Professional Documents
Culture Documents
Norridge 2015
Norridge 2015
Uploaded by
Kevin Bazán TorrealvaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Norridge 2015
Norridge 2015
Uploaded by
Kevin Bazán TorrealvaCopyright:
Available Formats
RESEARCH
doi: 10.1111/nicc.12160
The impact PICU nursing expertise
has on a child’s unplanned
extubation
Matthew Norridge and Alison E While
ABSTRACT
Aim: The study aimed to examine the impact of PICU nursing expertise on the unplanned extubations of children.
Background: Unplanned extubations in PICU are used as a measure of quality in clinical governance strategies. While many factors, such
as sedation or unit activity, impact negatively on unplanned extubations, high nurse-patient ratios reduce adverse patient events and improve
patient safety. However, optimal nurse-patient ratios and the impact of the level of nursing expertise on the quality of care are unknown.
Design: Audit and analysis of existing adverse event patient and nurse workforce data.
Method: This single-centre study examined unplanned extubations at a mixed general and cardiac tertiary PICU in the UK. Routinely collected
data from nursing and adverse incident databases were examined. The dataset included over 74,477 nurse allocations between August 2006
and April 2011. Unplanned extubations were the adverse event of interest.
Results: A total of 78 unplanned extubations occurred between April 2006 and April 2011. The majority of unplanned extubations occurred
when patients were looked after by junior nurses. The seniority of the nurse in-charge and the qualifications of the patient’s nurse were not
related to unplanned extubations. However, more unplanned extubations occurred at times of higher patient occupancy.
Conclusions: Nursing expertise and nurse-patient ratios were not related to unplanned extubations in this study. Further research is needed
to explore the non-workforce factors such as the securing of endotracheal tubes, sedation levels and unit activity and their relationship with
adverse events.
Relevance to Clinical Practice: In paediatric intensive care units where nurse-patient ratios are high, further investigation is needed to
establish what impact non-workforce factors have on unplanned extubations.
Key words: Adverse events • Nursing workforce • PICU • Unplanned extubation
BACKGROUND FOR THE STUDY have been more recently endorsed by the Paediatric
A Bridge to the Future [Department of Health (DH) Intensive Care Society (PICS) Standards (2010) and
1997a) made the first recommendations relating to Royal College of Nursing (RCN) (2013). In paediatrics,
the qualifications and experience of nurses on pae- much of the literature investigating patient safety in
diatric intensive care units (PICU) and caring for PICU has focused on the factors related to unplanned
patients of varying acuity as defined in the Framework extubations, as this is seen as a marker of care quality
for the Future (DH 1997b). These recommendations (Penuelas et al., 2011). While there is no current bench-
mark, unplanned extubations are monitored as a part
of clinical governance and by commissioners of PICU
Authors: M. Norridge, BSc, MSc, RN (Child): TCH Lecturer Practitioner,
services (NHS Commissioning Board 2013).
King’s College London, Florence Nightingale Faculty of Nursing and
Midwifery, London, UK and Evelina London Children’s Hospital, Guy’s & There are a number of factors which potentially
Thomas’ NHS Foundation Trust, London, UK; A.E. While, BSc, MSc, PhD, underpin unplanned extubations such as medical
RN, RHV: Professor of Community Nursing, King’s College London, staffing, unit activity, sedation levels and nursing
Florence Nightingale Faculty of Nursing and Midwifery, London, UK workforce factors. Therefore understanding the factors
Address for correspondence: M. Norridge, King’s College London,
influencing unplanned extubations in the PICU at the
Florence Nightingale Faculty of Nursing and Midwifery, 57 Waterloo Road,
London SE1 8WA, UK
unit level may enable quality improvement initiatives
E-mail matthew.norridge@kcl.ac.uk and decrease the occurrence of this adverse event and
ensure patient safety (Rachman et al., 2009).
© 2015 British Association of Critical Care Nurses 1
The impact PICU nursing expertise has on a child’s unplanned extubation
LITERATURE REVIEW Many conclusions from adult ICU studies indi-
A literature search was performed to understand cate improved patient outcomes with an increase
adverse events in the intensive care setting and in nursing workforce. However, of the four studies
their relationships with nursing workforce factors. exploring aspects of the nursing workforce in the
Studies were included from adult ICU settings as paediatric setting, only one reported upon the rela-
well as PICUs as there is a dearth of current liter- tionship with patient outcomes with the remaining
ature that specifically examines these issues in UK three studies investigating aspects of patient safety.
