You might also like
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Factors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaDocument10 pagesFactors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaInternational Journal of Current Innovations in Advanced Research100% (1)
- Prevalence of Malnutrition Among Under-Five Children in Al-Nohoud Province Western Kordufan, SudanDocument6 pagesPrevalence of Malnutrition Among Under-Five Children in Al-Nohoud Province Western Kordufan, SudanIJPHSNo ratings yet
- Prevalence of Acute Malnutrition and Associated Factors Among Under-Five Children in Gursum District, Somali Region, EthiopiaDocument7 pagesPrevalence of Acute Malnutrition and Associated Factors Among Under-Five Children in Gursum District, Somali Region, EthiopiajakeNo ratings yet
- Factors Associated With Stunting Among Children of Age 24 To 59 Months in Meskan District, Gurage Zone, South Ethiopia: A Case-Control StudyDocument7 pagesFactors Associated With Stunting Among Children of Age 24 To 59 Months in Meskan District, Gurage Zone, South Ethiopia: A Case-Control Studyfio rentiniNo ratings yet
- Agriculture in ZambiaDocument6 pagesAgriculture in ZambiaTheo CassNo ratings yet
- Stunting, Prevalence, Associated Factors, Wondo Genet, EthiopiaDocument14 pagesStunting, Prevalence, Associated Factors, Wondo Genet, EthiopiaJecko BageurNo ratings yet
- Factors That Contribute To Occurrence of Malnutrition Among Children Below Five Years in Pediatric Ward Itojo Hospital, Ntungamo District Uganda.Document14 pagesFactors That Contribute To Occurrence of Malnutrition Among Children Below Five Years in Pediatric Ward Itojo Hospital, Ntungamo District Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Agriculture in AfricaDocument6 pagesAgriculture in AfricaTheo CassNo ratings yet
- 17 Dipendra EtalDocument7 pages17 Dipendra EtaleditorijmrhsNo ratings yet
- Nutritional Status of Under-Five Children in Rural BangladeshDocument6 pagesNutritional Status of Under-Five Children in Rural BangladeshIJPHSNo ratings yet
- 107905-Article Text-294610-1-10-20140917Document26 pages107905-Article Text-294610-1-10-20140917Desi PuspitasariNo ratings yet
- Abdirauf Ahmed Isse's Individual AssignmentDocument15 pagesAbdirauf Ahmed Isse's Individual AssignmentAbdifatah Ahmed TubeNo ratings yet
- 1 PB - 2Document6 pages1 PB - 2Dereje DesalegnNo ratings yet
- Investigating Key Determinants of Childhood Diarrheal Incidence Among Patients at Hoima Regional Referral Hospital, Western UgandaDocument14 pagesInvestigating Key Determinants of Childhood Diarrheal Incidence Among Patients at Hoima Regional Referral Hospital, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Factors Contributing To Malnutrition Among HIV Positive Children Aged Between 6 and 60 MonthsDocument10 pagesFactors Contributing To Malnutrition Among HIV Positive Children Aged Between 6 and 60 MonthsInternational Organization of Scientific Research (IOSR)No ratings yet
- Article Assignment 3 - Breanna LaliberteDocument3 pagesArticle Assignment 3 - Breanna Laliberteapi-240098584No ratings yet
- 2246-Article Text-8369-9706-10-20230606Document11 pages2246-Article Text-8369-9706-10-20230606Gek Sinta ManuabaNo ratings yet
- SYNOPSIS. MalnutritionDocument3 pagesSYNOPSIS. MalnutritionManish JainNo ratings yet
- Prevalence of Malnutrition Among Pre-School Children In, South-East NigeriaDocument5 pagesPrevalence of Malnutrition Among Pre-School Children In, South-East NigeriadsNo ratings yet
