Professional Documents
Culture Documents
Pregnancy Outcome in POCS
Uploaded by
Meera Al AliCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pregnancy Outcome in POCS
Uploaded by
Meera Al AliCopyright:
Available Formats
SAAOG Papers www. AJOG.
org
Pregnancy outcomes in women with polycystic
ovary syndrome: a metaanalysis
Lucinda E. Kjerulff, MD; Luis Sanchez-Ramos, MD; Daniel Duffy, MD
OBJECTIVE: The purpose of this study was to examine which maternal tension, preeclampsia, preterm delivery, cesarean delivery, operative
and neonatal complications are associated with polycystic ovary syn- vaginal delivery, SGA, and large-for-gestational age. Only gestational
drome (PCOS) in pregnant women. diabetes mellitus, pregnancy-induced hypertension, preeclampsia,
STUDY DESIGN: The studies that were included compared pregnancy preterm delivery, and SGA infants were found to be statistically
outcomes between women with PCOS and those without diagnosed significant.
PCOS. Our primary outcomes included gestational diabetes mellitus, CONCLUSION: This metaanalysis confirms the higher association of
pregnancy-induced hypertension, and preeclampsia. Secondary out- pregnancy complications and PCOS compared with patients who do not
comes included cesarean delivery rates, operative vaginal delivery have PCOS. Additionally, there may be a stronger association between
rates, preterm delivery, small-for-gestational-age (SGA) infants and PCOS and hypertensive disorders than has been shown previously.
large-for-gestational-age infants.
RESULTS: We found that PCOS in pregnancy was associated with Key words: complication, gestational diabetes mellitus, polycystic
higher rates of gestational diabetes mellitus, pregnancy-induced hyper- ovary syndrome
Cite this article as: Kjerulff LE, Sanchez-Ramos L, Duffy D. Pregnancy outcomes in women with polycystic ovary syndrome: a metaanalysis. Am J Obstet Gynecol
2011;204:558.e1-6.
P olycystic ovary syndrome (PCOS) is
estimated to affect at least 5–15% of
reproductive-aged women and is there-
with menstrual irregularities, decreased
fertility, insulin resistance, diabetes mel-
litus, and hyperandrogenism.2 For this
lated to multiple births.9 Since that
report, 8 relevant studies have been pub-
lished, which includes one that has dis-
fore one of the most common endocrine population to become pregnant, many puted the increased risk of preeclampsia,
abnormalities worldwide.1 Despite its women require assisted reproductive preterm delivery, polyhydramnios, oli-
prevalence, PCOS is a disease with an techniques in addition to the medical gohydramnios, macrosomia, and ad-
unclear cause, varying diagnostic crite- treatment of insulin insensitivity.3-5 verse infant outcomes.10 In view of these
ria, expansive clinical effects, and de- Once this previously subfertile popula- new reports, we conducted an updated
batable management. In nonpregnant tion becomes pregnant, the effect of metaanalysis to reevaluate the risks of
women, PCOS is known to be associated maternal insulin insensitivity and hy- gestational diabetes mellitus, pregnancy-
perandrogenism on the fetus must be induced hypertension, preeclampsia, ce-
considered. sarean delivery, preterm delivery, and
From the Department of Obstetrics and
Pregnant women without PCOS have operative vaginal delivery.
Gynecology, University of Florida College of
a natural state of insulin resistance.6,7
Medicine–Jacksonville, Jacksonville, FL.
With the additive effect of PCOS, this M ATERIALS AND M ETHODS
Presented at the 73rd Annual Meeting of the
South Atlantic Association of Obstetricians and baseline insulin resistance may worsen We reviewed computerized databases,
Gynecologists, Hot Springs, VA, Jan. 30-Feb. and lead to gestational diabetes mel- references of published articles, and text-
2, 2011. litus and its consequences. Additionally, book chapters to find articles that would
Received Oct. 4, 2010; revised Feb. 17, 2011; women with PCOS have been shown to meet the inclusion criteria. Comput-
accepted March 9, 2011. have a low amount of insulin-like growth erized databases included MEDLINE
Reprints: Lucinda Esenam Kjerulff, MD, factor binding globulin-1 that may con- (Pubmed, NLM Gateway) and Cochrane
Resident Physician (PGY3), 653-1 West 8th tribute to preeclampsia and growth ab-
St., Department of Obstetrics and Gynecology, Library.
University of Florida College of
normalities.8 An earlier metaanalysis in
Medicine–Jacksonville, Jacksonville, FL 2006 found that women with PCOS had Study selection
32246. Lucy.Kjerulff@jax.ufl.edu. a significantly higher risk of experiencing To examine the association between
Authorship and contribution to the article is gestational diabetes mellitus, pregnancy- PCOS and pregnancy complications, we
limited to the 3 authors indicated. There was induced hypertension, preeclampsia, searched for studies from 1966 to April
no outside funding or technical assistance with and preterm birth. Additionally, infants 2010 in which outcomes were compared
the production of this article.
of women with PCOS also had a signifi- between women with PCOS and women
0002-9378/$36.00
cantly higher risk of admission to a neo- without diagnosed PCOS. Because most
© 2011 Published by Mosby, Inc.
doi: 10.1016/j.ajog.2011.03.021 natal intensive care unit and a higher of the studies were performed before the
perinatal mortality rate that was unre- revised 2006 Androgen Excess and Poly-
558.e1 American Journal of Obstetrics & Gynecology JUNE 2011
Downloaded for Meera Al Ali (meeali@seha.ae) at Abu Dhabi Health Services Co from ClinicalKey.com by Elsevier on February
27, 2023. For personal use only. No other uses without permission. Copyright ©2023. Elsevier Inc. All rights reserved.