PICUs. Studies were identified that considered the Notably, none of the studies investigated the role of
impact of nursing workforce factors on many adverse nurse training/education upon patient outcomes.
events (Tibby et al., 2004) including: patient outcomes Tibby et al.’s (2004) study examined nursing work-
(Amaravadi et al., 2000), length of stay (Pronovost et al., load, skill mix and staff support in relation to adverse
1999), mortality (Tarnow-Mordi et al., 2000; Pronovost incidents in PICU. They reported an increase in adverse
et al., 2001), respiratory complications (Dang et al., events during day shifts compared to night shifts due
2002), health care-associated infections (HCAIs) to increased activity during day shifts. They noted
(Hugonnet et al., 2007) and unplanned extubations that more rostered permanent staff was associated
(Marcin et al., 2005; Ream et al., 2007). Unplanned extu- with a decrease of adverse events. Tibby et al. (2004)
bations were chosen as they are considered quality also found a reduction in adverse incidents when a
markers in both adult and paediatric ICUs. senior nurse (Clinical G Grade) was in-charge. They
Six studies in the adult ICU setting examined suggested that the nursing staff composition was an
the relationship between nurse-patient ratios and important factor, both in terms of the nurse seniority
patient outcomes (Pronovost et al., 1999; Amaravadi and the proportion of permanent staff on duty.
et al., 2000; Tarnow-Mordi et al., 2000; Pronovost et al., Marcin et al.’s (2005) retrospective case-control study
2001; Dang et al., 2002, Hugonnet et al., 2007). A large found a significant relationship between patient agita-
American study examined the impact of nurse-patient tion levels and unplanned extubations (p < 0.01). How-
ratios upon post-cardiotomy patient outcomes with the ever, other factors that may impact on this, such as
ratio of 1:2 emerging as the optimum ratio (Pronovost methods used to secure the endotracheal tube (ETT)
et al., 1999). This study reported a significant reduction and types of restraints used to reduce activity in the
in ICU length of stay with higher nurse-patient ratios agitated patient, were not considered in this study.
(p < 0.05) (Pronovost et al., 1999). Another American They found no relationship between the nurses’ years
study concurred with these findings (Amaravadi et al., of experience and unplanned extubation rates but
2000) and found that lower nurse-patient ratios were they reported a positive relationship between high
associated with significantly higher costs (p < 0.001) nurse-patient ratios and reduced unplanned extuba-
due to a significant increase in length of stay (p < 0.001) tions.
and more complications. These findings suggest that Unplanned extubations were also investigated by
investment in the nursing workforce may reduce Ream et al. (2007). Using logistic regression modelling,
overall expenditure by reducing length of stay and this single-centre cohort study found a positive asso-
avoidable costs. ciation between unplanned extubations and nursing
A small single-centre observational Scottish study ratios (p = 0.03). This study found increasing numbers
found that an increased workload resulted in a sig- of unplanned extubations with nurse-patient ratios of
nificant increase in mortality (p < 0.05) (Tarnow-Mordi 1:2 as compared with 1:1.
et al., 2000). Conversely, Pronovost et al. (2001) strug- Using secondary data Hickey et al. (2010) investi-
gled to demonstrate a causal link between mortality gated the relationship between nursing staff, skill mix
and nurse-patient ratios; however, they reported a and Magnet hospital recognition. They found no rela-
significant relationship between increased respira- tionships between mortality rates and nursing staff fac-
tory complications and lower nurse-patient ratios tors including skill mix, and it is unclear on what basis
(p < 0.001). Similarly Dang et al. (2002) reported that they asserted the merits of Magnet hospitals and higher
a lower nurse-patient ratio resulted in increased nurse qualification ratios.
respiratory complications. A large Swiss study The influence of nursing staff factors upon patient
has also reported a 30% reduction in health care outcomes in the intensive care setting has attracted
associated infections with increased staff num- limited research. Yet the professional societies of
bers (Hugonnet et al., 2007). This study estimated adult and paediatric intensive care recommend a 1:1
that 26.7% of all infections could be avoided if the nurse-patient ratio for ventilated patients, suggesting
nurse-patient ratio was maintained at greater than the importance of nursing care including the avoidance
1:2. of adverse events such as unplanned extubation.
2 © 2015 British Association of Critical Care Nurses
The impact PICU nursing expertise has on a child’s unplanned extubation
While the importance of nurse-patient ratios was further training and complete a competency document
highlighted in the studies, none of the studies offered a assessing their ability to take charge of the PICU dur-
definitive ratio to improve patient outcomes. Only one ing a shift. This progression is specific to the study
study suggested that a ratio of 1:2 was preferable to 1:3 PICU and may differ from other PICUs in the UK.
