You might also like
- At the Precipice: My Three-Year Journey from Stroke to Good Health with Type 2 DiabetesFrom EverandAt the Precipice: My Three-Year Journey from Stroke to Good Health with Type 2 DiabetesNo ratings yet
- Mr J's Ant Infestation and Rheumatoid Arthritis ManagementDocument10 pagesMr J's Ant Infestation and Rheumatoid Arthritis ManagementmisswongNo ratings yet
- SOAP Note DiabetesDocument16 pagesSOAP Note Diabetesmichael thorn92% (25)
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- PBL Week 3Document5 pagesPBL Week 3alfredNo ratings yet
- Diabetic Case StudyDocument8 pagesDiabetic Case Studyrenana12100% (1)
- Diabetes Mellitus CuredDocument12 pagesDiabetes Mellitus CuredsherryNo ratings yet
- Diabetes Mellitus of The Human Digestive SystemDocument7 pagesDiabetes Mellitus of The Human Digestive SystemCHRISTINE KARENDINo ratings yet
- NP Case Example TwoDocument5 pagesNP Case Example TwoAnisaNo ratings yet
- PracticeExam CCSDocument12 pagesPracticeExam CCSBehrouz Yari75% (4)
- T2.DM&Obesity - Case - 2022Document14 pagesT2.DM&Obesity - Case - 2022Rhianna HarrisNo ratings yet
- Title: 1. Case Study 1 2. Case Study 2 3. Case Study 3 4. Case Study 4 5. Case Study 5 6. Case Study 6Document33 pagesTitle: 1. Case Study 1 2. Case Study 2 3. Case Study 3 4. Case Study 4 5. Case Study 5 6. Case Study 6drpraveendevarbhaviNo ratings yet
- Kasus EndokrinDocument8 pagesKasus EndokrinBani Adam AnindyaNo ratings yet
- Diabetes Case StudyDocument9 pagesDiabetes Case StudyFajri Nur PrasetyoNo ratings yet
- Nursing Care Plan for Mr. Tommy's Diabetes ManagementDocument6 pagesNursing Care Plan for Mr. Tommy's Diabetes ManagementTeddy LocNo ratings yet
- Diabetes Mellitus in PediatricsDocument22 pagesDiabetes Mellitus in PediatricsKermaigne MirandaNo ratings yet
- Diabetes diagnosis and managementDocument25 pagesDiabetes diagnosis and managementjljoioiuNo ratings yet
- l01.Htn .CaseDocument29 pagesl01.Htn .CaseFaith Castillo100% (2)
- Problem Based Learning in Endocrine Nursing-ADocument3 pagesProblem Based Learning in Endocrine Nursing-AjesperdomincilbayauaNo ratings yet
- Statin Therapy: Accepted BMI Ranges AreDocument23 pagesStatin Therapy: Accepted BMI Ranges AreDfaid NGNo ratings yet
- Transcribed HWDocument2 pagesTranscribed HWnikka aquinoNo ratings yet
- Dr. Rabia 1700 Plab Material McqsDocument1,092 pagesDr. Rabia 1700 Plab Material McqsMuhammad Amin100% (9)
- Blood Test Results - Your Guide To Understanding The Numbers NNHDocument21 pagesBlood Test Results - Your Guide To Understanding The Numbers NNHSN Wijesinhe100% (2)
- Brian Foster's Chest Pain AssessmentDocument4 pagesBrian Foster's Chest Pain AssessmentMallory ZaborNo ratings yet
- Group 3 (Myers) : White MaleDocument7 pagesGroup 3 (Myers) : White MaleMerry Joy DeliñaNo ratings yet
- Dietetics Case Study: Acute MI QuestionsDocument8 pagesDietetics Case Study: Acute MI Questionsapi-434982019No ratings yet
- New Microsoft Word DocumentDocument6 pagesNew Microsoft Word Documentragavan86No ratings yet
- Acute Pancreatitis Case StudyDocument39 pagesAcute Pancreatitis Case StudyJm Bernardo100% (1)
- Metabolic and Endocrine 2010 With AnswersDocument15 pagesMetabolic and Endocrine 2010 With AnswersWenzy CruzNo ratings yet
- Case Study 1 - DMDocument9 pagesCase Study 1 - DMapi-368453103No ratings yet
- Group 5 HFDocument21 pagesGroup 5 HFJerson Aizpuro SuplementoNo ratings yet
- M1 MET1 SG ACaseofAcuteCholecystitisDocument14 pagesM1 MET1 SG ACaseofAcuteCholecystitisNicholas ReljaNo ratings yet
- Letters Combined (11 Referral, 2 Discharge, 1 Transfer)Document49 pagesLetters Combined (11 Referral, 2 Discharge, 1 Transfer)Faisal ImtiazNo ratings yet
