You might also like
- Advanced Airway Management 4th YearsDocument39 pagesAdvanced Airway Management 4th YearsAmmaarah Isaacs100% (1)
- Fundamentals of NursingDocument5 pagesFundamentals of NursingLance Sta AnaNo ratings yet
- Farly Ihsan, S.Kep, .Ners Seminar - 28.06.2020 - International - Initial Assesment - Tangerang WEBINAR 28062020Document55 pagesFarly Ihsan, S.Kep, .Ners Seminar - 28.06.2020 - International - Initial Assesment - Tangerang WEBINAR 28062020Endang CandraNo ratings yet
- Anaesthetic Crisis Handbook PDFDocument44 pagesAnaesthetic Crisis Handbook PDFLouwis Perez100% (1)
- Bantuan Hidup Dasar Dan Lanjut: BHD-BHLDocument38 pagesBantuan Hidup Dasar Dan Lanjut: BHD-BHLIda Benecia DeseNo ratings yet
- NZ Crisis Handbook - EmergenciesDocument28 pagesNZ Crisis Handbook - EmergenciesSean SmythNo ratings yet
- Fundamentals of NursingDocument13 pagesFundamentals of NursingGiselle Chloe Baluya icoNo ratings yet
- Airway ManagementDocument25 pagesAirway ManagementmaithamNo ratings yet
- Anesthesia PocketDocument10 pagesAnesthesia Pocketnebrasothman977No ratings yet
- Luka BakarDocument30 pagesLuka BakarAkmal Sillivan Sods100% (1)
- Foreign BobyDocument29 pagesForeign BobyAbhilasha Singh PanwarNo ratings yet
- Neonatal Resuscitation: Dr. (Col) C.G.Wilson Professor& H.O.D (Paed)Document38 pagesNeonatal Resuscitation: Dr. (Col) C.G.Wilson Professor& H.O.D (Paed)shaharuddin_yahayaNo ratings yet
- Approach To Trauma PatientDocument49 pagesApproach To Trauma PatientHadinur Jufri100% (1)
- Case - ViedyaDocument40 pagesCase - ViedyaRaka WibisonoNo ratings yet
- Preop Conference AnesthesiaDocument33 pagesPreop Conference AnesthesiaBhi-An BatobalonosNo ratings yet
- AnesthesiaDocument56 pagesAnesthesiamahesh naniNo ratings yet
- Airway in Critical Care For GP RSUIDocument29 pagesAirway in Critical Care For GP RSUISeptiana Rizki FauziahNo ratings yet
- TMP 15Document38 pagesTMP 15FrontiersNo ratings yet
- DefinisiDocument8 pagesDefinisichriz murtNo ratings yet
- Difficult Airway ManagementDocument79 pagesDifficult Airway Managementedwardjohnson2310No ratings yet
- DevicesDocument36 pagesDevicesKUMUTHA MALAR A/P PARMESWARANNo ratings yet
- Airway Management in Emergency SituationsDocument29 pagesAirway Management in Emergency SituationsChi MutiaNo ratings yet
- Managemen Jalan Nafas & Bantuan NafasDocument79 pagesManagemen Jalan Nafas & Bantuan NafasTiara Jauhara AzzahraNo ratings yet
- CVAD For NursesDocument54 pagesCVAD For NursesRitaLakhaniNo ratings yet
- Dasar-Dasar Luka Bakar, Skin: Graft, Dan CleftDocument54 pagesDasar-Dasar Luka Bakar, Skin: Graft, Dan CleftM. R. EmeraldNo ratings yet
- RAPID SEQUENCE INTUBATION TECHNIQUEDocument16 pagesRAPID SEQUENCE INTUBATION TECHNIQUEAce ENo ratings yet
- Urologic Laparoscopic Procedures Update: Aly M. Abdel-Karim, MDDocument68 pagesUrologic Laparoscopic Procedures Update: Aly M. Abdel-Karim, MDkhaleeltahaNo ratings yet
- Endotracheal Intubation: A Step-by-Step GuideDocument28 pagesEndotracheal Intubation: A Step-by-Step Guidejeevan ghimireNo ratings yet
- Practical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingDocument24 pagesPractical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingyusNo ratings yet
- Laporan Kegiatan Magang MahasiswaDocument47 pagesLaporan Kegiatan Magang MahasiswaHana Amalia VirantiNo ratings yet
