You might also like
- Living with Metastatic Breast Cancer: Stories of Faith and HopeFrom EverandLiving with Metastatic Breast Cancer: Stories of Faith and HopeNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: Backgroundbehanges71No ratings yet
- Active Surveillance for Localized Prostate Cancer: A New Paradigm for Clinical ManagementFrom EverandActive Surveillance for Localized Prostate Cancer: A New Paradigm for Clinical ManagementNo ratings yet
- Fruits and Vegetables and Cervical Cancer: A Systematic Review and Meta-AnalysisDocument14 pagesFruits and Vegetables and Cervical Cancer: A Systematic Review and Meta-AnalysisSf AkhadiyatiNo ratings yet
- Current Status of Knowledge, Attitude and Practice (KAP) and Screening For Cervical Cancer in Countries at Different Levels of DevelopmentDocument7 pagesCurrent Status of Knowledge, Attitude and Practice (KAP) and Screening For Cervical Cancer in Countries at Different Levels of DevelopmentHuzaifa SaeedNo ratings yet
- Risk Factor of Ectopic PregnancyDocument10 pagesRisk Factor of Ectopic PregnancyFebie CareenNo ratings yet
- Efficacy of Vaccination Against HPV Infections To Prevent Cervical Cancer in France: Present Assessment and Pathways To Improve Vaccination PoliciesDocument8 pagesEfficacy of Vaccination Against HPV Infections To Prevent Cervical Cancer in France: Present Assessment and Pathways To Improve Vaccination PoliciesrickyNo ratings yet
- Winer2016 PDFDocument8 pagesWiner2016 PDFAlex AdamiteiNo ratings yet
- Abnormal Cervical Cytology in Women Eligible For IVFDocument5 pagesAbnormal Cervical Cytology in Women Eligible For IVFtavo823No ratings yet
- Epidemio - Clinical Profile and Management of Female Infertility in The City of IsiroDocument5 pagesEpidemio - Clinical Profile and Management of Female Infertility in The City of IsiroInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breast Cancer in Young WomenFrom EverandBreast Cancer in Young WomenOreste GentiliniNo ratings yet
- Care Pathway of Women With Interval Breast Cancer in 2016 - 2022 - Clinical BreaDocument9 pagesCare Pathway of Women With Interval Breast Cancer in 2016 - 2022 - Clinical BreaAd AdrianaNo ratings yet
- Epidemiological Profile of Gynecologic Breast Cancer inDocument3 pagesEpidemiological Profile of Gynecologic Breast Cancer indomi kalondaNo ratings yet
- Evidence-Based, Alternative Cervical Cancer Screening Approaches in Low-Resource SettingsDocument6 pagesEvidence-Based, Alternative Cervical Cancer Screening Approaches in Low-Resource Settingschica_asNo ratings yet
- 43 FullDocument9 pages43 Fullnayeta levi syahdanaNo ratings yet
- Induced Abortion: ESHRE Capri Workshop GroupDocument10 pagesInduced Abortion: ESHRE Capri Workshop GroupKepa NeritaNo ratings yet
- Risk Factors For Ectopic Pregnancy: A Comprehensive Analysis Based On A Large Case-Control, Population-Based Study in FranceDocument10 pagesRisk Factors For Ectopic Pregnancy: A Comprehensive Analysis Based On A Large Case-Control, Population-Based Study in FranceAreef EymanNo ratings yet
- Upper Tract Urothelial CarcinomaFrom EverandUpper Tract Urothelial CarcinomaShahrokh F. ShariatNo ratings yet