www.AJOG.org SAAOG Papers
cluded cesarean delivery rates, op- abstract. Of the remaining, 37 articles, 14
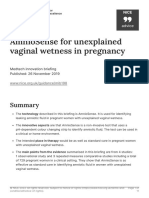
FIGURE
erative vaginal delivery rates, preterm articles were excluded because 4 lacked a
Flowchart of study selection
delivery, small-for-gestational age in- comparison group, 2 did not evaluate the
fants, and large-for-gestational age included outcomes, and 8 involved the
infants. use of metformin after diagnosis of preg-
nancy. The final 23 articles that fully met
inclusion criteria were then reviewed,
Tabulation and integration and data tables were constructed. A total
This systematic review was preceded by a of 92,392 patients were included in the
detailed study protocol that stated the metaanalysis (2544 patients with PCOS
question to be addressed, the subgroups compared with 89,848 patients without
of interest, and the methods and criteria PCOS). Table 1 shows the characteristics
to be used for the identification and se- of each study. Women with PCOS were
lection of relevant studies and extraction noted to have higher rates of gestational
and analysis of information. Approval diabetes mellitus (odds ratio [OR], 2.82;
from the institutional review board 95% confidence interval [CI], 1.93–
was not required to perform this meta- 4.10), pregnancy-induced hypertension
analysis. With the use of computerized (OR, 4.07; 95% CI, 2.75– 6.02), pre-
databases, references of published sys- eclampsia (OR, 4.23; 95% CI, 2.77–
tematic reviews, and textbook chap- 6.46), preterm delivery (OR, 2.20; 95%
ters, potential articles were found and CI, 1.59 –3.04), cesarean delivery (OR,
reviewed.9,12 Search terms included 1.41; 95% CI, 0.96 –2.07), operative vag-
PCOS and pregnancy complications, inal delivery (OR, 1.56; 95% CI, 0.93–
PCOS and pregnancy outcomes, PCOS 2.63), small-for-gestational-age infants
and neonatal outcomes, PCOS and (OR, 2.62; 95% CI, 1.35–5.10), and
gestational diabetes mellitus, PCOS large-for-gestational-age infants (OR,
Kjerulff. Pregnancy outcomes and polycystic ovary and pregnancy and hypertension, 1.56; 95% CI, 0.92–2.64). Table 2 sum-
syndrome. Am J Obstet Gynecol 2011.
PCOS and preeclampsia, PCOS and marizes these results. Tables 3-5 specifi-
preterm labor, PCOS and cesarean sec- cally outline the odds ratio for the
tion delivery, PCOS and operative vag- primary outcomes. All pregnancy out-
cystic Ovary Syndrome (AE-PCOS) So- inal delivery, PCOS and forceps, and comes, except for gestational diabetes
ciety criteria, the 2003 Rotterdam crite- PCOS and vacuum delivery. mellitus, were evaluated with the use of a
ria were used to establish the diagnosis of Articles that were included for full re- fixed-effects model in which the ran-
PCOS. Specifically, the Rotterdam crite- view required the following information: dom-effects model was used. We used
ria require at least 2 of 3 features of (1) assessment of obstetric outcomes in Stata software (version11.0; StataCorp,
PCOS: (1) oligomenorrhea and/or an- women with PCOS that had been diag- College Station, TX) to perform the
ovulation, (2) clinical and/or biochemi- nosed by the Rotterdam criteria or the metaanalysis.
cal signs of hyperandrogenism, (3) poly- updated 2006 AE-PCOS criteria, (2)
cystic ovaries on ultrasound scanning.2 assessment of obstetric outcomes in
The revised 2006 AE-PCOS criteria ex- women without PCOS, and (3) met- C OMMENT
cluded patients who were not hyperan- formin could not have been used by the This metaanalysis confirms earlier find-
drogenic with only oligo/anovulation PCOS group after conception. We fol- ings regarding obstetrics patients with
and polycystic ovaries on ultrasound lowed the Meta-analysis of Observa- PCOS and also updates ORs for associ-
scanning from the diagnosis of PCOS tional Studies in Epidemiology group ated pregnancy complications. Although
but included the other phenotypes of guidelines for analyzing observational women with PCOS were noted to have
PCOS that had been determined by the studies in a metaanalysis.13 Two contrib- higher rates of previously mentioned
Rotterdam consensus.11 Because the utors independently assessed each arti- outcomes, only gestational diabetes
2006 AE-PCOS criteria are inherently cle, and any discrepancies were discussed mellitus, pregnancy-induced hyperten-
within the definition of the Rotterdam with 1 of 2 other contributors. sion, preeclampsia, preterm delivery,
criteria, these updated criteria were and small-for-gestational-age infants
used as an acceptable alternative to use R ESULTS were found to be statistically significant.
to diagnose PCOS in the more current Initial broad search results yielded 946 Furthermore, when compared with the
articles. Our primary outcomes in- possible articles (Figure). Later, 897 arti- 2006 study, the ORs increased for preg-
cluded gestational diabetes mellitus, cles were excluded because of duplica- nancy-induced hypertension, pre-
pregnancy-induced hypertension, and tion or irrelevance by title; then 12 arti- eclampsia, preterm delivery, and small-
preeclampsia. Secondary outcomes in- cles were excluded on the basis of the for-gestational-age infants (Table 6).
JUNE 2011 American Journal of Obstetrics & Gynecology 558.e2
Downloaded for Meera Al Ali (meeali@seha.ae) at Abu Dhabi Health Services Co from ClinicalKey.com by Elsevier on February
27, 2023. For personal use only. No other uses without permission. Copyright ©2023. Elsevier Inc. All rights reserved.
SAAOG Papers www.AJOG.org
TABLE 1
Characteristics of included studies
Group, n
Women with
polycystic ovary Control
Study Outcomes included syndrome patients Conception method Study type
Altieri et al14 GDM, PIH, preeclampsia, cesarean 15 159 Spontaneous, ovulation Retrospective
delivery, OVD, PTD, neonatal induction, ART
malformation
................................................................................................................................................................................................................................................................................................................................................................................
15
Hu et al PIH, preeclampsia 22 22 Spontaneous Prospective
................................................................................................................................................................................................................................................................................................................................................................................
16
Li et al Preeclampsia, PTD, macrosomia, 34 70 Spontaneous and ART Prospective
LGA, SGA
................................................................................................................................................................................................................................................................................................................................................................................
