You might also like
- Oxygen TherapyDocument71 pagesOxygen TherapyJulia Rose Lee100% (1)
- Echocardiographic Anatomy in The FetusDocument14 pagesEchocardiographic Anatomy in The FetusAnonymous hOHi6TZTnNo ratings yet
- HerbalsmokeDocument19 pagesHerbalsmokelani100% (1)
- AsbestosDocument4 pagesAsbestoskoketsoNo ratings yet
- Oxygen Therapy: Prepared By: Moza Sulaiman Rashid Al-KaldiDocument31 pagesOxygen Therapy: Prepared By: Moza Sulaiman Rashid Al-Kaldimoza92sNo ratings yet
- Oxygen TherapyDocument74 pagesOxygen TherapyMark Reynie Renz Silva100% (6)
- Oxygen Therapy: by DR Finny Theo, MBBS, (DNB)Document59 pagesOxygen Therapy: by DR Finny Theo, MBBS, (DNB)The Telugu DoctorNo ratings yet
- DNA Mutations: Types, Causes and EffectsDocument28 pagesDNA Mutations: Types, Causes and EffectsCaroline Nguyen100% (1)
- Administration of O2 TherapyDocument36 pagesAdministration of O2 TherapyFatima Ysabelle Marie RuizNo ratings yet
- Oxygen Delivery Systems: Under Guidance of Dr. Shraddha Patel by - Dr. Dhwani PatelDocument68 pagesOxygen Delivery Systems: Under Guidance of Dr. Shraddha Patel by - Dr. Dhwani PatelDeep ShahNo ratings yet
- Head To Toe Assessment (Body Parts)Document16 pagesHead To Toe Assessment (Body Parts)jutah2013No ratings yet
- Oxygen Therapy AdministrationDocument15 pagesOxygen Therapy AdministrationMike Faustino Solangon100% (1)
- Bio 12 Zoology Lab ReviewerDocument12 pagesBio 12 Zoology Lab ReviewerFrettyDavidNo ratings yet
- Respiratory Care Module: Inhalers and Proper TechniqueDocument15 pagesRespiratory Care Module: Inhalers and Proper TechniqueNuruddin MuhamadNo ratings yet
- Manaka TechniqueDocument5 pagesManaka TechniqueKoa Carlos CastroNo ratings yet
- Oxygen Therapy Principles and PracticeDocument34 pagesOxygen Therapy Principles and PracticeMark Anthony AlcantaraNo ratings yet
- Oxygen Therapy Methods and Delivery SystemsDocument25 pagesOxygen Therapy Methods and Delivery Systemskirutheka nithilaaNo ratings yet
- Administration of O2 TherapyDocument36 pagesAdministration of O2 TherapyFatima Ysabelle Marie RuizNo ratings yet
- Food Borne DiseasesDocument29 pagesFood Borne DiseasesDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines67% (6)
- O2 TerapiDocument36 pagesO2 Terapinurulanisa0703No ratings yet
- Fundamentals of NursingDocument5 pagesFundamentals of NursingLance Sta AnaNo ratings yet
- Oxygen AdministrationDocument27 pagesOxygen AdministrationakhilNo ratings yet
- 7-Hypoxia Is A KillerDocument33 pages7-Hypoxia Is A KillerChamindraNo ratings yet
- Oxygen Source and TherapyDocument46 pagesOxygen Source and Therapykuruba mahendraNo ratings yet
- Basics of OxygenDocument78 pagesBasics of OxygenClarisse AcacioNo ratings yet
- Inbound 7669742920615241001Document4 pagesInbound 7669742920615241001Mae Loreen CapuyanNo ratings yet
- Oxygen TherapyDocument35 pagesOxygen Therapylala byuNo ratings yet
- Oxygen Delivery Devices: Dr. HimanshuDocument40 pagesOxygen Delivery Devices: Dr. HimanshusnezaimNo ratings yet
- Ncma113 Lec & Lab From Dash 10 - Summer Final 2021: Oxygen TherapyDocument12 pagesNcma113 Lec & Lab From Dash 10 - Summer Final 2021: Oxygen TherapyAliyah Julianne PayumoNo ratings yet
- Case Study AssigmentDocument8 pagesCase Study AssigmentArvin LabradaNo ratings yet
- Infant Feeding Tube: Paediatric Department Nepalese Army Institute of Health SciencesDocument32 pagesInfant Feeding Tube: Paediatric Department Nepalese Army Institute of Health Sciencesmac.rupakhetiNo ratings yet