- Cancer Entangled: Anticipation, Acceleration, and the Danish StateFrom EverandCancer Entangled: Anticipation, Acceleration, and the Danish StateRikke Sand AndersenNo ratings yet
- UKPMC Funders Group: Author ManuscriptDocument9 pagesUKPMC Funders Group: Author ManuscriptNikita BowmanNo ratings yet
- Fabian Ashley - Evaluating Secondary Cancer Prevention and The Role of NursesDocument10 pagesFabian Ashley - Evaluating Secondary Cancer Prevention and The Role of Nursesapi-662856597No ratings yet
- Artigo - 22-05Document9 pagesArtigo - 22-05Lu GaldinoNo ratings yet
- A Major Issue in MedicineDocument29 pagesA Major Issue in MedicineSiti NajwaNo ratings yet
- Endometriosis Pathogenesis, Clinical Impact and Management: Volume 9: Frontiers in Gynecological EndocrinologyFrom EverandEndometriosis Pathogenesis, Clinical Impact and Management: Volume 9: Frontiers in Gynecological EndocrinologyNo ratings yet
- The Risk Factors For Cervical Cytological Abnormalities Among Women Infected With Non-16/18 High-Risk Human Papillomavirus: Cross-Sectional StudyDocument14 pagesThe Risk Factors For Cervical Cytological Abnormalities Among Women Infected With Non-16/18 High-Risk Human Papillomavirus: Cross-Sectional StudyAli HNo ratings yet
- 503 837 1 PBDocument14 pages503 837 1 PB5m7m2c2kryNo ratings yet
- 10 1097@aog 0000000000001708Document20 pages10 1097@aog 0000000000001708oodarkfireooNo ratings yet
- Pap IntroductionDocument390 pagesPap IntroductionAnish VeettiyankalNo ratings yet
- International Journal of Africa Nursing Sciences: A A A B A ADocument7 pagesInternational Journal of Africa Nursing Sciences: A A A B A Ayuliaindahp18No ratings yet
- Simanjuntak, 2023Document8 pagesSimanjuntak, 2023Ivo TrisnaNo ratings yet
- ACOG Cervical Cancer ScreeningDocument20 pagesACOG Cervical Cancer ScreeningAlan Ahlawat SumskiNo ratings yet
- Female Sterility and Her Paraclinical Care in Lubumbashi Inventory From 1998 To 2001Document5 pagesFemale Sterility and Her Paraclinical Care in Lubumbashi Inventory From 1998 To 2001International Journal of Innovative Science and Research TechnologyNo ratings yet
- Final Round Case PDFDocument20 pagesFinal Round Case PDFTahiratul ElmaNo ratings yet
- Thesis Cervical CancerDocument6 pagesThesis Cervical Cancerheduurief100% (2)
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)Document18 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)subiNo ratings yet
- Epidemiology Research Paper TopicsDocument5 pagesEpidemiology Research Paper Topicsfemeowplg100% (1)
- Research Paper EpidemiologyDocument9 pagesResearch Paper Epidemiologygw060qpy100% (1)
- Estimating The Prevalence of Obstetric Fistula - A Systematic Review and Meta-Analysis - BMC Pregnancy and Childbirth - Full TextDocument33 pagesEstimating The Prevalence of Obstetric Fistula - A Systematic Review and Meta-Analysis - BMC Pregnancy and Childbirth - Full TextAli AlyousfeNo ratings yet
- Bullet Point CANCER CervicouterinoDocument20 pagesBullet Point CANCER CervicouterinoDaniela DuránNo ratings yet
- ACCP Cxca Screening 2011Document8 pagesACCP Cxca Screening 2011Lizeth López LeónNo ratings yet
- 38565-Article Text-106129-3-10-20200930Document5 pages38565-Article Text-106129-3-10-20200930kirito azumaNo ratings yet
- Pamj 22 26Document8 pagesPamj 22 26Yosie Yulanda PutraNo ratings yet