17
Maliqueo et al LGA, SGA 30 34 Spontaneous Prospective
................................................................................................................................................................................................................................................................................................................................................................................
18
Palomba et al GDM, PIH, preeclampsia, cesarean 93 69 Spontaneous Prospective
delivery, OVD, PTD, LGA, SGA,
placental abruption
................................................................................................................................................................................................................................................................................................................................................................................
19
Diamant et al Preeclampsia 70 71 Ovulation induction Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
20
Levran et al GDM 76 95 Spontaneous, ovulation induction Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
21
Wortsman et al GDM 53 2306 Spontaneous, ovulation induction Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
22
Cardenas et al GDM 31 78 Ovulation induction Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
23
Urman et al GDM, PIH, preeclampsia, PTD, NICU 47 100 Spontaneous, ovulation Retrospective
admission induction, ART
................................................................................................................................................................................................................................................................................................................................................................................
24
Fridstrom et al GDM, PIH, preeclampsia 33 66 Spontaneous, ovulation Retrospective
induction, ART
................................................................................................................................................................................................................................................................................................................................................................................
25
Radon et al GDM, preeclampsia 22 66 Spontaneous, ovulation Retrospective
induction, ART
................................................................................................................................................................................................................................................................................................................................................................................
Kashyap and PIH 22 27 Spontaneous, ovulation Retrospective
Claman26 induction, ART
................................................................................................................................................................................................................................................................................................................................................................................
27
Vollenhoven et al GDM, PIH, PTD 60 60 Spontaneous, ovulation induction Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
28
Mikola et al GDM, PIH, PTD 80 712 Ovulation induction Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
29
Bjercke et al GDM, PIH, preeclampsia, cesarean 52 335 Ovulation induction, ART Prospective
delivery, OVD, PTD, NICU admission
................................................................................................................................................................................................................................................................................................................................................................................
30
Haakova et al GDM, PIH, cesarean delivery, PTD 66 66 Spontaneous, unspecified ART Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
31
Turhan et al GDM, PIH, preeclampsia, cesarean 38 136 Not stated Retrospective
delivery, PTD, macrosomia,
neonatal malformation, abruption
................................................................................................................................................................................................................................................................................................................................................................................
32
Weerakiet et al GDM, PIH, preeclampsia, PTD 39 219 Spontaneous, ovulation Prospective
induction, ART
................................................................................................................................................................................................................................................................................................................................................................................
33
Sir-Peterman et al GDM, preeclampsia, PTD, LGA, SGA 47 180 Spontaneous, unspecified ART Prospective
................................................................................................................................................................................................................................................................................................................................................................................
34
Lesser and Garcia GDM 24 44 Unspecified ART Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
35
Lo et al GDM 1542 84882 Not stated Retrospective
................................................................................................................................................................................................................................................................................................................................................................................
36
Sir-Peterman et al GDM, PIH 48 51 Not stated Prospective
................................................................................................................................................................................................................................................................................................................................................................................
ART, assisted reproductive technique; GDM, gestational diabetes mellitus; LGA, large-for-gestational age; NICU, neonatal intensive care unit; OVD, operative vaginal delivery; PIH, pregnancy-induced
hypertension; PTD, preterm delivery; SGA, small-for-gestational age.
Kjerulff. Pregnancy outcomes and polycystic ovary syndrome. Am J Obstet Gynecol 2011.
This information should encourage tients are screened for these complica- lence and management of pregnancy
practitioners to be vigilant when caring tions, solely based on PCOS diagnosis. complications. As suggested in the 2006
for women with PCOS. Currently, there In addition to establishing causation, AE-PCOS task force report, pheno-
is insufficient evidence to establish cau- we also must investigate how the pheno- typic groups may include (1) full-blown
sation and to support changing how pa- typic variants of PCOS alter the preva- PCOS (hyperandrogenemia, hirsutism,
558.e3 American Journal of Obstetrics & Gynecology JUNE 2011
Downloaded for Meera Al Ali (meeali@seha.ae) at Abu Dhabi Health Services Co from ClinicalKey.com by Elsevier on February
27, 2023. For personal use only. No other uses without permission. Copyright ©2023. Elsevier Inc. All rights reserved.
www.AJOG.org SAAOG Papers
TABLE 2
Summary of results
Group, n
Patients with polycystic Control patients with polycystic Odds ratio
Variable ovary syndrome Total ovary syndrome Total (95% CI)
Gestational diabetes mellitus 340 2385 5263 89,669 2.82 (1.93–4.10)
................................................................................................................................................................................................................................................................................................................................................................................
Pregnancy-induced hypertension 84 521 56 1317 4.07 (2.75–6.02)
................................................................................................................................................................................................................................................................................................................................................................................
Preeclampsia 63 589 57 2228 4.23 (2.77–6.46)
................................................................................................................................................................................................................................................................................................................................................................................
Preterm delivery 76 565 155 2129 2.20 (1.59–3.04)
................................................................................................................................................................................................................................................................................................................................................................................
Cesarean delivery 57 171 201 716 1.41 (0.96–2.07)
................................................................................................................................................................................................................................................................................................................................................................................
Operative vaginal delivery 43 160 62 583 1.56 (0.93–2.63)
................................................................................................................................................................................................................................................................................................................................................................................
Small-for-gestational age 29 204 16 353 2.62 (1.35–5.10
................................................................................................................................................................................................................................................................................................................................................................................
Large-for-gestational age 32 204 44 353 1.56 (0.92–2.64)
................................................................................................................................................................................................................................................................................................................................................................................
CI, confidence interval.
Kjerulff. Pregnancy outcomes and polycystic ovary syndrome. Am J Obstet Gynecol 2011.
oligo-anovulation, and polycystic-ap-
TABLE 3 pearing ovaries), (2) hyperandrogenism
Odds ratio for incidence of gestation diabetes mellitus of women with menstrual irregularities, (3) and/or
with polycystic ovary syndrome and control patients hyperandrogenism without menstrual
irregularities. Palomba et al18 are to date
Group (n/N)
the only investigators that have pub-
Women with lished an assessment in this manner. In
polycystic ovary Control their prospective controlled study that
Study syndrome patients Odds ratio (95% CI)
compared 97 patients with PCOS with 73
Altieri et al14 3/15 6/159 6.38 (1.41–28.72) healthy pregnant subjects, they found an
..............................................................................................................................................................................................................................................
