You might also like
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Asa 2013Document1,076 pagesAsa 2013Marwa Mahrous100% (4)
- Technical Aspects of Focal Therapy in Localized Prostate CancerFrom EverandTechnical Aspects of Focal Therapy in Localized Prostate CancerEric BarretNo ratings yet
- Guidance For Return To Practice For Otolaryngology-Head and Neck SurgeryDocument10 pagesGuidance For Return To Practice For Otolaryngology-Head and Neck SurgeryLeslie Lindsay AlvarezNo ratings yet
- Perioperative Medicine: The Pathway To Better Surgical CareDocument28 pagesPerioperative Medicine: The Pathway To Better Surgical CareLee SungjongNo ratings yet
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyFrom EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyNo ratings yet
- Postoperative Care: Who Should Look After Patients Following Surgery?Document5 pagesPostoperative Care: Who Should Look After Patients Following Surgery?kishanm77No ratings yet
- RO-ILS Case StudyDocument4 pagesRO-ILS Case Studyapi-458422967No ratings yet
- Tutorials in Surgery For 4th Medical StudentsDocument180 pagesTutorials in Surgery For 4th Medical StudentsAnonymous jSTkQVC27bNo ratings yet
- 1.7 Right Person, Right Place, Right Time PDFDocument3 pages1.7 Right Person, Right Place, Right Time PDFKaren Osorio GilardiNo ratings yet
- Romanian Journal Analyzes Ethics of Hospital Stays After Tonsil SurgeryDocument4 pagesRomanian Journal Analyzes Ethics of Hospital Stays After Tonsil SurgeryMeva'a RogerNo ratings yet
- Module 1 Case StudyDocument7 pagesModule 1 Case StudyDivine ParagasNo ratings yet
- CX Preprotesica OOODocument4 pagesCX Preprotesica OOOMich ReynosoNo ratings yet
- Thesis On Incisional HerniaDocument4 pagesThesis On Incisional Herniapsmxiiikd100% (1)
- Surgical Preoperative Assessment - What To Do and Why? Student BMJDocument3 pagesSurgical Preoperative Assessment - What To Do and Why? Student BMJEd FitzgeraldNo ratings yet
- Radiation Safety-Nicolette SawickiDocument4 pagesRadiation Safety-Nicolette Sawickiapi-484758207No ratings yet
- Peninsula Cornwall - Pressure DamageDocument33 pagesPeninsula Cornwall - Pressure DamageDeepa JeyaseelanNo ratings yet
- Kakulamarri Pranav Ra2 10-13-17Document3 pagesKakulamarri Pranav Ra2 10-13-17api-373095622No ratings yet
- Incisional Hernia ThesisDocument5 pagesIncisional Hernia Thesisgbwy79ja100% (1)
- Cts ArticlesDocument4 pagesCts ArticlesdrarunraoNo ratings yet
- Thesis Topics in Interventional RadiologyDocument7 pagesThesis Topics in Interventional Radiologygjfcp5jb100% (2)
- Response ToDocument7 pagesResponse ToReza AbdarNo ratings yet
- Misconceptions and Safety in Radiation OncologyDocument5 pagesMisconceptions and Safety in Radiation Oncologyapi-692385376No ratings yet
- My Own Opinion TextDocument3 pagesMy Own Opinion TextM. Ricko NugrohoNo ratings yet
- Radiation Safety Paper 1Document3 pagesRadiation Safety Paper 1api-633087057No ratings yet
- Management of Pertrochanteric Fractures inDocument8 pagesManagement of Pertrochanteric Fractures inantonio dengNo ratings yet
- Ro-Ils PaperDocument4 pagesRo-Ils Paperapi-502011468No ratings yet
- Safety EssayDocument5 pagesSafety Essayapi-350437453No ratings yet
- Ethics Anda LawDocument12 pagesEthics Anda LawSiti Fatimahtusz07No ratings yet
- Day CaseDocument43 pagesDay CaseKamel HadyNo ratings yet
- Research Paper On Nurse AnesthetistDocument6 pagesResearch Paper On Nurse Anesthetistgw1gnz6b100% (1)