- Journal of Biosocial ScienceDocument14 pagesJournal of Biosocial ScienceOpen mindNo ratings yet
- Determinants of Undernutrition Among Young Children in EthiopiaDocument18 pagesDeterminants of Undernutrition Among Young Children in EthiopiaElijah IbsaNo ratings yet
- Factors Influencing Breastfeeding Practices Among Mothers in Lafia LocalDocument13 pagesFactors Influencing Breastfeeding Practices Among Mothers in Lafia LocalCha Tozenity ChieNo ratings yet
- Bahati FinalDocument14 pagesBahati FinalmwahalendejofreyNo ratings yet
- A Study On The Nutritional Status of Children in Mawlai Iewrynghep, East Khasi Hills District, Meghalaya (India)Document7 pagesA Study On The Nutritional Status of Children in Mawlai Iewrynghep, East Khasi Hills District, Meghalaya (India)archerselevatorsNo ratings yet
- Ajol File Journals - 87 - Articles - 173693 - Submission - Proof - 173693 1033 444977 1 10 20180625Document7 pagesAjol File Journals - 87 - Articles - 173693 - Submission - Proof - 173693 1033 444977 1 10 20180625Grace ArthurNo ratings yet
- Assessment of Nutritional Status Among Children Less Than 5 Years Old in Hilla CityDocument5 pagesAssessment of Nutritional Status Among Children Less Than 5 Years Old in Hilla CityJASH MATHEWNo ratings yet
- Journal Pre-Proof: Clinical Epidemiology and Global HealthDocument22 pagesJournal Pre-Proof: Clinical Epidemiology and Global HealthClaudia BuheliNo ratings yet
- Nigeria PDFDocument16 pagesNigeria PDFrima weniNo ratings yet
- Infant and Young Child Feeding PracticesDocument10 pagesInfant and Young Child Feeding Practicesblesslendor128No ratings yet
- School FeedingDocument13 pagesSchool FeedingJanelle MayonteNo ratings yet
- Dietary Diversity Score and Associated Factors Among High School Adolescent Girls in Gurage Zone, Southwest EthiopiaDocument5 pagesDietary Diversity Score and Associated Factors Among High School Adolescent Girls in Gurage Zone, Southwest EthiopiaFadhila NurrahmaNo ratings yet
- Nutritional Status of Under-Five Children Living inDocument7 pagesNutritional Status of Under-Five Children Living inUli Kartika SihalohoNo ratings yet
- A Survey of Undernutrition in Children Under Three Years of Age in Rural Western ChinaDocument10 pagesA Survey of Undernutrition in Children Under Three Years of Age in Rural Western ChinaCherryNo ratings yet
- Nutritional Status and Associated Factors Among School Adolescent in Chiro Town, West Hararge, EthiopiaDocument11 pagesNutritional Status and Associated Factors Among School Adolescent in Chiro Town, West Hararge, EthiopiaZEsca C'vivi LovlyDie Flow IINo ratings yet
- Prevalence of MalnutritionDocument7 pagesPrevalence of Malnutritionsara sisayNo ratings yet
- Risk Correlates of Diarrhea in Children Under 5 Years of Age in Slums of Bankura, West BengalDocument8 pagesRisk Correlates of Diarrhea in Children Under 5 Years of Age in Slums of Bankura, West BengalSanaNo ratings yet
- A Study On The Relationship Between Nutritional Status and Prevalence of Pneumonia and Diarrhoea Among Preschool Children in KushtiaDocument10 pagesA Study On The Relationship Between Nutritional Status and Prevalence of Pneumonia and Diarrhoea Among Preschool Children in KushtiaSukmaNo ratings yet
- Stunting and Anemia Among Children 6 - 23 Months Old in Damot Sore District, Southern EthiopiaDocument11 pagesStunting and Anemia Among Children 6 - 23 Months Old in Damot Sore District, Southern EthiopiaAchmad YunusNo ratings yet
- Dnhe 04 Project Proposal by Dt. Puneet KumarDocument13 pagesDnhe 04 Project Proposal by Dt. Puneet KumarPuneet KumarNo ratings yet