18
Palomba et al 15/93 4/69 3.13 (0.99–9.88)
..............................................................................................................................................................................................................................................
overall increased risk for adverse obstet-
Levran et al 20
15/76 9/95 2.35 (0.97–5.72) ric and neonatal outcome but noted that
..............................................................................................................................................................................................................................................
21 this risk varied according to the different
Wortsman et al 4/53 153/2306 1.15 (0.41–3.22)
..............................................................................................................................................................................................................................................
22
phenotypes. Specifically, the relative risk
Cardenas et al 1/31 1/78 2.57 (0.16–42.37) for adverse obstetric and neonatal out-
..............................................................................................................................................................................................................................................
23
Urman et al 6/47 2/100 7.17 (1.39–37.01) comes were 1.93 (95% CI, 1.12–2.96) for
..............................................................................................................................................................................................................................................
Fridstrom et al 24
1/33 1/66 2.03 (0.12–33.54) full-blown phenotype, 2.23 (95% CI,
..............................................................................................................................................................................................................................................
Radon et al 25
9/22 2/66 22.15 (4.28–114.68)
1.21–3.15) for hyperandrogenic non-
..............................................................................................................................................................................................................................................
27
PCO type, 0.54 (95% CI, 0.09 –1.63)
Vollenhoven et al 13/60 10/60 1.38 (0.55–3.45)
.............................................................................................................................................................................................................................................. for nonhyperandrogenic type, and 0.48
28
Mikola et al 20/99 66/737 2.57 (1.48–4.47) (95% CI, 0.31– 0.78) for ovulatory phe-
..............................................................................................................................................................................................................................................
Bjercke et al 29
4/52 2/355 14.71 (2.62–82.46) notypes. This suggested that patients
..............................................................................................................................................................................................................................................
Haakova et al 30
3/66 8/66 0.36 (0.087–1.36) with PCOS can be further categorized as
..............................................................................................................................................................................................................................................
31
high-risk if they have full-blown PCOS
Turhan et al 1/38 11/136 0.31 (0.038–2.46)
.............................................................................................................................................................................................................................................. or have non-PCO hyperandrogenic phe-
32
Weerakiet et al 8/39 13/219 4.09 (1.57–10.66) notypes.18 Specific risk assessment of
..............................................................................................................................................................................................................................................
33
Sir-Petermann et al 6/47 1/180 26.20 (3.07–223.54) each phenotypic group may help identify
..............................................................................................................................................................................................................................................
Lesser and Garcia 34
4/24 3/44 2.73 (0.56–13.40) patients with high-risk PCOS vs patients
..............................................................................................................................................................................................................................................
35 with low-risk PCOS to improve effi-
Lo et al 221/1542 4970/84,882 2.69 (2.33–3.11)
.............................................................................................................................................................................................................................................. ciency of screening, diagnosis, and
36
Sir-Petermann et al 6/48 1/51 7.14 (0.827–61.71) treatment.
..............................................................................................................................................................................................................................................
TOTAL 340/2385 5263/89,669 2.82 (1.94–4.11) Another classification of PCOS that is
..............................................................................................................................................................................................................................................
Heterogeneity 2 ⫽ 36.19 (degrees of freedom ⫽ 17; P ⫽ .004); estimate of between-study variance Tau-squared ⫽ described frequently is “lean” vs “obese”
0.2369; test of odds ratio ⫽ 1: z ⫽ 5.42; P ⫽ .000. patients with PCOS. The difference of
CI, confidence interval.
Kjerulff. Pregnancy outcomes and polycystic ovary syndrome. Am J Obstet Gynecol 2011.
weight and body mass index between
these 2 phenotypes may be the cause of
JUNE 2011 American Journal of Obstetrics & Gynecology 558.e4
Downloaded for Meera Al Ali (meeali@seha.ae) at Abu Dhabi Health Services Co from ClinicalKey.com by Elsevier on February
27, 2023. For personal use only. No other uses without permission. Copyright ©2023. Elsevier Inc. All rights reserved.
SAAOG Papers www.AJOG.org
the marked heterogeneity that is noted
among the studies the have evaluated TABLE 4
gestational diabetes mellitus. A sub- Odds ratio for incidence of pregnancy-induced hypertension of women
group analysis that compared language with polycystic ovary syndrome and control patients
and date and country of publication did Group (n/N)
not explain the heterogeneity. We at-
Women with
tempted to investigate whether body polycystic ovary Control
mass index would account for this vari- Study syndrome patients Odds ratio (95% CI)
ation, but few studies included patient Altieriat et al14 2/15 10/159 2.29 (0.45–11.59)
..............................................................................................................................................................................................................................................
weight in their data, and even fewer stud- 15
Hu et al 6/22 0/22 17.73 (0.93–337.26)
ies documented body mass index. An in- ..............................................................................................................................................................................................................................................
18
depth metaregression that compared Palomba et al 13/93 3/69 3.58 (0.98–13.08)
..............................................................................................................................................................................................................................................
body mass index and age among women Urman et al 23
12/47 8/100 3.94 (1.49–10.46)
..............................................................................................................................................................................................................................................
with and without PCOS might illumi- Fridstrom et al 24
6/33 3/66 4.67 (1.09–20.04)
..............................................................................................................................................................................................................................................
nate reasons for variability between
Kashyap and 7/22 1/27 12.13 (1.36–108.36)
studies. Claman26
Last, we must examine how the use of ..............................................................................................................................................................................................................................................
27
metformin past the first trimester may Vollenhoven et al 10/44 3/44 4.02 (1.02–15.79)
..............................................................................................................................................................................................................................................
