You might also like
- PLAB 2 List of PhrasesDocument4 pagesPLAB 2 List of Phrasesshuvo786100% (4)
- Excrementum Caninum, Eberle, Ritzer, EnglishDocument82 pagesExcrementum Caninum, Eberle, Ritzer, EnglishDr. Khurshid AlamNo ratings yet
- 10 Adult Anesthesia Pre-Operative Evaluation FormDocument1 page10 Adult Anesthesia Pre-Operative Evaluation FormAina HaravataNo ratings yet
- Science: Quarter 1, WK 2 - Module 2Document31 pagesScience: Quarter 1, WK 2 - Module 2Andres Boni85% (13)
- Jurnal Chen Et AlDocument31 pagesJurnal Chen Et AlUtami MNo ratings yet
- 1 s2.0 S0272638620306120 ManinDocument10 pages1 s2.0 S0272638620306120 ManinrezaNo ratings yet
- 2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaDocument4 pages2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaClaav HugNo ratings yet
- Higher Level of Neutrophil-to-Lymphocyte Is Associated With Severe COVID-19Document12 pagesHigher Level of Neutrophil-to-Lymphocyte Is Associated With Severe COVID-19Emier HidayatNo ratings yet
- Clinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaDocument6 pagesClinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaBobanBisercicNo ratings yet
- Piis0923753420363833 PDFDocument26 pagesPiis0923753420363833 PDFSyed HossainNo ratings yet
- Artikel Covid-19Document9 pagesArtikel Covid-19nhshivani532000No ratings yet
- Coronavirus Disease 2019 (COVID-19) A Perspective From ChinaDocument29 pagesCoronavirus Disease 2019 (COVID-19) A Perspective From ChinabackupNo ratings yet
- Estudo DiabetesDocument9 pagesEstudo DiabetesFulano de TalNo ratings yet
- Epidemiological and Clinical Characteristics of 671 COVID-19 Patients in Henan Province, ChinaDocument11 pagesEpidemiological and Clinical Characteristics of 671 COVID-19 Patients in Henan Province, ChinaOrlando JúniorNo ratings yet
- (14374331 - Clinical Chemistry and Laboratory Medicine (CCLM) ) Prominent Changes in Blood Coagulation of Patients With SARS-CoV-2 InfectionDocument5 pages(14374331 - Clinical Chemistry and Laboratory Medicine (CCLM) ) Prominent Changes in Blood Coagulation of Patients With SARS-CoV-2 InfectionMahtosurup GodavarthyNo ratings yet
- 1 s2.0 S0924857920301059 MainDocument13 pages1 s2.0 S0924857920301059 MainNini RinNo ratings yet
- InternacionalDocument9 pagesInternacionalbryan ronaldNo ratings yet
- Clinical Characteristics of Severe Acute Respiratory Syndrome Coronavirus 2 Reactivation Guangming Ye Download 2024 Full ChapterDocument23 pagesClinical Characteristics of Severe Acute Respiratory Syndrome Coronavirus 2 Reactivation Guangming Ye Download 2024 Full Chaptervito.lyons426100% (11)
- Covide 19Document12 pagesCovide 19Hamza MehalliNo ratings yet
- Coronavirus (2019 Ncov) Selected Bibliographic References 12 02 2020 v1Document6 pagesCoronavirus (2019 Ncov) Selected Bibliographic References 12 02 2020 v1Andi SanapatiNo ratings yet
- Association of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Document9 pagesAssociation of Procalcitonin Levels With The Progression and Prognosis of Hospitalized Patients With COVID-19Dian Putri NingsihNo ratings yet
- The Management of Coronavirus Disease 2019 (COVID 19) : Jialin Liu - Siru LiuDocument7 pagesThe Management of Coronavirus Disease 2019 (COVID 19) : Jialin Liu - Siru LiuFina RepitiyanaNo ratings yet
- Ciaa242 2 PDFDocument8 pagesCiaa242 2 PDFHesbon MomanyiNo ratings yet
- Prominent Changes in Blood Coagulation of Patients With Sars-Cov-2 InfectionDocument10 pagesProminent Changes in Blood Coagulation of Patients With Sars-Cov-2 InfectionMuhammad Rizky CaniagoNo ratings yet
- 1 s2.0 S0924857920302211 MainDocument3 pages1 s2.0 S0924857920302211 MainYuniati ValentinaNo ratings yet