- Anesthesia Images (All in OnDocument100 pagesAnesthesia Images (All in OnpvsvrNo ratings yet
- Anestesi Pada Operasi Mata by PikalDocument60 pagesAnestesi Pada Operasi Mata by PikalSyahpikal SahanaNo ratings yet
- Rapid Sequence IntubationDocument60 pagesRapid Sequence IntubationFlighterdoc100% (1)
- The Occasional Intubator: by DR Minh Le Cong RFDS Cairns, April 2011Document55 pagesThe Occasional Intubator: by DR Minh Le Cong RFDS Cairns, April 2011carlodapNo ratings yet
- Terapi Oxygen Pada Pasien Covd-19Document24 pagesTerapi Oxygen Pada Pasien Covd-19normamNo ratings yet
- Snake Bite Medical Management (5) - 1Document52 pagesSnake Bite Medical Management (5) - 1Anam Syah100% (1)
- The Difficult Airway Management in Adult Critical Care: 5 May 2014 J MatsheDocument60 pagesThe Difficult Airway Management in Adult Critical Care: 5 May 2014 J MatsheSianipar RomulussNo ratings yet
- 1. Basic Airway ManagementDocument56 pages1. Basic Airway ManagementMuhammad Hafiz bin KamaruddinNo ratings yet
- MEDICAL MANAGEMENT OF POSTPARTUM HAEMORRHAGEDocument21 pagesMEDICAL MANAGEMENT OF POSTPARTUM HAEMORRHAGEFamilia Valdivia VilcaNo ratings yet
- RVT ATLS Review & General Principles in TraumaDocument91 pagesRVT ATLS Review & General Principles in TraumaRifqi NuriyNo ratings yet
- Principles of Laparoscopic Surgery: Dr. S. Hasan HarrisDocument20 pagesPrinciples of Laparoscopic Surgery: Dr. S. Hasan HarrisIbrohim ObidovNo ratings yet
- Crash Cart Emergency DrugsDocument103 pagesCrash Cart Emergency DrugsMarianne Laylo67% (3)
- Chapter 3 Airway Management in Trauma PatientDocument53 pagesChapter 3 Airway Management in Trauma PatientMGCNo ratings yet
- Hysteroscopy Procedure Guide for Diagnosis and TreatmentDocument42 pagesHysteroscopy Procedure Guide for Diagnosis and TreatmentNenqply LeaderNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportPrasad Narangoda100% (1)
- Anesthesia For Laparoscopic Myomectomy (LM)Document25 pagesAnesthesia For Laparoscopic Myomectomy (LM)東廣謀No ratings yet
- Airway Management Techniques and DifficultiesDocument89 pagesAirway Management Techniques and DifficultiesJovian LutfiNo ratings yet
- The CaseDocument33 pagesThe CasemarunxNo ratings yet
- Emergency and Acute Phase in Burns - Afriyanti SandhiDocument45 pagesEmergency and Acute Phase in Burns - Afriyanti SandhiPtunk Ndu PutraNo ratings yet
- Rapid Sequence Ion EditedDocument52 pagesRapid Sequence Ion EditedSurgicalgownNo ratings yet
- Laparoscopic Cholecystectomy Techniques and IndicationsDocument100 pagesLaparoscopic Cholecystectomy Techniques and IndicationsRakshay Kaul100% (1)
- ICU - Luka BakarDocument89 pagesICU - Luka BakarAgnes Ummu Afifah100% (1)
- PolytraumaDocument64 pagesPolytraumaOkkie Mharga SentanaNo ratings yet
- Penilaian Awal Dan Pengelolaan (BHD)Document57 pagesPenilaian Awal Dan Pengelolaan (BHD)Rahma DiniNo ratings yet
- Enls V 4 0 Protocol Avs FinalDocument14 pagesEnls V 4 0 Protocol Avs Finalsucipto suciptoNo ratings yet
- Emergency Department Intubation ChecklisTDocument2 pagesEmergency Department Intubation ChecklisTStacey Woods100% (1)
- Nurc Gastrointestinal Hepatobiliary & Neurological Nursing: Masmunaa Hassan 19 September 2017Document29 pagesNurc Gastrointestinal Hepatobiliary & Neurological Nursing: Masmunaa Hassan 19 September 2017Jakub KubaNo ratings yet