(Amaravadi et al., 2000) which would clearly have cost The study PICU provides a regional, integrated
implications. Without robust evidence implementing PICU retrieval service with one to two specially
increases in nurse-patient ratios may be difficult in the trained retrieval nurses allocated within the nurs-
current fiscal climate with the emphasis upon provid- ing numbers on each shift. Other unit characteristics
ing optimal patient outcomes and patient safety within that may impact upon the service provision and
existing resources (Tibby et al., 2004). Thus there is a nursing workload include a health care assistant
need for more evidence of the impact of nursing work- on each shift, whose role is primarily focussed on
force factors upon care quality. house-keeping and little patient contact. There is
also a dedicated PICU Play Specialist available for
7.5 hours, Monday to Friday. Additionally a pharmacy
METHODS centralized intravenous additive service (CIVAS) pro-
Aim vides pre-ordered antibiotics, morphine and milrinone
The study aimed to examine the impact of nursing infusions.
expertise and shifts on unplanned extubations as a
quality marker within one PICU.
Data Collection methods
The study PICU has a nurse allocation database com-
Study Site pleted on each shift by the nurse in-charge which
This single-centre study examined unplanned extuba- includes nurse allocations to roles/patients, patient
tions on a 20-bedded tertiary PICU in the UK which acuity and dependency levels, admissions, discharges
is currently funded for 18 beds. For this study an and ward events. This database was accessed ret-
unplanned extubation was defined as an extuba- rospectively in January 2012 to collect data relating
tion where the ETT was displaced or removed from to nurse allocations to role (including shift nurse
the trachea by either the patient (self-extubation) in-charge) and patients on each shift (n = 74,477).
or by medical personnel at a time outside the plan Patient and unplanned extubation data were collected
of care. for the period April 2006 to April 2011 from the hos-
The study PICU provides care for children requiring pital databases. Nurse workforce data included shift
various general and cardiac critical care needs, for type, start time, end time, nurse clinical grade (band),
example, respiratory failure and post-cardiotomy. The nurse qualification, rostered staff or agency, alloca-
nurses work twelve-and-half-hour shifts (day and tion type (i.e. patient or role). Anonymized patient
night shifts) and rotate between these shifts through- data included: patient acuity and patient depen-
out the month. On joining the PICU, a new nurse dency. Unplanned extubation data were obtained
undertakes a 6-month, mandatory in-house orienta- in January 2012 from the PICU adverse incident
tion programme as an introduction to the foundational database which is a self-reporting system of patient
aspects of nursing care specific to PICU. Six weeks of incidents.
supervised practice with an associated competency
document guides their development with all new
nurses required to complete core competencies prior Data Analysis
to practising independently, such as safe airway man- The data were analysed using IBM SPSS Statistics
agement. Anecdotal evidence suggests that nurses 21. The Pearson’s chi-square test was used to explore
commence a nationally recognised PICU qualification whether there was a relationship between two cat-
after approximately 12–18 months’ experience in egorical variables (Field, 2009). The data were not
PICU. Courses leading to the PICU qualification, as set normally distributed and therefore the appropriate
out in the PICS Standards (PICS 2010), are delivered non-parametric statistical test was selected.
by local universities. Additionally the study PICU
offers ongoing clinical education and support with a Validity and Reliability
dedicated nurse education team. This study utilized retrospective organizational data.
On gaining the PICU qualification, the nurses at The allocation data were scrutinized for accuracy, but
the study PICU will typically apply for promotion its accuracy depended upon the correct documentation
to Senior Staff Nurse (Clinical Band 6). Two years of individual roles by the shift in-charge nurse at the
following promotion to Band 6, the nurses undertake time of data input.
© 2015 British Association of Critical Care Nurses 3
The impact PICU nursing expertise has on a child’s unplanned extubation
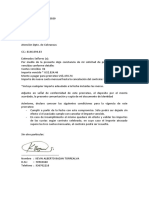
Figure 1 The number of unplanned extubations by shift type and day of the week.
Ethical Considerations (Clinical Band 5) (accounting for 47% of nursing work-
Permission for the study as a service evaluation was force), the clinical grade of the patient’s nurse was not
granted through the NHS Trust’s Research and Devel- significant (p = 0.46) (Table 2). Four more unplanned
opment Department. All the study data were routinely extubations occurred when the patients were being
collected so that no ethical approval was required. cared for by nurses holding a PICU qualification
All nurse and patient details analyzed were fully (Table 2) (n = 41) although this was not statistically
anonymized. significant (p = 0.44).
Examination of nurse-patient ratios showed that
most extubations occurred when there was a ratio of
1:1 (n = 70) with only a 1:2 ratio occurring on 10% of
RESULTS
the shifts. The clinical grade of the shift nurse in-charge
During the period April 2006 to April 2011 there
was not related to unplanned extubations (p = 0.59)
were 78 unplanned extubations recorded in the study
(Table 3).