29
decrease pregnancy complications. It is Bjercke et al 6/52 1/355 46.17 (5.44–392.13)
..............................................................................................................................................................................................................................................
already known that PCOS increases the Haakova et al 30
5/66 4/66 1.27 (0.33–4.96)
..............................................................................................................................................................................................................................................
baseline insulin resistance of pregnancy. Turhan et al 31
4/38 9/136 1.66 (0.48–5.72)
Separately, metformin is known to de- ..............................................................................................................................................................................................................................................
32
crease this state of insulin resistance in Weerakiet et al 9/41 14/222 4.18 (1.67–10.45)
..............................................................................................................................................................................................................................................
33
patients with PCOS. Although the use of Sir-Petermann et al 4/48 0/51 10.42 (0.55–198.83)
..............................................................................................................................................................................................................................................
metformin alone or in combination with TOTAL 84/521 56/1317 4.07 (2.75–6.02)
..............................................................................................................................................................................................................................................
clomiphene has not been shown to im- Heterogeneity 2 ⫽ 12.64 (degrees of freedom ⫽ 11; P ⫽ 0.317); test of odds ratio ⫽ 1: z ⫽ 7.03; P ⫽ .000.
prove live birth rates, clinical pregnancy CI, confidence interval.
rates are improved when compared with Kjerulff. Pregnancy outcomes and polycystic ovary syndrome. Am J Obstet Gynecol 2011.
placebo.1 Currently, 3 controlled trials
and 3 observational studies have investi-
gated the prevention of gestational dia- TABLE 5
betes mellitus by continuing metfor- Odds ratio for the incidence of preeclampsia for women
min therapy throughout pregnancy in with polycystic ovary syndrome and control patients
women with PCOS, but the sample sizes Group (n/N)
are small, and the results are conflicting.
Polycystic ovary Control
An initial metaanalysis of the use of met- Study syndrome patients Odds ratio (95% CI)
formin throughout pregnancy was per- 14
Altieri et al 0/15 2/159 2.03 (0.09–44.26)
formed but did not show a statistically ..............................................................................................................................................................................................................................................
16
significant reduction of gestational dia- Li et al 6/34 4/70 3.54 (0.93–13.51)
..............................................................................................................................................................................................................................................
betes mellitus. Palomba et al 18
9/93 1/69 7.29 (0.90–58.94)
..............................................................................................................................................................................................................................................
Inherent to the nature of observa- Diamant et al 19
20/70 3/71 9.07 (2.55–32.20)
tional studies are the main limitations to ..............................................................................................................................................................................................................................................
23
Urman et al 3/47 4/100 1.64 (0.35–7.62)
this study: heterogeneity and lack of pro- ..............................................................................................................................................................................................................................................
24
spective data to establish causation. De- Fridstrom et al 3/33 0/66 15.26 (0.76–304.73)
..............................................................................................................................................................................................................................................
spite its limitation, this study is still Radon et al 25
5/22 1/66 19.12 (2.09–174.70)
..............................................................................................................................................................................................................................................
useful for clinical practice. Physicians Mikola et al 28
4/99 14/737 2.17 (0.70–6.74)
should continue to consider patients ..............................................................................................................................................................................................................................................
29
Bjercke et al 7/52 25/355 2.05 (0.84–5.02)
with PCOS to be high risk and to moni- ..............................................................................................................................................................................................................................................
31
tor them closely for the development of Turhan et al 3/38 2/136 5.74 (0.92–35.71)
..............................................................................................................................................................................................................................................
gestational diabetes mellitus, pregnancy- Weerakiet et al 32
1/39 1/219 5.74 (0.35–93.70)
..............................................................................................................................................................................................................................................
induced hypertension, and preeclamp- Sir-Petermann et al 33
2/47 0/180 19.84 (0.94–420.39)
sia. Hypertensive disorders in PCOS may ..............................................................................................................................................................................................................................................
TOTAL 63/589 57/2228 4.23 (2.77–6.46)
be due to low levels of insulin-like ..............................................................................................................................................................................................................................................
growth factor binding globulin-1 and Heterogeneity 2 ⫽ 10.87 (degrees of freedom ⫽ 11; P ⫽ .454); test of odds ratio ⫽ 1: z ⫽ 6.69; P ⫽ .000.
CI, confidence interval.
therefore may account for the increase in Kjerulff. Pregnancy outcomes and polycystic ovary syndrome. Am J Obstet Gynecol 2011.
pregnancy-induced hypertension and
558.e5 American Journal of Obstetrics & Gynecology JUNE 2011
Downloaded for Meera Al Ali (meeali@seha.ae) at Abu Dhabi Health Services Co from ClinicalKey.com by Elsevier on February
27, 2023. For personal use only. No other uses without permission. Copyright ©2023. Elsevier Inc. All rights reserved.
www.AJOG.org SAAOG Papers
ovary syndrome. J Reprod Med 1991;36:
TABLE 6 659-61.
Comparison of the odds ratios of the current and previous metaanalyses 22. Cardenas M, Coulson CC, Legro RS. Infer-
tile PCOS women do not have an increased risk
Odds ratio (95% CI) for gestational diabetes or macrosomia [ab-
stract]. Hum Reprod Update 2006;12:673-83.
Variable Current study (2010) Boomsma et al5 (2006)
23. Urman B, Sarac E, Dogan L, Gurgan T. Preg-
Pregnancy-induced hypertension 4.07 (2.75–6.02) 3.67 (1.98–6.81) nancy in infertile PCOD patients, complications
..............................................................................................................................................................................................................................................
and outcome. J Reprod Med 1997;42:501-5.
Preeclampsia 4.23 (2.77–6.46) 3.47 (1.95–6.17)
.............................................................................................................................................................................................................................................. 24. Fridstrom M, Nisell H, Sjoblom P, Hillensjo
Preterm delivery 2.20 (1.59–3.04) 1.75 (1.16–2.62) T. Are women with polycystic ovary syndrome
..............................................................................................................................................................................................................................................
at an increased risk of pregnancy-induced hy-
Small-for-gestational age 2.62 (1.35–5.10) 1.16 (0.31–5.12)
.............................................................................................................................................................................................................................................. pertension and/or preeclampsia? Hypertens
CI, confidence interval. Pregnancy 1999;18:73-80.