- Oxygen TherapyDocument41 pagesOxygen TherapyYOGAKRISHNANNo ratings yet
- O2 Presentation2Document28 pagesO2 Presentation2Sangeetha KarunanithiNo ratings yet
- O2 PDFDocument74 pagesO2 PDFsaranya amuNo ratings yet
- MS LAB Oxygenation Nursing SkillsDocument9 pagesMS LAB Oxygenation Nursing SkillsRouwi DesiatcoNo ratings yet
- Critical Care Nursing Guide to Oxygen Therapy and HumidificationDocument73 pagesCritical Care Nursing Guide to Oxygen Therapy and HumidificationChris ZantiraNo ratings yet
- Devices for giving oxygen - How to use and sterilize themDocument51 pagesDevices for giving oxygen - How to use and sterilize themAlok ShuklaNo ratings yet
- Intubation and O2 Basics - Chuko EditDocument34 pagesIntubation and O2 Basics - Chuko EditJon Chuko100% (1)
- MMC OxyDocument13 pagesMMC OxyAira KieNo ratings yet
- Anesthesia Images (All in OnDocument100 pagesAnesthesia Images (All in OnpvsvrNo ratings yet
- Airway Management-Dr RistiawanDocument75 pagesAirway Management-Dr RistiawanjavajavuNo ratings yet
- LECTURE4-Airway Management and Equipment-Dr ManaaDocument68 pagesLECTURE4-Airway Management and Equipment-Dr ManaasnezaimNo ratings yet
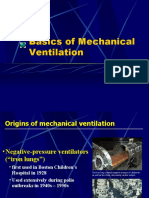
- Basics of Mechanical Ventilation History and SettingsDocument38 pagesBasics of Mechanical Ventilation History and SettingsbennyrolandnababanNo ratings yet
- Bantuan Hidup Dasar Dan Lanjut: BHD-BHLDocument38 pagesBantuan Hidup Dasar Dan Lanjut: BHD-BHLIda Benecia DeseNo ratings yet
- Common Respiratory Interventions GuideDocument5 pagesCommon Respiratory Interventions GuideAngelica Joan SorianoNo ratings yet
- Morbidly Obese Patient: From Fully Supine To Head Elevated Laryngoscopy Postion (H.E.L.P.)Document4 pagesMorbidly Obese Patient: From Fully Supine To Head Elevated Laryngoscopy Postion (H.E.L.P.)Hany ElbarougyNo ratings yet
- Care of Patients Requiring Oxygen Therapy or TracheostomyDocument5 pagesCare of Patients Requiring Oxygen Therapy or TracheostomyAnnie Rose Dorothy MamingNo ratings yet
- Ncma113-Finals Modules SummariesDocument3 pagesNcma113-Finals Modules Summariesroldanmarygrace023No ratings yet
- Funda MidtermsDocument13 pagesFunda MidtermsMutya XDNo ratings yet
- Oxygen concentrator specifications and accessoriesDocument3 pagesOxygen concentrator specifications and accessoriesjamesNo ratings yet
- 00 Anaethesia NotesDocument62 pages00 Anaethesia Notesoe jarmanNo ratings yet
- Oxygen Therapy: Delivery Methods and EquipmentDocument74 pagesOxygen Therapy: Delivery Methods and Equipment3amabelle arevalo100% (2)
- 3 OxygentherapyDocument74 pages3 OxygentherapyHema AnkamreddyNo ratings yet
- ATLS RangkumanDocument162 pagesATLS RangkumanA. Muh. IksanNo ratings yet
- HIGH FLOW NASAL CANNULADocument6 pagesHIGH FLOW NASAL CANNULALord King LlamasNo ratings yet
- Oxygen InhalationDocument26 pagesOxygen InhalationdaisyNo ratings yet
- Techniques of Oxygen DeliveryDocument55 pagesTechniques of Oxygen DeliveryRabi DhakalNo ratings yet
- Airway Management & Ventilation TechniquesDocument13 pagesAirway Management & Ventilation Techniquesmariafer99No ratings yet
- Airway Suctioning (2)Document15 pagesAirway Suctioning (2)Shaira SariaNo ratings yet
- Artificial Airways: Dr. Abhijit Diwate Cardio-Vascular & Respiratory PT DVVPF College of Physiotherapy, Ahmednagar 414111Document40 pagesArtificial Airways: Dr. Abhijit Diwate Cardio-Vascular & Respiratory PT DVVPF College of Physiotherapy, Ahmednagar 414111Mourian AmanNo ratings yet