PICU, 42 during day shifts and 36 during night shifts
(Figure 1). An examination of unplanned extubations
by day of the week showed that most (n = 20) occurred
on Mondays. On Tuesdays, Fridays and Saturdays 12 DISCUSSION
extubations occurred with Sundays having the least The Impact of Day Shifts and Night Shifts
(n = 8). This study found no significant difference in the
A notably higher number of unplanned extubations number of unplanned extubations between the day
occurred during 2010 compared to any other year and night shifts in contrast to Hamilton et al.’s (2007)
(Table 1) which was also the year with the highest bed reported increase in adverse patient events at night
occupancy. The winter months had the highest number and weekends. However, a direct comparison of the
of unplanned extubations at the same time as there was findings may not be helpful as the practice environ-
high bed occupancy. The months of April and Septem- ment and demographics of each area vary. In Hamilton
ber had a high number of unplanned extubations, yet et al.’s (2007) review, many of the studies were from
the bed occupancy in both months was lower than in the USA which has distinct teams for unsocial and
the other months. social shifts respectively with more senior nurses
Although most extubations occurred when the working less unsocial shifts, thus creating an envi-
patient was being looked after by a junior staff nurse ronment where experienced nurses work day shifts
4 © 2015 British Association of Critical Care Nurses
The impact PICU nursing expertise has on a child’s unplanned extubation
Table 1 Average patient occupancy and unplanned extubations by month In the study PICU much effort is directed at nor-
and year malizing the children’s activities where possible so
that during a day shift there is an increase in the
Year: 2006 2007 2008 2009 2010 2011 Total number of visitors and interventions to stimulate the
patient which in turn may increase the chance of
January Patients 730 704 747 916 839 3936
the ETT becoming dislodged. In contrast, during a
UPE 0 1 2 4 3 10
night shift, where the patient’s condition allows, light-
February Patients 652 494 633 841 760 3380
ing is significantly lower and both the patient and
UPE 2 0 0 1 1 4
March Patients 695 556 773 852 857 3733
unit activities are reduced to assist the children to
UPE 1 1 1 1 1 5 maintain near normal day/night sleeping and activity
April Patients 497 625 688 728 694 75 3307 patterns.
UPE 3 1 2 0 3 0 9
May Patients 464 675 739 622 889 3389 Variability in Unplanned Extubations and the
UPE 0 0 1 0 3 4 Day of the Week
June Patients 465 677 651 612 635 3040
There were no differences between the days of the week
UPE 1 1 1 1 0 4
and the number of unplanned extubations, albeit a
July Patients 528 757 769 548 834 3436
slight increase occurred on Mondays which contrasts
UPE 1 2 0 2 1 6
with an increase in the number of adverse events at the
August Patients 491 641 673 607 660 3072
weekend reported elsewhere (Hamilton et al., 2007). It
UPE 2 0 0 0 1 3
September Patients 554 634 662 711 814 3375 is unclear why Mondays had the highest number of
UPE 1 1 1 3 2 8 unplanned extubations as there are no activities which
October Patients 609 737 749 790 842 3727 are specific to Mondays. One factor which may account
UPE 0 0 0 6 3 9 for this variation is high staff changeover due to nurses
November Patients 724 740 789 711 785 3749 requesting to work clustered weekend shifts separately
UPE 2 1 0 0 2 5 from weekday shifts. This shift pattern is also mirrored
December Patients 735 761 777 913 891 4077 by medical staff. However, a larger dataset would be
UPE 2 5 2 2 0 11 required to determine whether the day of the week was
Total Patients 5067 8324 8251 8395 9653 2531 42221 associated with the frequency of unplanned extubation
UPE 12 14 9 17 21 5 78 events.
UPE, Unplanned Extubations.
Variability in Unplanned Extubations
and Month
and new or inexperienced staff work night shifts. In The study found that the largest number of unplanned
the study PICU there is internal rotation between day, extubations occurred between October and January
weekend and night shifts with all Clinical Band 5–7 which was unsurprising as other studies have shown
nurses working all shifts in any given month so that that increased patient workload, due to the seasonal
the experience level and skill mix is consistent. variation of the winter months, results in an increased
As in Tibby et al.’s (2004) study, an increased num- number of adverse events (Tarnow-Mordi et al., 2000;
ber of adverse events occurred during day shifts which Tucker et al., 2002; Tibby et al., 2004). There is raised
Tibby et al. concluded was the result of increased activ- activity during October to January (Table 1) due to an
ity including an increased number of multidisciplinary increased number of patients with respiratory patholo-
team members present during a day shift. When specif- gies, primarily infants with bronchiolitis, all of whom
ically focusing on unplanned extubations, there are are usually ventilated.
a number of other factors which could influence the The number of unplanned extubations that occurred
occurrence of unplanned extubations, for example, in April and September was unexpected but may
patients are more likely to be transferred for scans and reflect the new rotation of medical staff on the unit.
