EfficacySyahri FaziraNo ratings yet
- Relapse Prevention BasicDocument12 pagesRelapse Prevention BasicNigil ManojNo ratings yet
- 1 PBDocument7 pages1 PBdiana ElenaNo ratings yet
- MJZ 37 n0 1 PDFDocument6 pagesMJZ 37 n0 1 PDFNurul ShahirahNo ratings yet
- (R) PainDocument7 pages(R) PainVera El Sammah SiagianNo ratings yet
- 1609 FullDocument7 pages1609 FullElvi KurniaNo ratings yet
- PENADocument5 pagesPENACepti CkaleeNo ratings yet
- Alfano Recovery in CancerDocument12 pagesAlfano Recovery in CancerMircea AndreiNo ratings yet
- 2019 Sheng BrCa Survivorship Care Beyond TherapyDocument7 pages2019 Sheng BrCa Survivorship Care Beyond TherapyAngélica Fernández PérezNo ratings yet
- Oral Oncology: Hoda Badr, Vishal Gupta, Andrew Sikora, Marshall PosnerDocument7 pagesOral Oncology: Hoda Badr, Vishal Gupta, Andrew Sikora, Marshall PosnerpadillaNo ratings yet
- Quality of Life in Palliative Care Cancer Patients A Literature ReviewDocument4 pagesQuality of Life in Palliative Care Cancer Patients A Literature Reviewgw155nahNo ratings yet
- Influence of Physician Communication On Newly Diagnosed Breast Patients' Psychologic Adjustment and Decision MakingDocument6 pagesInfluence of Physician Communication On Newly Diagnosed Breast Patients' Psychologic Adjustment and Decision MakingAnonymous YdFUaW6fBNo ratings yet
- tmp27B4 TMPDocument6 pagestmp27B4 TMPFrontiersNo ratings yet
- End of Life Care Simulation A Review of The LiteratureDocument7 pagesEnd of Life Care Simulation A Review of The LiteratureafmabzmoniomdcNo ratings yet
- Chapter 1 - The Nature and Content of General Practice: DefinitionsDocument9 pagesChapter 1 - The Nature and Content of General Practice: Definitionsprofarmah6150No ratings yet
- Cancer Pain Management Program: Patients' Experiences - A Qualitative StudyDocument12 pagesCancer Pain Management Program: Patients' Experiences - A Qualitative StudyKEANNA ZURRIAGANo ratings yet
- Pursuing Minimally Disruptive Medicine: Disruption From Illness and Health Care-Related Demands Is Correlated With Patient CapacityDocument10 pagesPursuing Minimally Disruptive Medicine: Disruption From Illness and Health Care-Related Demands Is Correlated With Patient CapacityDewi KusumastutiNo ratings yet
- Jadp 07 339Document4 pagesJadp 07 339Marden OcatNo ratings yet
- JCM 10 04900Document14 pagesJCM 10 04900Chistian LassoNo ratings yet
- Team-Based Oncology Care: The Pivotal Role of Oncology NavigationFrom EverandTeam-Based Oncology Care: The Pivotal Role of Oncology NavigationLillie D. ShockneyNo ratings yet
- DuaDocument10 pagesDuaAyesha Khan100% (1)
- Differences Between Opinion, Persuasive, and Argument WritingDocument1 pageDifferences Between Opinion, Persuasive, and Argument WritingCláudiaSilvaNo ratings yet
- Creatinine Determined by "High-Performance" Liquid ChromatographyDocument4 pagesCreatinine Determined by "High-Performance" Liquid ChromatographyKaren A Ortega NNo ratings yet
- What Fiqh English Part 1Document20 pagesWhat Fiqh English Part 1Actress VeriyanNo ratings yet