Kjerulff. Pregnancy outcomes and polycystic ovary syndrome. Am J Obstet Gynecol 2011. 25. Radon PA, McMahon MJ, Meyer WR. Im-
paired glucose tolerance in pregnant women
with polycystic ovary syndrome. Obstet Gyne-
preeclampsia in our study population. diabetes mellitus in women with polycystic col 1999;94:194-7.
ovary syndrome. J Perinat Med 2010 38:141-6. 26. Kashyap S, Claman P. Polycystic ovary dis-
Practitioners should wait for additional
11. Azziz R, Carmina E, Dewailly D, et al. The ease and the risk of pregnancy-induced hyper-
evidence that supports deviation from Androgen Excess and PCOS Society Criteria tension. J Reprod Med 2000;45:991-4.
current screening guidelines. f for the Polycystic Ovary Syndrome: the com- 27. Vollenhoven B, Clark S, Kovacs G, Burger
plete task force report. Fertil Steril 2009; H, Healy D. Prevalence of gestational diabetes
91:456-88. mellitus in polycystic ovarian syndrome (PCOS)
REFERENCES 12. Toulis KA, Goulis DG, Kolibianakis EM, et al. patients pregnant after ovulation induction with
1. Tang T, Lord JM, Norman RJ, Yasmin E, Risk of gestational diabetes mellitus in women gonadotrophins. Aust N Z J Obstet Gynaecol
Balen AH. Insulin-sensitizing drugs (metformin, with polycystic ovary syndrome: a systematic 2000;40:54-8.
rosiglitazone, pioglitazone, D-chiro-inositol) for review and a meta-analysis. Fertil Steril 2009; 28. Mikola M, Hiilesmaa V, Halttunen M,
women with polycystic ovary syndrome, oligo 92:667-77. Suhonen L, Tiitinen A. Obstetric outcome in
amenorrhea and subfertility. Cochrane Data- 13. Stroup DF, Berlin JA, Morton SC, et al. women with polycystic ovarian syndrome. Hum
base Syst Rev 2009:CD003053. Meta-analysis of observational studies in epide- Reprod 2001;16:226-9.
2. American College of Obstetricians and Gyne- miology: a proposal for reporting: Meta-analysis 29. Bjercke S, Dale PO, Tanbo T, Storeng R,
cologists. ACOG practice bulletin no. 108: poly- of Observational Studies in Epidemiology Ertzeid G, Abyholm T. Impact of insulin resistance
cystic ovary syndrome. Obstet Gynecol 2009; (MOOSE) group. JAMA 2000;283:2008-12. on pregnancy complications and outcome in
114:936-49. 14. Altieri P, Gambineri A, Prontera O, et al. Ma- women with polycystic ovary syndrome. Gynecol
3. Azziz R, Ehrmann D, Legro RS, et al. Trogli- ternal polycystic ovary syndrome may be asso- Obstet Invest 2002;54:94-8.
tazone improves ovulation and hirsutism in the ciated with adverse pregnancy outcomes. Eur J 30. Haakova L, Cibula D, Rezabek K, Hill M, Fanta
polycystic ovary syndrome: a multicenter, dou- Obstet Gynecol Reprod Biol 2010;149:31-6. M, Zivny J. Pregnancy outcome in women with
ble-blond, placebo-controlled trial. PCOS/Tro- 15. Hu S, Lenoard A, Seifalian A, Hardiman P. PCOS and in controls matched by age and
glitazone study group. J Clin Endocrinol Metab Vascular dysfunction during pregnancy in weight. Hum Reprod 2003;18:1438-41.
2001;86:1626-32. women with polycystic ovary syndrome. Hum 31. Turhan NO, Seçkin NC, Aybar F, Inegöl I.
4. Lord JM, Flight IH, Norman RJ. Metformin in Reprod 2007;22:1532-9. Assessment of glucose tolerance and preg-
polycystic ovary syndrome: systematic review 16. Li G, Fan L, Zhang L, Zhang W, Huang X. nancy outcome of polycystic ovary patients. Int
and meta-analysis BMJ 2003;327:951-3. Metabolic parameters and perinatal outcomes J Gynaecol Obstet 2003;81:163-8.
5. Heijnen E, Eijkemans M, Hughes E, Laven J, of gestational diabetes in women with polycys- 32. Weerakiet S, Srisombut C, Rojanasakul A,
Macklon N, Fauser B. A meta-analysis of out- tic ovary syndrome. J Perinat Med 2010;38: Panburana P, Thakkinstian A, Herabutya Y.
comes of conventional IVF in women with poly- 141-6. Prevalence of gestational diabetes mellitus and
cystic ovary syndrome. Hum Reprod Update 17. Maliqueo M, Echiburú B, Crisosto N, et al. pregnancy outcomes in Asian women with
2006;12:13-21. Metabolic parameters in cord blood of new- polycystic ovary syndrome. Gynecol Endocrinol
6. Yogev Y, Ben-Haroush A, Chen R, et al. Di- borns of women with polycystic ovary syn- 2004;19:134-40.
urnal glycemic profile in obese and normal drome. Fertil Steril 2009;92:277-82. 33. Sir-Petermann T, Hitchsfeld C, Maliqueo M,
weight nondiabetic pregnant women. Am J Ob- 18. Palomba S, Falbo A, Russo T, Tolino A, Orio et al. Birth weight in offspring of mothers with
stet Gynecol 2004;191:949. F, Zullo F. Pregnancy in women with polycystic polycystic ovarian syndrome. Hum Reprod
7. Ryan E. Hormones and insulin resistance in ovary syndrome: the effect of different pheno- 2005;20:2122-6.
pregnancy. Lancet 2003;362:1777. types and features on obstetric and neonatal 34. Lesser KB, Garcia FA. Association between
8. Jensen RB, Chellakooty M, Vielwerth S, et al. outcomes. Fertil Steril 2010;94:1805-11. polycystic ovary syndrome and glucose intoler-
Intrauterine growth retardation and conse- 19. Diamant YZ, Rimon E, Evron S. High inci- ance during pregnancy. J Matern Fetal Med
quences for endocrine and cardiovascular dis- dence of preeclamptic toxemia in patients with 1997;6:303-7.