- Asymptomatic and Human To Human Transmission of SARS COV 2Document3 pagesAsymptomatic and Human To Human Transmission of SARS COV 2belinda thaniaNo ratings yet
- COVID-19 Screening Prognosis and Severity Assessment With Biomarkers HORIBA MedicalDocument14 pagesCOVID-19 Screening Prognosis and Severity Assessment With Biomarkers HORIBA MedicalIrkania PasangkaNo ratings yet
- Clinical Microbiology and InfectionDocument6 pagesClinical Microbiology and InfectionRaghu NadhNo ratings yet
- Coagulation Disorder PDFDocument4 pagesCoagulation Disorder PDFBrownell TraciNo ratings yet
- Covid Er ArticleDocument6 pagesCovid Er ArticleReeb BukhariNo ratings yet
- The Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudyDocument10 pagesThe Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudygiovannaNo ratings yet
- High-Dose Intravenous Immunoglobulin As A Therapeutic Option For Deteriorating Patients With Coronavirus Disease 2019Document6 pagesHigh-Dose Intravenous Immunoglobulin As A Therapeutic Option For Deteriorating Patients With Coronavirus Disease 2019my accountNo ratings yet
- JMV 25815Document2 pagesJMV 25815fadil ahmadiNo ratings yet
- WHO Declares COVID-19 A Pandemic: Domenico Cucinotta, Maurizio VanelliDocument4 pagesWHO Declares COVID-19 A Pandemic: Domenico Cucinotta, Maurizio VanelliNessa Dila AnandaNo ratings yet
- Ciaa 247Document6 pagesCiaa 247berlian gurningNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument18 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- JCMM 24 6558Document13 pagesJCMM 24 6558Roberto D. GarceteNo ratings yet
- The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaDocument5 pagesThe Clinical and Chest CT Features Associated With Severe and Critical COVID-19 PneumoniaNadanNadhifahNo ratings yet
- Zhou2020 Article CoronavirusDisease2019COVID-19 PDFDocument10 pagesZhou2020 Article CoronavirusDisease2019COVID-19 PDFElena AlexandraNo ratings yet
- TAC COVID 19. LEC-S3-SEM1pdfDocument9 pagesTAC COVID 19. LEC-S3-SEM1pdfJimena Obregon GarciaNo ratings yet
- 2020 Article 78870Document12 pages2020 Article 78870nadaNo ratings yet
- Journal Pre-Proof: Journal of Microbiology, Immunology and InfectionDocument16 pagesJournal Pre-Proof: Journal of Microbiology, Immunology and Infectionbrip selNo ratings yet
- 1.clinical Characteristics of 28 PatientsDocument7 pages1.clinical Characteristics of 28 PatientsTeguh WibowoNo ratings yet
- Journal Pre-Proof: Journal of Clinical VirologyDocument12 pagesJournal Pre-Proof: Journal of Clinical VirologymiNo ratings yet
- Clinico-Radiological Profile in Covid - 19 PatientsDocument6 pagesClinico-Radiological Profile in Covid - 19 PatientsInternational Journal of Innovative Science and Research Technology100% (1)
- Correlation Between Ground-Glass Opacity On Pulmonary CT and The Levels of Inflammatory CytokinesDocument7 pagesCorrelation Between Ground-Glass Opacity On Pulmonary CT and The Levels of Inflammatory CytokinesEarlya RifaniNo ratings yet
- Gastrointestinal Symptoms of 95 Cases With Sars-Cov-2 InfectionDocument5 pagesGastrointestinal Symptoms of 95 Cases With Sars-Cov-2 Infectionjitesh141No ratings yet
- MainDocument7 pagesMainM ANo ratings yet
- Jurnal 6Document2 pagesJurnal 6kalstarNo ratings yet
- Coronavirus Disease 2019 (COVID-19) : A Perspective From ChinaDocument11 pagesCoronavirus Disease 2019 (COVID-19) : A Perspective From Chinasri karuniaNo ratings yet
- Pulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung CancerDocument5 pagesPulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung Cancermuhammad RidoNo ratings yet
- Understanding About CovidDocument5 pagesUnderstanding About CovidChristine Jane RodriguezNo ratings yet