admitted from theatre during the day shift. Transfer- New doctors start in August and towards the end of
ring an intubated patient has the potential to disturb February. During their first few weeks on the study
the ETT position and thus the potential for unplanned PICU, they are closely supervised by the consultants as
extubation is higher. This study did not account for part of their induction prior to being given more auton-
these activities. Future research should measure activ- omy and reduced scrutiny of their practice. The April
ity levels to understand the full context of adverse and September unplanned extubations peaks coincide
events. with the independence level of the new PICU medical
© 2015 British Association of Critical Care Nurses 5
The impact PICU nursing expertise has on a child’s unplanned extubation
Table 2 Allocations to ventilated patients and extubations by nurse seniority and PICU qualification
2006-11 Patient Allocations
No Unplanned Unplanned Total Patient
Extubations Extubations Allocation
PICU
Nurse Seniority Qualification n n % n %
Junior Staff Nurse∗ No Count 30083 37 47% 30120 55%
Expected Count 30077.0 43.0 30120
Senior Staff Nurse† Yes Count 4978 11 14% 4989 9%
Expected Count 4981.9 7.1 4989
Junior Sister‡ Yes Count 15271 25 32% 15296 28%
Expected Count 15274.2 21.8 15296
Senior Sister/ Charge Nurse§ Yes Count 4266 5 6% 4271 8%
Expected Count 4264.9 6.1 4271
Total Count 54598 78 54676
Expected Count 54598.0 78 54676
∗ Band 5 Nurses.
† Band 5 Nurses with PICU Qualification.
‡ Band 6 Nurses.
§ Band 7 Nurses.
Table 3 Comparison of the clinical grade of the shift nurse in-charge over extubation during the study period. This finding
the 5-year study period and unplanned extubations was not unexpected, as junior staff nurses are the
largest group in the qualified nursing workforce in
2006-11 Shifts In-charge Allocations the study PICU although Marcin et al. (2005) found
no relationship between nurses’ years of experience
No Unplanned Unplanned Total In-charge
and unplanned extubation rates. The junior staff nurse
Extubations Extubations Shifts
Shift In-charge role is exclusively to look after patients due to the
Nurse n n % n % limitations of their experience and lack of addi-
tional qualifications which increases their patient
Junior Sister∗ Count 1218 28 36 1246 33
exposure and therefore the likelihood of experiencing
Expected Count 1220.2 25.8 1246
an unplanned extubation. Junior staff nurses have
Senior Sister/ Count 2473 50 64 2523 67
Charge Nurse† Expected Count 2470.8 52.2 2523
less experience and as a result may not have the
Total Count 3691 78 3769 skills of anticipation and management of unexpected
Expected Count 3691.0 78.0 3769 events, as they usually operate somewhere between
the advanced beginner or competent stages of practice
∗ Band 6 Nurses.
† Band 7 Nurses.
(Benner 2001). In contrast more experienced nurses are
expected to operate on a higher level of practice and to
anticipate and prevent adverse events. This highlights
staff who may not yet be familiar with all the proto- the importance of providing education and training
cols including the securing of ETTs. This contrasts with to facilitate the development of expert knowledge and
Tibby et al. (2004) who found that the arrival of new intuition together with the importance of appropriate
medical staff was a significant factor in the reduction of airway management.
adverse events. However, their study comprised data There is currently no evidence regarding the com-
for only a 12-month period compared to the 5 years in pletion of a PICU course and its effect upon patient
this study. care and this study found no relationship between the
number of unplanned extubations and a PICU quali-
Impact of Nurses Experience and Expertise fication. Conversely, Tarnow-Mordi et al. (2000) found
The majority of patients who experienced an that inadequate training and supervision resulted in
unplanned extubation were looked after by junior staff increased patient related adverse events, although
nurses, although it is noteworthy that every clinical they did not specify the nature of the training.
grade of nurse experienced at least one unplanned This study’s findings lend support to the role of
6 © 2015 British Association of Critical Care Nurses
The impact PICU nursing expertise has on a child’s unplanned extubation
the PICU Induction Programme as preparation for comparable study which reported a decrease in
the PICU nursing care setting although firm con- adverse events when a senior nurse (equivalent Clini-
clusions cannot be drawn on the basis of this study cal Band 7) was in-charge suggesting the importance of
alone. clinical leadership. Tibby et al.’s (2004) study covered
a shorter period of time (12 months) and examined all
Impact of Nurse-Patient Ratios adverse events rather than only unplanned extuba-
This study found no association between nurse-patient tions. A larger study of all adverse events may have
ratios and unplanned extubations with 90% of the yielded different findings because a senior sister/
recorded events occurring within a 1:1 nurse-patient charge nurse is always present on each shift to provide
ratio and only 10% occurring within a 1:2 nurse-patient clinical leadership, although not necessarily as desig-
ratio. This contrasts with the literature which reported nated shift in-charge nurse. As the study period only
that a high nurse-patient ratio had a significant effect covered the time when there was a senior sister/charge
on reducing patient related adverse events (Pronovost nurse on each shift, it is difficult to draw conclusions
et al., 1999; Amaravadi et al., 2000; Tarnow-Mordi et al., about their impact upon patient outcomes although
2000; Pronovost et al., 2001; Dang et al., 2002; Marcin the NNRU (2008) has suggested that role-modelling
et al., 2005; Hugonnet et al., 2007; Ream et al., 2007; is important for the provision of quality patient care.