- Short and Long-Term Outcomes After Surgical Procedures Lasting For More Than Six HoursDocument8 pagesShort and Long-Term Outcomes After Surgical Procedures Lasting For More Than Six HoursDickyNo ratings yet
- Radiation Safety PaperDocument4 pagesRadiation Safety Paperapi-632529930No ratings yet
- Paediatric Ambulatory Surgery - Perioperative Concerns: Dr. Pramila Chari Dr. Indu SenDocument7 pagesPaediatric Ambulatory Surgery - Perioperative Concerns: Dr. Pramila Chari Dr. Indu SenT RonaskyNo ratings yet
- Anesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFDocument11 pagesAnesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFtiaraleshaNo ratings yet
- Cirugia AmbulatoriaDocument17 pagesCirugia AmbulatoriaCarlos Guillermo Chillihuani CanoNo ratings yet
- Thyroid Surgery DissertationDocument5 pagesThyroid Surgery DissertationDoMyPaperCanada100% (1)
- Dissertation Topics For MD AnaesthesiaDocument4 pagesDissertation Topics For MD AnaesthesiaWhitePaperWritingServicesCanada100% (1)
- Care Elderly 01Document16 pagesCare Elderly 01Emyx MaNo ratings yet
- Pre Hospital PDFDocument4 pagesPre Hospital PDFAndi Tri SutrisnoNo ratings yet
- Paediatric Radiography DissertationDocument4 pagesPaediatric Radiography DissertationGhostWriterCollegePapersHartford100% (1)
- 13 Anaesthesia Outside The OR AC 2016Document18 pages13 Anaesthesia Outside The OR AC 2016Anastesiologi CNo ratings yet
- Uhns Guidelines 2010Document187 pagesUhns Guidelines 2010varrakesh100% (1)
- 37 157 1 PB PDFDocument4 pages37 157 1 PB PDFDhea Amalia WibowoNo ratings yet
- Anesthesia Cosmetic SurgeryDocument7 pagesAnesthesia Cosmetic SurgerySergio ArbelaezNo ratings yet
- Radiation Safety PaperDocument4 pagesRadiation Safety Paperapi-525837437No ratings yet
- Basic Patient NeedsDocument15 pagesBasic Patient NeedsMarggie SalaoNo ratings yet
- Thesis On Episiotomy Wound HealingDocument5 pagesThesis On Episiotomy Wound HealingCollegePapersForSaleCanada100% (2)
- Preoperative, Anesthetic, and Postoperative Care For Rhinoplasty PatientsDocument7 pagesPreoperative, Anesthetic, and Postoperative Care For Rhinoplasty PatientsTarek abo kammerNo ratings yet
- Radiation Safety Essay Ryan MonagoDocument5 pagesRadiation Safety Essay Ryan Monagoapi-632682404No ratings yet
- InterviewDocument3 pagesInterviewapi-486625755No ratings yet
- Assessment and Management of Preoperative AnxietyDocument6 pagesAssessment and Management of Preoperative AnxietyFiorel Loves EveryoneNo ratings yet
- Non-Operatingroom Anesthesia: The Principles of Patient Assessment and PreparationDocument18 pagesNon-Operatingroom Anesthesia: The Principles of Patient Assessment and PreparationEolia EffendiNo ratings yet
- Groot Koerkamp, BasDocument231 pagesGroot Koerkamp, BasHelmy BahdalaNo ratings yet
- 10 1005 - Continuous Patient MonitoringDocument3 pages10 1005 - Continuous Patient MonitoringChristian KleinNo ratings yet
- CDVC and Integrated Practice Unit for Cancer CareDocument6 pagesCDVC and Integrated Practice Unit for Cancer CareAbdullah Alhurani100% (1)
- An Research Surrpunding The Profession, SurgeonDocument6 pagesAn Research Surrpunding The Profession, SurgeonKaizen257No ratings yet
- Roils 1Document4 pagesRoils 1api-574059920No ratings yet
- April2019JuniorCriticalCareFellowJDDocument6 pagesApril2019JuniorCriticalCareFellowJDM LubisNo ratings yet