- Combination of RT-QPCR Testing and Clinical Features For Diagnosis of Covid-19 Facilitates Management of Sars-Cov-2 OutbreakDocument7 pagesCombination of RT-QPCR Testing and Clinical Features For Diagnosis of Covid-19 Facilitates Management of Sars-Cov-2 OutbreakPrivate HunterNo ratings yet
- Aksungar 2007Document10 pagesAksungar 2007twarrenNo ratings yet
- A Biological Profile For Diagnosis and Outcome of COVID-19 PatientsDocument10 pagesA Biological Profile For Diagnosis and Outcome of COVID-19 PatientsAristidesNo ratings yet
- ARTIKELDocument6 pagesARTIKELandi susiloNo ratings yet
- A Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesDocument19 pagesA Review of Sars-Cov-2 and The Ongoing Clinical Trials: Molecular SciencesJoseGarciaNo ratings yet
- Characteristics and Mechanism of Liver Injury in 2019 Coronavirus DiseaseDocument5 pagesCharacteristics and Mechanism of Liver Injury in 2019 Coronavirus DiseaseRaaqa AnastaNo ratings yet
- Preliminary Study To Identify Severe From Moderate Cases of COVID-19 Using Combined Hematology ParametersDocument15 pagesPreliminary Study To Identify Severe From Moderate Cases of COVID-19 Using Combined Hematology Parameterstrisna amijayaNo ratings yet
- PIIS0002961020302221Document4 pagesPIIS0002961020302221kuncoroNo ratings yet
- Coronavirus COVID-19 (SARS-CoV-2) - Johns Hopkins ABX GuideDocument12 pagesCoronavirus COVID-19 (SARS-CoV-2) - Johns Hopkins ABX GuidePierre Richard MompremierNo ratings yet
- Research Letters: Co-Infection With Sars-Cov-2 and Influenza A Virus in Patient With Pneumonia, ChinaDocument3 pagesResearch Letters: Co-Infection With Sars-Cov-2 and Influenza A Virus in Patient With Pneumonia, Chinajitesh141No ratings yet
- Journal Pre-Proof: Journal of Clinical VirologyDocument18 pagesJournal Pre-Proof: Journal of Clinical VirologyOkki Wahyu AtikasariNo ratings yet
- Facing COVID-19 with the benefits of medical cannabisFrom EverandFacing COVID-19 with the benefits of medical cannabisNo ratings yet
- Zara Sarzin The Impact of Forced Migration On The Labor Market Outcomes and Welfare of Host CommunitiesDocument45 pagesZara Sarzin The Impact of Forced Migration On The Labor Market Outcomes and Welfare of Host Communitiesabeer alrofaeyNo ratings yet
- War On Ukraine Impact On Ukrainian Medical StudentsDocument3 pagesWar On Ukraine Impact On Ukrainian Medical Studentsabeer alrofaeyNo ratings yet
- Jeffrey R. Wilson Academic WritingDocument363 pagesJeffrey R. Wilson Academic Writingabeer alrofaeyNo ratings yet
- Crosby J 1997 Learning in Small Groups AMEE Education Guide No 8Document14 pagesCrosby J 1997 Learning in Small Groups AMEE Education Guide No 8abeer alrofaeyNo ratings yet
- Dina Abu Ghaida and Karishma Silva Educating The Forcibly Displaced Key Challenges and Opportunities 1Document34 pagesDina Abu Ghaida and Karishma Silva Educating The Forcibly Displaced Key Challenges and Opportunities 1abeer alrofaeyNo ratings yet
- Writing For UniversityDocument128 pagesWriting For Universityabeer alrofaey100% (1)
- Distribution of HCP SirilankaDocument6 pagesDistribution of HCP Sirilankaabeer alrofaeyNo ratings yet
- Mcguirt 1979Document6 pagesMcguirt 1979abeer alrofaeyNo ratings yet
- Czad 002Document15 pagesCzad 002abeer alrofaeyNo ratings yet
- Dental Environment and War-Related Stress Among Dental StudentsDocument8 pagesDental Environment and War-Related Stress Among Dental Studentsabeer alrofaeyNo ratings yet
- Management of Juvenile Ossifying Fibroma in The MaDocument6 pagesManagement of Juvenile Ossifying Fibroma in The Maabeer alrofaeyNo ratings yet