- New Snake EmergencyDocument8 pagesNew Snake EmergencyRoxanneNo ratings yet
- Anaesthesia DFX WorkbookDocument10 pagesAnaesthesia DFX WorkbookSaurav SinghNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Shock 1Document15 pagesShock 1kimberlygeducosornedoNo ratings yet
- Basic Life Support 2020Document69 pagesBasic Life Support 2020vidyashetty007100% (2)
- TriageDocument7 pagesTriageSrishti BajajNo ratings yet
- Airway Management EssentialsDocument11 pagesAirway Management EssentialsCarlos Emmanuel Ramirez SantosNo ratings yet
- Ed Trauma Flow Sheet: Part of The Medical RecordDocument6 pagesEd Trauma Flow Sheet: Part of The Medical RecordsafasayedNo ratings yet
- Pengantar SL CPRDocument19 pagesPengantar SL CPRHana SinurayaNo ratings yet
- Abg Analysis: Presented by Anuja Nair Sy MSC NursingDocument15 pagesAbg Analysis: Presented by Anuja Nair Sy MSC NursingAnuja NairNo ratings yet
- Grelha Avaliação ITLSDocument2 pagesGrelha Avaliação ITLSMargarida ReisNo ratings yet
- 12 SeventhproblemDocument52 pages12 SeventhproblemAlicia TjinNo ratings yet
- CPCRDocument51 pagesCPCRAnushaNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityAlexis HospitalNo ratings yet
- Form Initial AssessmentDocument2 pagesForm Initial Assessmentari andiNo ratings yet
- Finals Act 5Document2 pagesFinals Act 5zoro100 88No ratings yet
- Aninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017Document2 pagesAninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017pelangiNo ratings yet
- CMC Maritime Academy - Chennai MFA-Exit Exam Questions: (Revision JUNE 2021) - 1Document4 pagesCMC Maritime Academy - Chennai MFA-Exit Exam Questions: (Revision JUNE 2021) - 1Meghanath AdkonkarNo ratings yet
- ATLSDocument9 pagesATLSAdi Dharmawan100% (7)
- CPC - Appendicitis (Flowchart)Document1 pageCPC - Appendicitis (Flowchart)Milet NacionalesNo ratings yet
- Abdominal Trauma: James R. Nichols III Michael A. PuskarichDocument17 pagesAbdominal Trauma: James R. Nichols III Michael A. PuskarichfitrilihawaNo ratings yet
- Diagnosis and Treatment of Traumatic Brain InjuryDocument22 pagesDiagnosis and Treatment of Traumatic Brain InjuryAmandaNo ratings yet
- Shepherd CertificateDocument1 pageShepherd Certificateapi-643125012No ratings yet
- CRI 089 PrelimsDocument74 pagesCRI 089 Prelimsdebroah280No ratings yet
- 2019 BLS 1 - Revisi Akhir - PPT - Final DR - APRILDocument34 pages2019 BLS 1 - Revisi Akhir - PPT - Final DR - APRILarga setyo adjiNo ratings yet
- Emergency Dispatch ProtocolDocument17 pagesEmergency Dispatch Protocolmeljamerlan100% (2)
- AirQ3 Brochure 2023Document4 pagesAirQ3 Brochure 2023Deya PrastikaNo ratings yet
- Makalah Basic Life Support CompressDocument22 pagesMakalah Basic Life Support CompressNovia RahmaNo ratings yet
- Trauma Team 2007Document5 pagesTrauma Team 2007Christopher TorresNo ratings yet
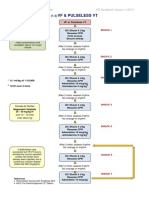
- VF & Pulseless VTDocument1 pageVF & Pulseless VTmadimadi11No ratings yet
- BLS Test PDFDocument76 pagesBLS Test PDFalex rodman50% (2)
- PALS Certification Exam - NHCPS - Com.pdf - Shock (Circulatory) - Cardiopulmonary Resuscitation PDFDocument2 pagesPALS Certification Exam - NHCPS - Com.pdf - Shock (Circulatory) - Cardiopulmonary Resuscitation PDFMarta Delli Carpini Leva100% (1)
- Surgical ICU Exam Content OutlineDocument6 pagesSurgical ICU Exam Content OutlineDarren DawkinsNo ratings yet