- Internship ReportDocument15 pagesInternship Reportpreethi balakrishnanNo ratings yet
- Professional AdvancementDocument51 pagesProfessional AdvancementReshma AnilkumarNo ratings yet
- Population Trends in INDIADocument8 pagesPopulation Trends in INDIAcheedikrishnaNo ratings yet
- Breech BirthDocument10 pagesBreech Birthcirlce:twoworldsconnectedNo ratings yet
- Implementasi SPM Kesehatan Bayi Baru Lahir di Puskesmas DukuhsetiDocument10 pagesImplementasi SPM Kesehatan Bayi Baru Lahir di Puskesmas DukuhsetiFidia sariNo ratings yet
- No Article Title Time of Publication Authors Journal Name Received Date Revised Date Accepted DateDocument4 pagesNo Article Title Time of Publication Authors Journal Name Received Date Revised Date Accepted DateAnin Kalma MartadinataNo ratings yet
- Tobacco Free Generation Next - M. Amebari NongsiejDocument2 pagesTobacco Free Generation Next - M. Amebari NongsiejM. Amebari NongsiejNo ratings yet
- Continuous Insulin InfusionDocument6 pagesContinuous Insulin Infusionbobobo22No ratings yet
- Nurse Midwife PractionersDocument8 pagesNurse Midwife PractionersVineeta JoseNo ratings yet
- Small Spaces Need Smart Solutions - Kristoffer ThøgersenDocument12 pagesSmall Spaces Need Smart Solutions - Kristoffer ThøgersenTuan Huy Le100% (1)
- Mayasthenia Gravis NclexDocument47 pagesMayasthenia Gravis NclexKrishna SapkotaNo ratings yet
- Theodore Millon On Rosenhan PaperDocument6 pagesTheodore Millon On Rosenhan PaperJuliette WarnesNo ratings yet
- Nestle PolicyDocument29 pagesNestle PolicyMuhammad HarlandNo ratings yet
- Parasitology SummaryDocument7 pagesParasitology Summaryshiner99100% (1)
- Career Day Brochure FinalDocument2 pagesCareer Day Brochure Finalapi-375229945No ratings yet
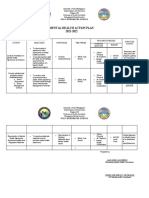
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
- Alt - Cancer (1) BookDocument419 pagesAlt - Cancer (1) Bookniceia matos100% (3)
- Dragon BoatDocument7 pagesDragon BoatandrewadrianNo ratings yet
- Psychosocial interventions ease suffering in complex palliative care patientsDocument7 pagesPsychosocial interventions ease suffering in complex palliative care patientsSiti Malkah KamilahNo ratings yet
- Mental Health EssayDocument2 pagesMental Health EssayROHITNo ratings yet
- SKF MSDS LGHP 2 PDFDocument5 pagesSKF MSDS LGHP 2 PDFMunkhnasan MonaNo ratings yet
- NYCOSH Letter To DOB Re: OSHA Card Arrests 10262015Document2 pagesNYCOSH Letter To DOB Re: OSHA Card Arrests 10262015Monica NovoaNo ratings yet
- MukokelDocument3 pagesMukokeljulietNo ratings yet
- The Future of Positive Psychology: A Declaration of IndependenceDocument17 pagesThe Future of Positive Psychology: A Declaration of IndependenceEbonnie DiazNo ratings yet
- Patient Information Guide: AH-QF-FO-07Document35 pagesPatient Information Guide: AH-QF-FO-07jose rajanNo ratings yet
- Teks Percakapan Bahasa InggrisDocument2 pagesTeks Percakapan Bahasa Inggrisnaufal456No ratings yet
- Research Proposal On Fast FoodDocument8 pagesResearch Proposal On Fast FoodManish Ravat100% (5)
- Fitness Testing Guide PDFDocument10 pagesFitness Testing Guide PDFdodovadaNo ratings yet
- Understanding Neurology - A Problem-Orientated Approach PDFDocument241 pagesUnderstanding Neurology - A Problem-Orientated Approach PDFAshabul AnharNo ratings yet
- Evidence Based Chinese Medicine HypertensionDocument13 pagesEvidence Based Chinese Medicine Hypertensionpranaji100% (2)