- Aspergillus in Endodontic Infection Near The Maxillary SinusDocument6 pagesAspergillus in Endodontic Infection Near The Maxillary Sinusabeer alrofaeyNo ratings yet
- Fungal Infections of The Maxillary Sinus Case ReportsDocument7 pagesFungal Infections of The Maxillary Sinus Case Reportsabeer alrofaeyNo ratings yet
- Aspergillosis of The Maxillary Sinus in Chronic Myelomonocytic LeukaemiaDocument2 pagesAspergillosis of The Maxillary Sinus in Chronic Myelomonocytic Leukaemiaabeer alrofaeyNo ratings yet
- Barra Para-Aortica Artículo Adela PointevinDocument7 pagesBarra Para-Aortica Artículo Adela Pointevinmod_naiveNo ratings yet
- FNCPDocument3 pagesFNCPFatima Ysabelle Marie RuizNo ratings yet
- Vector Control Intro - Jan2019Document18 pagesVector Control Intro - Jan2019rosana_527421859No ratings yet
- שחזוריםDocument678 pagesשחזוריםTarek Tarek100% (2)
- FFFFFFF: Health Declaration Form Health Declaration Form Health Declaration FormDocument1 pageFFFFFFF: Health Declaration Form Health Declaration Form Health Declaration FormLeny Goyo LaurenteNo ratings yet
- Fact Sheet SpasticityDocument7 pagesFact Sheet SpasticitySajid RahmanNo ratings yet
- Breast Cancer - McMaster Pathophysiology Review PDFDocument8 pagesBreast Cancer - McMaster Pathophysiology Review PDFAprilla Ayu W.No ratings yet
- Psychiatry EdgeDocument1 pagePsychiatry EdgeskNo ratings yet
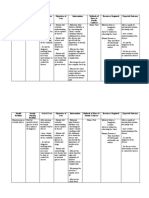
- Defining Characteristics Nursing Diagnosis Outcome Identification Nursing Interventions Rationale EvaluationDocument2 pagesDefining Characteristics Nursing Diagnosis Outcome Identification Nursing Interventions Rationale EvaluationAudrie Allyson GabalesNo ratings yet
- Complex Regional Pain Syndrome: Ens Teaching ReviewDocument8 pagesComplex Regional Pain Syndrome: Ens Teaching ReviewDiego Agustin ZarzaNo ratings yet
- Otitis ExternaDocument14 pagesOtitis ExternaRizkaGayoNo ratings yet
- Asking The Dimensions of SymptomDocument9 pagesAsking The Dimensions of SymptomAnastesiologi CNo ratings yet
- Prof. DR. Dr. Ketut Suastika, SP - PD-KEMD - Management of Growth Hormone Deficiency in AdultDocument31 pagesProf. DR. Dr. Ketut Suastika, SP - PD-KEMD - Management of Growth Hormone Deficiency in AdultvillnachintyaNo ratings yet
- Caustic IngestionDocument16 pagesCaustic IngestionLuanne Rose Dideles-Sandifer100% (1)
- Oncologic NursingDocument16 pagesOncologic NursingDharline Abbygale Garvida AgullanaNo ratings yet
- List Rujukan BPJSDocument104 pagesList Rujukan BPJSpartyNo ratings yet
- Unit 1 FromDocument6 pagesUnit 1 FromjdjdjdhNo ratings yet
- MODIFIED RADICAL MASTOIDECTOMY IN A PATIENT WITH MILD r2Document7 pagesMODIFIED RADICAL MASTOIDECTOMY IN A PATIENT WITH MILD r2Jay Flores San JoseNo ratings yet
- SHAKTI THAKUR MedicalDocument3 pagesSHAKTI THAKUR MedicalNokia5gMHPartner's ReportsNo ratings yet
- 21st - Press Release For Free ScreeningDocument1 page21st - Press Release For Free Screeningapi-288707397No ratings yet
- Cues/Data Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective DataDocument5 pagesCues/Data Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Datatimie_reyesNo ratings yet
- Sarcoma RetroperitonealDocument26 pagesSarcoma Retroperitonealsalas912No ratings yet
- Breast ComplicationsDocument42 pagesBreast ComplicationskurniaNo ratings yet
- The Management of Diarrhoea in Adults: RCN Guidance For Nursing StaffDocument35 pagesThe Management of Diarrhoea in Adults: RCN Guidance For Nursing StaffPopa ElenaNo ratings yet
- 2.a FOOD AND WATERBORNE DISEASES PREVENTION AND CONTROL PROGRAMDocument28 pages2.a FOOD AND WATERBORNE DISEASES PREVENTION AND CONTROL PROGRAMKieth SeresulaNo ratings yet
- Case Clerking Surg Sem 4Document14 pagesCase Clerking Surg Sem 4Selvat ThankamonyNo ratings yet