- Assessment of Nutritional Status of Children in Al Hilla CityDocument8 pagesAssessment of Nutritional Status of Children in Al Hilla CityKamruzzaman ManikNo ratings yet
- ResearchDocument10 pagesResearchGildred Rada BerjaNo ratings yet
- EJCM - Volume 36 - Issue 1 - Pages 45-60-1Document16 pagesEJCM - Volume 36 - Issue 1 - Pages 45-60-1Yaumil FauziahNo ratings yet
- Jurnal Ika 1Document11 pagesJurnal Ika 1jihadahNo ratings yet
- Abera2017 Prevalence of Malnutrition and Associated Factors in EthiopiaDocument8 pagesAbera2017 Prevalence of Malnutrition and Associated Factors in EthiopiaSHILPA PATILNo ratings yet
- Factors Influencing Anemia and Night Blindness Among Children Less Than Five Years Old (0 - 4.11 Years) in Khartoum State, SudanDocument13 pagesFactors Influencing Anemia and Night Blindness Among Children Less Than Five Years Old (0 - 4.11 Years) in Khartoum State, SudanAmin MojiriNo ratings yet
- 10 11648 J SJPH 20130102 12Document6 pages10 11648 J SJPH 20130102 12SukmaNo ratings yet
- 4 - Factors Associated With Malnutrition inDocument7 pages4 - Factors Associated With Malnutrition inRezki Purnama YusufNo ratings yet
- 259 Risk Factors For Severe Acute Malnutrition inDocument10 pages259 Risk Factors For Severe Acute Malnutrition inVibhor Kumar JainNo ratings yet
- Prevalence and Determinants of Overweight and Obesity Among School-Aged Children and AdolescentsDocument8 pagesPrevalence and Determinants of Overweight and Obesity Among School-Aged Children and AdolescentsIJPHSNo ratings yet
- Vol 05 Issue 02 Section: Healthcare Category: Research Received On: 02/12/12 Revised On: 27/12/12 Accepted On: 16/01/13Document6 pagesVol 05 Issue 02 Section: Healthcare Category: Research Received On: 02/12/12 Revised On: 27/12/12 Accepted On: 16/01/13Dwitiara SeptianiNo ratings yet
- Prevalence of Malnutrition Among Hospitalized Children: June 2014Document4 pagesPrevalence of Malnutrition Among Hospitalized Children: June 2014Imin BuntaraNo ratings yet
- 5 Determinants of Acute Malnutrition Among ChildrenDocument8 pages5 Determinants of Acute Malnutrition Among ChildrenRezki Purnama YusufNo ratings yet
- 1 s2.0 S2666149722000202 MainDocument6 pages1 s2.0 S2666149722000202 MainALEXANDRE SOUSANo ratings yet
- Prevalence of Stunting and Associated Factors of Children Among 6-59 Months Age in Guto Gida District, East Wollega Zone, Oromia, EthiopiaDocument18 pagesPrevalence of Stunting and Associated Factors of Children Among 6-59 Months Age in Guto Gida District, East Wollega Zone, Oromia, EthiopiaFeizar Nak SpentuNo ratings yet
- Jurnal Internasional 2Document4 pagesJurnal Internasional 2Ria SaputriNo ratings yet
- Appraisal of Nursing Mothers' Knowledge and Practice ofDocument8 pagesAppraisal of Nursing Mothers' Knowledge and Practice ofAlexander DeckerNo ratings yet
- Bete Bo 2017Document18 pagesBete Bo 2017Zemenu AddissNo ratings yet
- A Study of Acute Malnutrition Among Children in NRCDocument11 pagesA Study of Acute Malnutrition Among Children in NRCkharemixNo ratings yet
- Point-Of-Purchase Health Information Encourages Customers To Purchase Vegetables: Objective Analysis by Using A Point-Of-Sales SystemDocument8 pagesPoint-Of-Purchase Health Information Encourages Customers To Purchase Vegetables: Objective Analysis by Using A Point-Of-Sales SystemMark Lee BaincoNo ratings yet
- EVM Module While On Quarantine - SectionDocument10 pagesEVM Module While On Quarantine - SectionFish BallNo ratings yet