- Diabetes Case Study: Goals and Treatment PlanDocument3 pagesDiabetes Case Study: Goals and Treatment PlanRoxanne Nasingao100% (1)
- Chapter 12 - Hypertension - Pass The Salt, Please Level IIDocument7 pagesChapter 12 - Hypertension - Pass The Salt, Please Level IIRichix K Yabe0% (1)
- Case 1Document15 pagesCase 1api-272660148100% (1)
- NUR 377 Advanced Medical Surgical Nursing vSim Course Point PharmacologyDocument5 pagesNUR 377 Advanced Medical Surgical Nursing vSim Course Point PharmacologyMichelle Pinkhasova100% (3)
- YL3 GI End of Module Activity Complex Task - StudentsDocument1 pageYL3 GI End of Module Activity Complex Task - StudentsAnonymous Xlpj86laNo ratings yet
- 1st Case Session ToT CPG HPTDocument124 pages1st Case Session ToT CPG HPThakimahsNo ratings yet
- Case PediatricsDocument6 pagesCase PediatricsHarsh NimavatNo ratings yet
- Metabolic Disease Case Study Learning ActivityDocument8 pagesMetabolic Disease Case Study Learning ActivityKhali Sciola0% (1)
- Diabetic Ketoacidosis Case PresentationDocument37 pagesDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- Resource Unit On Hypertension.Document14 pagesResource Unit On Hypertension.Eloina Grace Obrero RuleteNo ratings yet
- All CasesDocument32 pagesAll CasesMona NasrNo ratings yet
- JT Family Med OSCE NotesDocument5 pagesJT Family Med OSCE NotesNathan KimNo ratings yet
- Case Study 1Document15 pagesCase Study 1api-272464131100% (2)
- Reading Test - 5 Diabetes Text A: Clinical AssessmentDocument16 pagesReading Test - 5 Diabetes Text A: Clinical AssessmentJisha JanardhanNo ratings yet
- Pediatrics CaseDocument6 pagesPediatrics CaseHarsh NimavatNo ratings yet
- Nursing NoteDocument6 pagesNursing Noteshiller0% (1)
- MEQ Faisal 2023Document3 pagesMEQ Faisal 2023Faisal AlmohailebNo ratings yet
- Sample Case StudyDocument10 pagesSample Case Studyapi-702059884No ratings yet
- Feedback: Case StudyDocument12 pagesFeedback: Case StudyTiffany Sabilla RamadhaniNo ratings yet
- DiabetesDocument26 pagesDiabetesAlina Juliana MagopetNo ratings yet
- Case Simulation 118Document4 pagesCase Simulation 118Rica AvendañoNo ratings yet
- Prevention: Can Prediabetes, Type 2 Diabetes and Gestational Diabetes Be Prevented?Document9 pagesPrevention: Can Prediabetes, Type 2 Diabetes and Gestational Diabetes Be Prevented?BethChay LacsonNo ratings yet
- M M M MDocument8 pagesM M M MAudrey MaeNo ratings yet
- PBL PgamboaDocument6 pagesPBL PgamboaLeanne Princess GamboaNo ratings yet
- Acute Pancreatitis PathoDocument5 pagesAcute Pancreatitis PathoENo ratings yet
- Case Studies in Managing GG Hypertension: Defining The Barriers To ControlDocument37 pagesCase Studies in Managing GG Hypertension: Defining The Barriers To Controlkirubel deribNo ratings yet
- Unit 2 ReviewDocument5 pagesUnit 2 Reviewduonghi3lpsNo ratings yet
- Blood Doping PPT PresentationDocument26 pagesBlood Doping PPT Presentationee4254100% (1)
- Bedside Pulmonary Function TestDocument2 pagesBedside Pulmonary Function TestChandan SardarNo ratings yet
- Nervous CoordinationDocument45 pagesNervous CoordinationTajXNo ratings yet
- Patient-Ventilator AsynchronyDocument14 pagesPatient-Ventilator AsynchronyJavier Enrique Barrera PachecoNo ratings yet
- Disturbances in OxygenationDocument10 pagesDisturbances in OxygenationjenrylNo ratings yet
- Research Article on Characteristics of Coronary Heart Disease Patients in North MalukuDocument10 pagesResearch Article on Characteristics of Coronary Heart Disease Patients in North MalukuAbduNo ratings yet
- Drugs Affecting Respiratory SystemDocument19 pagesDrugs Affecting Respiratory SystemRuby Ann DimayugaNo ratings yet
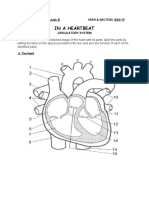
- Circulatory System ActivityDocument5 pagesCirculatory System ActivityKeen Jude CaminosNo ratings yet