Profit et al., 2010; Sink et al., 2011). The study find- Further exploration of the relationship between clinical
ings may reflect the lack of adjustment for other influ- leadership and patient care outcomes is warranted.
encing factors present at the time of the incident,
namely, physiotherapy, transfer from trolley to bed,
ETT securing methods, ETT position and sedation CONCLUSION
levels. The focus of the health services is not just mainte-
At the study PICU, ventilated patients are not heav- nance of a safe and sustainable service, but on deliv-
ily sedated as it is believed to reduce the number of ery of high-quality health care efficiently. The current
ventilator days per patient. Further the study PICU challenge for health services is to provide this within
has one of the lowest number of ventilator days per limited resources for further care improvement. Fur-
patient in the UK (Paediatric Intensive Care Audit ther research is needed to explore the relationships
Network 2010). A previous study has found a rela- of non-nursing workforce factors such as ETT care
tionship between patient agitation and unplanned protocols, patient agitation and ward activities upon
extubations highlighting that, while reducing sedation unplanned extubations alongside the impact of clini-
may reduce the length of ventilation time, it may cal leadership in the form of senior nurse presence. The
potentially increase the risk of unplanned extubations study findings suggest that high nurse-patient ratios
(Marcin et al., 2005). The sedation protocol in the provide a solid foundation upon which to deliver safe,
study PICU is currently under review so that it may high quality care within PICUs.
be interesting to explore the incidence of unplanned
extubations in relation to the current and new sedation
protocols. IMPLICATIONS FOR CLINICAL PRACTICE
Transferring conclusions about nurse-patient ratios This study did not find a clear relationship between
from this study to other PICUs is difficult because the the nursing workforce factors of nurse-patient ratio
study PICU employed consistently high nurse-patient and senior nurse on site clinical leadership and
ratios. More research is needed to ascertain an appro- unplanned extubations in the study PICU. The slight
priate nurse-patient ratio and whether 1:2 ratios over a increase in unplanned extubations on Mondays
long period result in increased unplanned extubations. may have implications for shift scheduling to pre-
The current recommendations are limited and focus on vent ‘whole team’ changeover on Mondays. Greater
the number of Registered Nurses to patients (Penoyer, attention may be warranted regarding non-nursing
2010; PICS, 2010; RCN, 2013) without consideration of workforce factors, such as activities levels, patient
overall staffing levels and the skill mix within the nurs- acuity and patient numbers to reduce unplanned
ing team [National Nursing Research Unit (NNRU), extubations where PICUs have high nurse-patient
2012]. ratios.
The Impact of the Shift In-charge Nurse
ACKNOWLEDGEMENTS
A senior sister/charge nurse (Clinical Band 7) as the
We are grateful to Joanna Philip and Andrew Durward
shift in-charge nurse was not related to unplanned
for assistance with access to the databases.
extubations which contrasts with Tibby et al.’s (2004)
© 2015 British Association of Critical Care Nurses 7
The impact PICU nursing expertise has on a child’s unplanned extubation
WHAT IS KNOWN ABOUT THIS TOPIC
• The influence of nurse factors upon patient outcomes in the intensive care setting has attracted limited research.
• Professional societies of adult and paediatric intensive care recommend a 1:1 nurse-patient ratio for ventilated patients, suggesting the
importance of the nursing role in the provision of this care.
WHAT THIS PAPER ADDS
• There is no relationship between nursing workforce factors and unplanned extubations in a PICU within the context of high
nurse-patient ratios and a senior sister/charge nurse providing on-site leadership.
• In PICUs where nurse-patient ratios are high, further investigation is needed to establish what impact non-nursing workforce factors
have on unplanned extubations.
REFERENCES NHS Commissioning Board. (2013). 2013/14 HS Standard
Contract for Paediatric Intensive Care. http://www.england.nhs.