- A Phenomenological Study: Parent Children With AutismDocument338 pagesA Phenomenological Study: Parent Children With AutismDonna Barrow-GreenNo ratings yet
- Mamas Pizza Nutrition FactsDocument2 pagesMamas Pizza Nutrition FactsMonicaNo ratings yet
- Discharge PlanDocument1 pageDischarge PlanlaehaaaNo ratings yet
- Working in Early Childhood - Learner Guide - High Res V1.0 (ID 186109)Document68 pagesWorking in Early Childhood - Learner Guide - High Res V1.0 (ID 186109)Andrea AndersonNo ratings yet
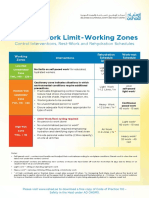
- Thermal Work Limit-Working Zones: Control Interventions, Rest-Work and Rehydration SchedulesDocument1 pageThermal Work Limit-Working Zones: Control Interventions, Rest-Work and Rehydration SchedulesSuprkliNo ratings yet
- Kavitha SDocument223 pagesKavitha SAshwinee KadelNo ratings yet
- Listening 10-8Document2 pagesListening 10-8Duy DươngNo ratings yet
- MAZENOD COLLEGE WEIGHT ROOM - Students (NEW FORM)Document1 pageMAZENOD COLLEGE WEIGHT ROOM - Students (NEW FORM)ThatGuyJosephNo ratings yet
- A Comparative Study On Selected Anthropometrical and Motor Ability Variables Among Inter Collegiate Kabaddi PlayersDocument5 pagesA Comparative Study On Selected Anthropometrical and Motor Ability Variables Among Inter Collegiate Kabaddi PlayersLindon DillyNo ratings yet
- Pricelist2024 YENDocument372 pagesPricelist2024 YENATAY OZOKEEVNo ratings yet
- PSM10-Motivation and Awareness) SG-21Document10 pagesPSM10-Motivation and Awareness) SG-21Muhammad saadNo ratings yet
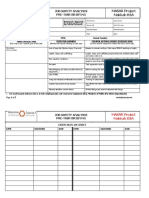
- Job Safety Analysis Pre-Task Briefing: MASAR Project Makkah KSADocument2 pagesJob Safety Analysis Pre-Task Briefing: MASAR Project Makkah KSAmahammed saleem100% (2)
- Job Satisfaction and Human BehaviorDocument22 pagesJob Satisfaction and Human BehaviorEdgardo M. delacruz100% (2)
- Cholesterol LDL Precipitating Reagent: Biosystems S.ADocument1 pageCholesterol LDL Precipitating Reagent: Biosystems S.Ajef1234321No ratings yet
- The Benefits of Corporate Social ResponsibilityDocument2 pagesThe Benefits of Corporate Social ResponsibilityDavid Stivens CastroNo ratings yet
- Neocon 2017Document71 pagesNeocon 2017Jasleen KaurNo ratings yet
- DM in Pregnancy PDFDocument89 pagesDM in Pregnancy PDFMichael Angelo BrinezNo ratings yet
- Drug Study Calcium GluconateDocument1 pageDrug Study Calcium GluconateLarah Mae AndogNo ratings yet
- Crossdressing GuideDocument155 pagesCrossdressing GuideSofiaPasserini78% (9)
- TLE G6 Q2 Module 1Document10 pagesTLE G6 Q2 Module 1Matt The idkNo ratings yet
- Report-on-Safety-Seal-Certification-2021 (October 21-27, 2021)Document4 pagesReport-on-Safety-Seal-Certification-2021 (October 21-27, 2021)Mecs NidNo ratings yet
- Module 4 Unified Course Pack CWTS 1 2022 2023Document30 pagesModule 4 Unified Course Pack CWTS 1 2022 2023Jan Rey RizonNo ratings yet
- December2023 - V1 Bee Cultura AbejaDocument100 pagesDecember2023 - V1 Bee Cultura AbejaVictor Hugo UñoNo ratings yet
- Demon Back Lv1: Week1 Week2 Week3 Week4 Week5 Week6 Week7 Week8Document1 pageDemon Back Lv1: Week1 Week2 Week3 Week4 Week5 Week6 Week7 Week8Severi NurminenNo ratings yet
- Resume FinalDocument3 pagesResume Finalapi-660462296No ratings yet
- Blossom (Phase 4) : Female Infertility - Luteal Phase FormulaDocument6 pagesBlossom (Phase 4) : Female Infertility - Luteal Phase FormulaJohn FightakisNo ratings yet
- Florence Nightingales Theory of NursingDocument20 pagesFlorence Nightingales Theory of NursingJay-ar Jay-arNo ratings yet
- Ginott TheoryDocument21 pagesGinott TheoryUmmu SalmahNo ratings yet