- Waggoner 2003Document9 pagesWaggoner 2003behanges71No ratings yet
- Cervical Cancer Screening With Human Papillomavirus DNA and Cytology in JapanDocument7 pagesCervical Cancer Screening With Human Papillomavirus DNA and Cytology in Japandella kharisma putriNo ratings yet
- 11 - Trichomonas, Candida, and Gardnerella in CervicalDocument6 pages11 - Trichomonas, Candida, and Gardnerella in CervicalRenan RodriguesNo ratings yet
- Cervical CA Proposal Jan152010Document21 pagesCervical CA Proposal Jan152010redblade_88100% (2)
- Articles: BackgroundDocument10 pagesArticles: BackgroundInryuu ZenNo ratings yet
- Koko's Project 2 Submitted WorkDocument50 pagesKoko's Project 2 Submitted WorkNlemorusa PaschalineNo ratings yet
- CA3 Ginsburg2016 The Global Burden of Women's Cancers A Grand Challenge in Global HealthDocument14 pagesCA3 Ginsburg2016 The Global Burden of Women's Cancers A Grand Challenge in Global Healthalam25No ratings yet
- Full Title: Accuracy of Clinical Breast Examination's AbnormalitiesDocument21 pagesFull Title: Accuracy of Clinical Breast Examination's AbnormalitiesMaria AyaNo ratings yet
- For Personal Use. Only Reproduce With Permission From The LancetDocument10 pagesFor Personal Use. Only Reproduce With Permission From The Lancetzahrah rasyidaNo ratings yet
- HPV Vaccine in Men - Where To?Document10 pagesHPV Vaccine in Men - Where To?RaduAnghelNo ratings yet
- Tatalaksana Dan Pencegahan - Hal 29-38 - Cancer of The Cervix Uteri 2021 UpdateDocument17 pagesTatalaksana Dan Pencegahan - Hal 29-38 - Cancer of The Cervix Uteri 2021 UpdateAl-Amirah ZainabNo ratings yet
- Review Article: Epidemiology and Prognosis of Breast Cancer in Young WomenDocument7 pagesReview Article: Epidemiology and Prognosis of Breast Cancer in Young WomenYudi SupartaNo ratings yet
- Sdarticle 132 PDFDocument1 pageSdarticle 132 PDFRio Michelle CorralesNo ratings yet
- Legal Methods - Course Outline - 2016-17Document4 pagesLegal Methods - Course Outline - 2016-17radhakrishnaNo ratings yet
- UCR Time Series Classification ArchiveDocument14 pagesUCR Time Series Classification ArchivePrithireddy ThenetiNo ratings yet
- Saputri - 2015 - FACTORS INFLUENCING CONSUMER BEHAVIOR TOWARDS MAGNUM ICE CREAMDocument86 pagesSaputri - 2015 - FACTORS INFLUENCING CONSUMER BEHAVIOR TOWARDS MAGNUM ICE CREAMbintang kelanaNo ratings yet
- Free Distribution or Cost Sharing? Evidence From A Randomized Malaria Experiment - Jessica Cohen and Pascaline DupasDocument45 pagesFree Distribution or Cost Sharing? Evidence From A Randomized Malaria Experiment - Jessica Cohen and Pascaline DupassdfzdvgzdfbzdfNo ratings yet
- Jurnal Mengenai Alat Pemotong DahanDocument10 pagesJurnal Mengenai Alat Pemotong DahanSyifa AwaliaNo ratings yet
- CSEC SBA Social StudiesDocument19 pagesCSEC SBA Social StudiesElizabeth Prince76% (17)
- Wheelan 14e ch01Document41 pagesWheelan 14e ch01mostafaragab1983No ratings yet
- Project 3 Paper Mindfulness in Canadian Students. Hurst Desrosiers Dr. Dusic Dr. MilutinovicDocument22 pagesProject 3 Paper Mindfulness in Canadian Students. Hurst Desrosiers Dr. Dusic Dr. MilutinovicMaristela Luman-agNo ratings yet
- Mim 2016Document9 pagesMim 2016Muhammad SyiraziNo ratings yet