Amaravadi RK, Dimick JB, Pronovost PJ, Lipsett PA. (2000). ICU
uk/wp-content/uploads/2013/07/eo7sa-paed-inten-care.pdf
nurse-to-patient ratio is associated with complications and
(accessed 2/10/14).
resource use after esophagectomy. Intensive Care Medicine; 26:
Paediatric Intensive Care Audit Network. (2010). Annual Report of
1857–1862.
the Paediatric Intensive Care Audit Network. http://www.
Benner P. (2001). From Novice to Expert: Excellence and Power
picanet.org.uk/Documents/General/Annual%20Report%20
in Clinical Nursing Practice (Commemorative Edition). London:
2010/2010%20PICANet%20Annual%20Report.pdf (accessed
Prentice Hall Health.
13/04/11)
Dang D, Johantgen ME, Pronovost PJ, Jenckes MW, Bass EB.
Paediatric Intensive Care Society [PICS]. (2010). Standards for the
(2002). Postoperative complications: does intensive care unit
Care Critically Ill Children. 4th ed. www.ukpics.org.uk/
staff nursing make a difference? Heart & Lung; 31: 219–228.
documents/PICS_standards.pdf (accessed 15/02/11)
Department of Health. (1997a). A Bridge to the Future.
Penoyer DA. (2010). Nurse staffing and patient outcomes in criti-
http://www.dh.gov.uk/prod_consum_dh/groups/dh_
cal care: a concise review. Critical Care Medicine; 38: 1521–1528
digitalassets/@dh/@en/documents/digitalasset/dh_40143
quiz 1529.
68.pdf (accessed 13/02/11). Penuelas O, Frutos-Vivar F, Esteban A. (2011). Unplanned extuba-
Department of Health. (1997b). Paediatric Intensive Care “A Frame- tions in the ICU: a marker of quality assurance of mechanical
work for the Future”. http://www.dh.gov.uk/prod_consum_ ventilation. Critical Care; 15: 128–129.
dh/groups/dh_digitalassets/@dh/@en/documents/digital Profit J, Petersen LA, McCormick MC, Escobar GJ, Coleman-Phox
asset/dh_4034342.pdf (accessed 13/02/11). K, Zheng Z, Pietz K, Zupancic JAF. (2010). Patient-to-nurse
Field A. (2009). Discovering Statistics Using SPSS. 3rd edn. London: ratios and outcomes of moderately preterm infants. Pediatrics;
Sage. 125: 320–326.
Hamilton P, Eschiti VS, Hernandez K, Neill D. (2007). Differences Pronovost PJ, Jenckes MW, Dorman T, Garrett E, Breslow MJ,
between weekend and weekday nurse work environments Rosenfeld BA, Lipsett PA, Bass EB. (1999). Organizational
and patient outcomes: a focus group approach to model test- characteristics of intensive care units related to outcomes of
ing. The Journal of Perinatal & Neonatal Nursing; 21: 331–341. abdominal aortic surgery. JAMA; 281: 1310–1317.
Hickey P, Gauvreau K, Connor J, Sporing E, Jenkins K. (2010). The Pronovost PJ, Dang D, Dorman T, Lipsett PA, Garrett E, Jenckes
relationship of nurse staffing, skill mix, and magnet recogni- M, Bass EB. (2001). Intensive care unit nurse staffing and the
tion to institutional volume and mortality for congenital heart risk for complications after abdominal aortic surgery. Effective
surgery. Journal of Nursing Administration; 40: 226–232. Clinical Practice; 4: 199–206.
Hugonnet S, Chevrolet J, Pittet D. (2007). The effect of workload Rachman BR, Watson R, Woods N, Mink RB. (2009). Reducing
on infection risk in critically ill patients. Critical Care Medicine; unplanned extubations in a pediatric intensive care unit: a
35: 76–81. systematic approach. International Journal of Pediatrics 820495:
Marcin JP, Rutan E, Rapetti PM, Brown JP, Rahnamayi R, Pretzlaff 30.
RK. (2005). Nurse staffing and unplanned extubation in the Ream RS, Mackey K, Leet T, Green MC, Andreone TL, Loftis
pediatric intensive care unit. Pediatric Critical Care Medicine; 6: LL, Lynch RE. (2007). Association of nursing workload and
254–257. unplanned extubations in a pediatric intensive care unit. Pedi-
National Nursing Research Unit [NNRU]. (2008). High atric Critical Care Medicine; 8: 366–371.
quality nursing care – what is it and how can we Royal College of Nursing [RCN]. (2013). Defining Staffing
best ensure its delivery? Policy+;13: http://www.kcl.ac.uk/ Levels for Children and Young People’s Services. http://
content/1/c6/04/37/71/PolicyIssue13.pdf (accessed www.rcn.org.uk/__data/assets/pdf_file/0004/78592/002
13/07/11). 172.pdf. (accessed 07/04/2014).