- Bangladesh Earthquake SocietyDocument1 pageBangladesh Earthquake Societyapi-3711437No ratings yet
- HA Human Engineering Philosophy 2021 Sem2Document1 pageHA Human Engineering Philosophy 2021 Sem2Shubham bangarNo ratings yet
- Art of Indus ValleyDocument10 pagesArt of Indus ValleyThejasvi AtmadasaNo ratings yet
- HTW 1 3 1nDocument241 pagesHTW 1 3 1nmingo622No ratings yet
- Philippine Art History TimelineDocument1 pagePhilippine Art History TimelineTricia KimNo ratings yet
- 3.fungal Corneal UlcerDocument33 pages3.fungal Corneal Ulcersajjad hossainNo ratings yet
- Why Is Academic Research ImportantDocument5 pagesWhy Is Academic Research ImportantEli EzraNo ratings yet
- Abg AnalysisDocument3 pagesAbg AnalysisRam PattnaikNo ratings yet
- Notes On MetamodernismDocument15 pagesNotes On MetamodernismRodrigo AlcocerNo ratings yet
- In The High Court of Judicature at Hyderabad For The State of TelanganaDocument9 pagesIn The High Court of Judicature at Hyderabad For The State of Telanganayogeetha saiNo ratings yet
- Chapter 6 PDFDocument26 pagesChapter 6 PDFSITINo ratings yet
- Part I, II, III & AppendicesDocument84 pagesPart I, II, III & AppendicesLemuel Adriel TolentinoNo ratings yet
- General Anesthesia: Presented By: Shalakha Bhardwaj BDS Final Year (2007-2011)Document85 pagesGeneral Anesthesia: Presented By: Shalakha Bhardwaj BDS Final Year (2007-2011)KrishnaBihariShuklaNo ratings yet
- Interview Me Interactive Version Student A...Document1 pageInterview Me Interactive Version Student A...Heidy Forero0% (1)
- Halaman Pengesahan: Sebagai Implementasi Etika Bisnis Dalam Perusahaan Multi Level Marketing (MLM)Document16 pagesHalaman Pengesahan: Sebagai Implementasi Etika Bisnis Dalam Perusahaan Multi Level Marketing (MLM)Intan BerlianNo ratings yet
- Name of Branch Manager SBL CodeDocument20 pagesName of Branch Manager SBL CodeMohammad Zahidul AlamNo ratings yet
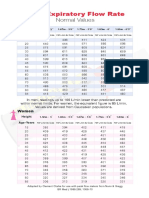
- Peak Flow Rate Chart PDFDocument2 pagesPeak Flow Rate Chart PDFlyn g100% (1)
- The Complex PlaneDocument22 pagesThe Complex PlaneAnurag KasaudhanNo ratings yet
- Socialist Strategy: Presentation by Sonny Melencio, Partido Lakas NG Masa (PLM) PhilippinesDocument20 pagesSocialist Strategy: Presentation by Sonny Melencio, Partido Lakas NG Masa (PLM) Philippinesreihana_mohideenNo ratings yet
- Gauge Theory: José Figueroa-O'FarrillDocument37 pagesGauge Theory: José Figueroa-O'Farrillcifarha venantNo ratings yet
- 1 To 12 Calndar 2023-24 Sunita MamDocument17 pages1 To 12 Calndar 2023-24 Sunita MamPoonm ChoudharyNo ratings yet
- How To Answer Bi Paper 1 and Paper 2 Wisely and Effectively by PDocument21 pagesHow To Answer Bi Paper 1 and Paper 2 Wisely and Effectively by PNorlida Abd RahmanNo ratings yet
- Dementia Agitation PathwayDocument3 pagesDementia Agitation Pathwaytatih_meilaniNo ratings yet
- HPFEM MOOC - Module FEM in Science and Society: Reference TextDocument9 pagesHPFEM MOOC - Module FEM in Science and Society: Reference TextYuryNo ratings yet
- The Poetry of Shah Isma Il IDocument49 pagesThe Poetry of Shah Isma Il IFelix De Haas100% (1)