- Architectural Design Concept and Guidelines For Floating Structures For Tackling Sea Level Rise Impacts On Abu-QirDocument12 pagesArchitectural Design Concept and Guidelines For Floating Structures For Tackling Sea Level Rise Impacts On Abu-QirNiveditha NivesNo ratings yet
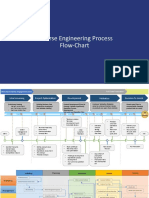
- Reverse Engineering Process Flow ChartDocument3 pagesReverse Engineering Process Flow Chartpradeep k100% (1)
- 2019 HPTLC Association - Marcel Hug - PR HPTLC AssociationDocument13 pages2019 HPTLC Association - Marcel Hug - PR HPTLC AssociationRifanNo ratings yet
- Education Loan BlackbookDocument16 pagesEducation Loan BlackbookSachinSums50% (2)
- Explains Critical Reading As ReasoningDocument19 pagesExplains Critical Reading As ReasoningGianne GuiasNo ratings yet
- Jamiajournalofeducation Vol3 n2 2017march PDFDocument204 pagesJamiajournalofeducation Vol3 n2 2017march PDFAjit MondalNo ratings yet
- Beat The Bourgeoisie - A Social Class Inequality and Mobility Simulation GameDocument12 pagesBeat The Bourgeoisie - A Social Class Inequality and Mobility Simulation GameBig AllanNo ratings yet
- Table of Contents Purposive CommunicationDocument4 pagesTable of Contents Purposive CommunicationFrances Jay FerrerNo ratings yet
- Eysenck Personality Inventory PDFDocument2 pagesEysenck Personality Inventory PDFSean0% (1)
- Dionyssopoulou-Stafylakis 1-16Document16 pagesDionyssopoulou-Stafylakis 1-16Yetaseb SeyoumNo ratings yet
- 3 III Final Final FormatDocument36 pages3 III Final Final FormatMaca UyagNo ratings yet
- Civilian Trail Under Law of Armed ForcesDocument99 pagesCivilian Trail Under Law of Armed Forcesjusnrem aINo ratings yet
- Literature Review On BseDocument7 pagesLiterature Review On Bseafmzfxfaalkjcj100% (1)
- Extended Abstract DelfinoJeconiahDjaja-FhilipYanus CS Nas2023.Docx (Old)Document2 pagesExtended Abstract DelfinoJeconiahDjaja-FhilipYanus CS Nas2023.Docx (Old)Fhilip KnowsNo ratings yet
- The Interaction of Filipino Time and Informal Power Dynamics in The University of The Philippines School of Economics - A Case Study PDFDocument20 pagesThe Interaction of Filipino Time and Informal Power Dynamics in The University of The Philippines School of Economics - A Case Study PDFRafael JohnNo ratings yet
- Perceptions of Social Media Impact On Students Social Behavior A Comparison Between Arts and Science StudentsDocument10 pagesPerceptions of Social Media Impact On Students Social Behavior A Comparison Between Arts and Science StudentsMiaochiiNo ratings yet
- Thesis of Customer Satisfaction in Fast FoodDocument6 pagesThesis of Customer Satisfaction in Fast Foodadrianawilsonpaterson100% (2)
- Sample Thesis Title For Criminology StudentsDocument5 pagesSample Thesis Title For Criminology StudentsPaperWritingServicesReviewsUK100% (2)
- Var WWW Dwpub - Com Htdocs Docs Whitepapers DWPub Public Relations Whitepaper12 An Intro To Social Media MonitoringDocument7 pagesVar WWW Dwpub - Com Htdocs Docs Whitepapers DWPub Public Relations Whitepaper12 An Intro To Social Media MonitoringglasnividNo ratings yet
- Engineering Statistics Handbook 4. Process ModelingDocument60 pagesEngineering Statistics Handbook 4. Process Modelingagbas20026896No ratings yet
- Mtelp Samples l2Document6 pagesMtelp Samples l2bubu_18No ratings yet