National Nursing Research Unit [NNRU]. (2012). Is it time to Sink DW, Hope SA, Hagadorn JI. (2011). Nurse:patient ratio and
set minimum nurse staffing levels in English hospitals? achievement of oxygen saturation goals in premature infants.
Policy+;34: http://www.kcl.ac.uk/nursing/research/nnru/ Archives of Disease in Childhood. Fetal and Neonatal Edition; 96:
Policy/Currentissue/PolicyIssue34.pdf (accessed 1/04/12). F93–F98.
8 © 2015 British Association of Critical Care Nurses
The impact PICU nursing expertise has on a child’s unplanned extubation
Tarnow-Mordi WO, Hau C, Warden A, Shearer AJ. (2000). Hospi- Tucker J, UKNSS. (2002). Patient volume, staffing, and workload
tal mortality in relation to staff workload: a 4-year study in an in relation to risk-adjusted outcomes in a random stratified
adult intensive-care unit. Lancet; 356: 185–189. sample of UK neonatal intensive care units: a prospective
Tibby SM, Correa-West J, Durward A, Ferguson L, Murdoch IA. evaluation. Lancet; 359: 99–107.
(2004). Adverse events in a paediatric intensive care unit: rela-
tionship to workload, skill mix and staff supervision. Intensive
Care Medicine; 30: 1160–1166.
© 2015 British Association of Critical Care Nurses 9
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Achieving Sustainability in Reducing Unplanned Extubations in PICUDocument7 pagesAchieving Sustainability in Reducing Unplanned Extubations in PICUKevin Bazán TorrealvaNo ratings yet
- Ba 002 Sup Raanc 2022Document8 pagesBa 002 Sup Raanc 2022Kevin Bazán TorrealvaNo ratings yet
- 5 PS Maya - PediatriaDocument3 pages5 PS Maya - PediatriaKevin Bazán TorrealvaNo ratings yet
- Ba 003 Sup Ratar 2022Document8 pagesBa 003 Sup Ratar 2022Kevin Bazán TorrealvaNo ratings yet
- Lineamientos para Proceso de Reasignacion Ley N 31538Document148 pagesLineamientos para Proceso de Reasignacion Ley N 31538Kevin Bazán TorrealvaNo ratings yet
- Memorando Circular #095-Gcgp-Essalud-2021 - Actualización de Los Linemientos de Acción Ante Sospecha o Confirmación de Covid 19 en Los Trabajadores de EssaludDocument7 pagesMemorando Circular #095-Gcgp-Essalud-2021 - Actualización de Los Linemientos de Acción Ante Sospecha o Confirmación de Covid 19 en Los Trabajadores de EssaludKevin Bazán TorrealvaNo ratings yet
- Ba 001 Sup Rpreb 2022Document8 pagesBa 001 Sup Rpreb 2022Kevin Bazán TorrealvaNo ratings yet
- Escala Remunerativa 2022 PDFDocument3 pagesEscala Remunerativa 2022 PDFKevin Bazán TorrealvaNo ratings yet
- Memorando Circular #095-Gcgp-Essalud-2021 - Actualización de Los Linemientos de Acción Ante Sospecha o Confirmación de Covid 19 en Los Trabajadores de EssaludDocument7 pagesMemorando Circular #095-Gcgp-Essalud-2021 - Actualización de Los Linemientos de Acción Ante Sospecha o Confirmación de Covid 19 en Los Trabajadores de EssaludKevin Bazán TorrealvaNo ratings yet
- Entrevista Personal Via ZoomDocument3 pagesEntrevista Personal Via ZoomKevin Bazán TorrealvaNo ratings yet
- Fragilidad CapilarDocument48 pagesFragilidad CapilarKevin Bazán TorrealvaNo ratings yet
- Descargo MINSADocument1 pageDescargo MINSAKevin Bazán TorrealvaNo ratings yet
- Prorrateo OPCIONDocument1 pageProrrateo OPCIONKevin Bazán TorrealvaNo ratings yet
- Preguntas y Respuestas de Nutrición ParenteralDocument1 pagePreguntas y Respuestas de Nutrición ParenteralKevin Bazán TorrealvaNo ratings yet
- Declaracion Jurada No Haber Realizado SERUMSDocument1 pageDeclaracion Jurada No Haber Realizado SERUMSKevin Bazán TorrealvaNo ratings yet
- Plan de Estudios Del Residentado Médico en Pediatría - UNAPDocument2 pagesPlan de Estudios Del Residentado Médico en Pediatría - UNAPKevin Bazán TorrealvaNo ratings yet
- NPT PreguntasDocument4 pagesNPT PreguntasKevin Bazán TorrealvaNo ratings yet
- Lactate DehydrogenaseDocument2 pagesLactate DehydrogenaseKevin Bazán Torrealva100% (1)