ease in adult life: does insulin-like growth fac- polycystic ovarian disease. Eur J Obstet Gyne- 35. Lo JC, Feigenbaum SL, Yang J, Pressman
tor-1 play a role? Horm Res 2003;60(suppl): col Reprod Biol 1982;14:199-204. AR, Selby JV, Go A. Epidemiology and adverse
136-48. 20. Levran JS, Imani B, Eijkemans MJ, Fauser cardiovascular risk profile of diagnosed poly-
9. Boomsma CM, Eijkemans MJC, Huges EG, BC. New approach to polycystic ovary syn- cystic ovary syndrome. J Clin Endocrinol Metab
et al. A meta-analysis of pregnancy outcomes in drome and other forms of anovulatory infertility 2006;91:1357-63.
women with polycystic ovary syndrome. Hum Obstet Gynecol Surv 2002;57:755– 67. 36. Sir-Petermann T, Echiburú B, Maliqueo MM,
Reprod Update 2006;12:673-83. 21. Wortsman J, de Angeles S, Futterweit W, et al. Serum adiponectin and lipid concentrations
10. Li G, Fan L, Zhang L, et al. Metabolic pa- Singh KB, Kaufmann RC. Gestational diabetes in pregnant women with polycystic ovary syn-
rameters and perinatal outcomes of gestational and neonatal macrosomia in the polycystic drome. Hum Reprod 2007;22:1830-6.
JUNE 2011 American Journal of Obstetrics & Gynecology 558.e6
Downloaded for Meera Al Ali (meeali@seha.ae) at Abu Dhabi Health Services Co from ClinicalKey.com by Elsevier on February
27, 2023. For personal use only. No other uses without permission. Copyright ©2023. Elsevier Inc. All rights reserved.
You might also like
- Pregnancy Complications in Women With PCOS: A Meta-Analysis: KM Tanvir and Mohammad Lutfor RahmanDocument6 pagesPregnancy Complications in Women With PCOS: A Meta-Analysis: KM Tanvir and Mohammad Lutfor Rahmanmr1998goNo ratings yet
- The Impact of Fetal Growth Restriction On Latency in The Setting of Expectant Management of PreeclampsiaDocument7 pagesThe Impact of Fetal Growth Restriction On Latency in The Setting of Expectant Management of PreeclampsiagusriaNo ratings yet
- Irv 311Document9 pagesIrv 311Anonymous YyLSRdNo ratings yet
- pdf 2Document21 pagespdf 2agung krisNo ratings yet
- Can Placental Growth Factor in Maternal Circulation Identify Fetuses With Placental Intrauterine Growth RestrictionDocument7 pagesCan Placental Growth Factor in Maternal Circulation Identify Fetuses With Placental Intrauterine Growth RestrictionagusNo ratings yet
- The Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaDocument8 pagesThe Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaAndres GallegosNo ratings yet
- Original Research PaperDocument4 pagesOriginal Research PaperOviya ChitharthanNo ratings yet
- Polycystic Ovary SyndromeDocument6 pagesPolycystic Ovary SyndromealemNo ratings yet
- Laborinduction: Areviewof Currentmethods: Mildred M. RamirezDocument11 pagesLaborinduction: Areviewof Currentmethods: Mildred M. RamirezRolando DiazNo ratings yet
- Effect of Placenta Previa On Fetal Growth: ObstetricsDocument5 pagesEffect of Placenta Previa On Fetal Growth: ObstetricsAnonymous 4OpLzzt6No ratings yet
- Prevalence of Infertility and Use of Fertility Treatment in Women With Polycystic Ovary Syndrome: Data From A Large Community-Based Cohort StudyDocument9 pagesPrevalence of Infertility and Use of Fertility Treatment in Women With Polycystic Ovary Syndrome: Data From A Large Community-Based Cohort Studymnn164No ratings yet
- Jurnal ObsgynDocument11 pagesJurnal ObsgynVivie Tirany SoediroNo ratings yet
- Bjo12636 PDFDocument9 pagesBjo12636 PDFLuphly TaluvtaNo ratings yet
- Articulo EndometriosisDocument7 pagesArticulo EndometriosisMaIt VeFloNo ratings yet
- 10 1016@j Ajog 2019 01 206Document8 pages10 1016@j Ajog 2019 01 206Yusvita WaliaNo ratings yet
- 10 1016@j Ajog 2019 01 206 PDFDocument8 pages10 1016@j Ajog 2019 01 206 PDFYusvita WaliaNo ratings yet
- Exercise During Pregnancy Protects Against Hypertension and Macrosomia: Randomized Clinical TrialDocument8 pagesExercise During Pregnancy Protects Against Hypertension and Macrosomia: Randomized Clinical TrialDaniela VenegasNo ratings yet
- Maternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewDocument23 pagesMaternal, Labor, Delivery, and Perinatal Outcomes Associated With Placental Abruption: A Systematic ReviewasfwegereNo ratings yet
- Neonatal Complications of Term Pregnancy: Rates by Gestational Age Increase in A Continuous, Not Threshold, FashionDocument6 pagesNeonatal Complications of Term Pregnancy: Rates by Gestational Age Increase in A Continuous, Not Threshold, FashionAndreea BorislavschiNo ratings yet
- DownloadDocument6 pagesDownloadKai GgNo ratings yet
- Associated Risk Factors of Placenta Previa A Matched Case Control StudyDocument4 pagesAssociated Risk Factors of Placenta Previa A Matched Case Control StudyFitri Nur DiniNo ratings yet
- Effect of High-Dose Folic Acid Supplementation On The Prevention of Preeclampsia in Twin PregnancyDocument7 pagesEffect of High-Dose Folic Acid Supplementation On The Prevention of Preeclampsia in Twin PregnancyAzmia TabahNo ratings yet
- Good Outcome of Teenage Pregnancies in High-Quality Maternity CareDocument5 pagesGood Outcome of Teenage Pregnancies in High-Quality Maternity CareNabila MomorNo ratings yet