- DIB - Week 01 - 02 - Anatomy & Physiology PDFDocument99 pagesDIB - Week 01 - 02 - Anatomy & Physiology PDFFaisal MujibNo ratings yet
- Muscular System Final1Document33 pagesMuscular System Final1Karl Maurice ApogNo ratings yet
- Session 1Document15 pagesSession 1Feona82No ratings yet
- Drug Study Module 5Document3 pagesDrug Study Module 5Krisyll Meah Torred RamalNo ratings yet
- General Pathology - Topical Past Papers-1Document21 pagesGeneral Pathology - Topical Past Papers-1RazaNo ratings yet
- Fatigue PowerPoint Presentation Compatibility ModeDocument96 pagesFatigue PowerPoint Presentation Compatibility ModePouryaNo ratings yet
- Test Bank For High Acuity Nursing 6th Edition Kathleen Dorman WagnerDocument18 pagesTest Bank For High Acuity Nursing 6th Edition Kathleen Dorman WagnerDavidRobinsonfikq100% (35)
- Spontaneously, Without A Known CauseDocument6 pagesSpontaneously, Without A Known CauseAnalyn SarmientoNo ratings yet
- Drugs and The Brain - CourseraDocument5 pagesDrugs and The Brain - CourseraSinisa RisticNo ratings yet
- Cells Tissues Organs and Systems Power PointDocument11 pagesCells Tissues Organs and Systems Power PointNidonama E. KabmatNo ratings yet
- Varicose VeinsDocument2 pagesVaricose VeinsroycNo ratings yet
- Julie Bui - Respiratory System WorksheetDocument4 pagesJulie Bui - Respiratory System Worksheetapi-522650514No ratings yet
- Nursing Care Plan - Impaired DentitionDocument18 pagesNursing Care Plan - Impaired Dentitionken kiplimoNo ratings yet
- Nutrition Considerations PDFDocument11 pagesNutrition Considerations PDFNutricion Buap ComdeNo ratings yet
- Physiological:biological Psychology NotesDocument36 pagesPhysiological:biological Psychology NotesjeynNo ratings yet
- 12 Tips to Stay Awake NaturallyDocument14 pages12 Tips to Stay Awake NaturallyJohayra AbbasNo ratings yet
- NCP Deficient Fluid VolumeDocument5 pagesNCP Deficient Fluid VolumeCHRISTINE GRACE ELLONo ratings yet
- Cardiomyopathy and myocarditis: Causes, symptoms, diagnosis and treatmentDocument69 pagesCardiomyopathy and myocarditis: Causes, symptoms, diagnosis and treatmentImmanuel100% (1)
- Chapter 12 - The Lymphatic System and Body DefensesDocument16 pagesChapter 12 - The Lymphatic System and Body DefensesHannah Lee LumosbogNo ratings yet
- Group 5 Bahasa Inggris 2Document12 pagesGroup 5 Bahasa Inggris 2Desri AjengNo ratings yet
- Cardiovascular Physiology Review QuestionsDocument44 pagesCardiovascular Physiology Review QuestionsTim100% (1)
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDFrom EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDRating: 4 out of 5 stars4/5 (8)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Drop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)From EverandDrop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Rating: 4.5 out of 5 stars4.5/5 (52)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- Food of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionFrom EverandFood of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionRating: 4.5 out of 5 stars4.5/5 (117)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholFrom EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholRating: 4 out of 5 stars4/5 (6)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.From EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Rating: 4 out of 5 stars4/5 (7)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- The Language of Letting Go: Daily Meditations on CodependencyFrom EverandThe Language of Letting Go: Daily Meditations on CodependencyRating: 4.5 out of 5 stars4.5/5 (18)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryFrom EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryRating: 5 out of 5 stars5/5 (47)