- Dr. Subhasis Roy: Consultant, Sisu Sanjiban Hospital, Salt Lake, KolkataDocument19 pagesDr. Subhasis Roy: Consultant, Sisu Sanjiban Hospital, Salt Lake, Kolkatacy_alcantaraNo ratings yet
- Managemen Jalan Nafas & Bantuan NafasDocument79 pagesManagemen Jalan Nafas & Bantuan NafasTiara Jauhara AzzahraNo ratings yet
- Group care bundle improves pediatric ICU outcomesDocument12 pagesGroup care bundle improves pediatric ICU outcomesvruttika parmarNo ratings yet
- CH - 3 Airway ManagementDocument45 pagesCH - 3 Airway ManagementHasnat AhmedNo ratings yet
- 1. Basic Airway ManagementDocument56 pages1. Basic Airway ManagementMuhammad Hafiz bin KamaruddinNo ratings yet
- Oxygen TherapyDocument83 pagesOxygen Therapymahmod omerNo ratings yet
- Airway Management: Airway Suctioning Artificial AirwaysDocument25 pagesAirway Management: Airway Suctioning Artificial AirwaysMichelle LindsayNo ratings yet
- Cambridge International AS & A Level: BIOLOGY 9700/21Document20 pagesCambridge International AS & A Level: BIOLOGY 9700/21jamalNo ratings yet
- Chest Pneumonia Detection From X-Ray Images Using Resnet101 ModelDocument19 pagesChest Pneumonia Detection From X-Ray Images Using Resnet101 ModelMahesh TekiNo ratings yet
- Single-Cell Map of Diverse Immune Phenotypes in The Breast Tumor MicroenvironmentDocument53 pagesSingle-Cell Map of Diverse Immune Phenotypes in The Breast Tumor MicroenvironmentRoger FigueiredoNo ratings yet
- Healing Through Loss and GriefDocument3 pagesHealing Through Loss and Griefjackieob123No ratings yet
- Example of Delivery NoteDocument1 pageExample of Delivery NoteRuDy RaviNo ratings yet
- Significance of Study-Denguesummer2012Document2 pagesSignificance of Study-Denguesummer2012Mark Remuel Cruz FinezNo ratings yet
- Endoscopic Retrograde CholangiopancreatographyDocument7 pagesEndoscopic Retrograde CholangiopancreatographyMat JawiNo ratings yet
- 2007 4328b1 02 PrestwickDocument149 pages2007 4328b1 02 PrestwickComunidad Cetram100% (1)
- Scoliosis Clinical & ExerciseDocument14 pagesScoliosis Clinical & ExercisePurohit_RNo ratings yet
- Sample Test Funda Death & DyingDocument1 pageSample Test Funda Death & DyingDanna Kim AuxteroNo ratings yet
- Jib Achha Applied Preventive Vet MedicineDocument2 pagesJib Achha Applied Preventive Vet MedicineAweke EngdaworkNo ratings yet
- Acute Abdomen CausesDocument5 pagesAcute Abdomen CausesSheetal DherangeNo ratings yet
- CDC 2017 0019 0010 - ContentDocument156 pagesCDC 2017 0019 0010 - ContentTrey Martin-EllisNo ratings yet
- Symptoms of Flu: Share On PinterestDocument4 pagesSymptoms of Flu: Share On Pinterestdinesh11rNo ratings yet
- June 2008 Rural Women Magazine, New ZealandDocument8 pagesJune 2008 Rural Women Magazine, New ZealandRural Women New ZealandNo ratings yet
- Session 5 - Performing Cardiovascular System ExaminationDocument22 pagesSession 5 - Performing Cardiovascular System ExaminationOtsward OwdenNo ratings yet
- Pulmonary Rehabilitation (S)Document79 pagesPulmonary Rehabilitation (S)liz100% (3)
- ReferencesDocument6 pagesReferencesAndrew MakariosNo ratings yet
- Journal Club: DR Meera Nandan 3 Year MD ClinicalyogaDocument54 pagesJournal Club: DR Meera Nandan 3 Year MD ClinicalyogaMeera NandanNo ratings yet
- Alien TechnologyDocument11 pagesAlien TechnologySharvari TaklikarNo ratings yet
- Bennett2007 PDFDocument8 pagesBennett2007 PDFMirza RisqaNo ratings yet
- Kinesiology Course WorkDocument8 pagesKinesiology Course Workvepybakek1t3100% (2)