- Herrera 2017Document9 pagesHerrera 2017Bianca Maria PricopNo ratings yet
- 05 N010 260Document13 pages05 N010 260Kinjal VasavaNo ratings yet
- Pregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninDocument5 pagesPregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninMentari SetiawatiNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- Effects of prepregnancy dietary patterns on infant birth weight a prospective cohort studyDocument11 pagesEffects of prepregnancy dietary patterns on infant birth weight a prospective cohort studyLola SantiaNo ratings yet
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyFrom EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyNo ratings yet
- Treatment HEGDocument10 pagesTreatment HEGAnonymous 7jvQWDndVaNo ratings yet
- 10 1111@jog 143436777777Document17 pages10 1111@jog 143436777777Epiphany SonderNo ratings yet
- The Effect of Obesity On Pregnancy and Its Outcome in The Population of Oman, Seeb ProvinceDocument12 pagesThe Effect of Obesity On Pregnancy and Its Outcome in The Population of Oman, Seeb ProvinceHazley ZeeNo ratings yet
- Ultrasound Diagnosis of MacrosomiaDocument4 pagesUltrasound Diagnosis of MacrosomiaIndah 15No ratings yet
- The Prediction of Preeclampsia The Way Forward 20Document14 pagesThe Prediction of Preeclampsia The Way Forward 20Ecaterina Sorto de ArgeñalNo ratings yet
- 1 s2.0 S1110569015300042 MainDocument5 pages1 s2.0 S1110569015300042 MainAzam alausyNo ratings yet
- PCOS Pregnancy RisksDocument26 pagesPCOS Pregnancy RisksPany Chandra LestariNo ratings yet
- Ovario PoliqDocument16 pagesOvario PoliqlizethNo ratings yet
- Articulo 5Document6 pagesArticulo 5Monica ReyesNo ratings yet
- Artigo 3Document7 pagesArtigo 3Cirineu NetoNo ratings yet
- Rethinking IUGR in preeclampsiaDocument5 pagesRethinking IUGR in preeclampsiaAntonius Joko NugrohoNo ratings yet
- Jurnal Placenta PreviaDocument9 pagesJurnal Placenta Previasheva25No ratings yet
- Clinical Study of Infant of Diabetic Mother, Clinical Profile and Immediate Outcome in Peri-Natal PeriodDocument14 pagesClinical Study of Infant of Diabetic Mother, Clinical Profile and Immediate Outcome in Peri-Natal Periodvighnaharta Online ServicesNo ratings yet
- Group 15 Research Paper PcosDocument14 pagesGroup 15 Research Paper Pcosapi-717342251No ratings yet
- Adolescent Preeclampsia: Pathological Drivers and Clinical Prevention StrategiesDocument13 pagesAdolescent Preeclampsia: Pathological Drivers and Clinical Prevention StrategiesEmmanuel Guevara HernándezNo ratings yet
- Maternal Obesity 2Document13 pagesMaternal Obesity 2lalimdNo ratings yet
- Jurnal KedokteranDocument6 pagesJurnal Kedokteranusk.ppdsobgynganjil2022No ratings yet
- Malnutrition Among Pregnant Women Iran StudyDocument8 pagesMalnutrition Among Pregnant Women Iran StudyKimberlyjoycsolomonNo ratings yet
- Jurnal 1Document8 pagesJurnal 1lomba Panah Dies UnsriNo ratings yet
- 33873-Article Text-121761-1-10-20170831Document6 pages33873-Article Text-121761-1-10-20170831AnggaNo ratings yet
- Del 153Document6 pagesDel 153Fan AccountNo ratings yet
- Pre-Existing Diabetes Mellitus and Adverse PDFDocument5 pagesPre-Existing Diabetes Mellitus and Adverse PDFMetebNo ratings yet
- Prevalence of Preeclampsia and The Associated Risk Factors Among Pregnant Women in BangladeshDocument10 pagesPrevalence of Preeclampsia and The Associated Risk Factors Among Pregnant Women in BangladeshNanda Puspita SariNo ratings yet
- Aust NZ J Obst Gynaeco - 2022 - Silveira - Placenta Accreta Spectrum We Can Do BetterDocument7 pagesAust NZ J Obst Gynaeco - 2022 - Silveira - Placenta Accreta Spectrum We Can Do BetterDrFeelgood WolfslandNo ratings yet
- Update On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal MedicineDocument217 pagesUpdate On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal Medicinemeriatmaja100% (1)
- Is Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyDocument6 pagesIs Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyYessie ErNo ratings yet
- Elective Delivery Versus Expectant Management For Pre-Eclampsia: A Meta-Analysis of RctsDocument16 pagesElective Delivery Versus Expectant Management For Pre-Eclampsia: A Meta-Analysis of RctsErliana Damayanti100% (1)
- A Comparison of Maternal End Perinatal Outcomes With Vaginal DeliveryDocument7 pagesA Comparison of Maternal End Perinatal Outcomes With Vaginal DeliveryStéphanieNo ratings yet
- HHS Public Access: The Effects of Aspirin in Gestation and Reproduction (EAGeR) TrialDocument17 pagesHHS Public Access: The Effects of Aspirin in Gestation and Reproduction (EAGeR) TrialAndre PutraNo ratings yet
- Sibai PDFDocument2 pagesSibai PDFAdriana PajueloNo ratings yet
- 114 FullDocument7 pages114 FullAnnette ChavezNo ratings yet
- Diabetes in Pregnancy PDF 75545246042053Document25 pagesDiabetes in Pregnancy PDF 75545246042053Meera Al AliNo ratings yet
- Social and Emotional Wellbeing Early Years PDF 1996351221445Document76 pagesSocial and Emotional Wellbeing Early Years PDF 1996351221445Meera Al AliNo ratings yet
- Ectopic Pregnancy and Miscarriage Diagnosis and Initial Management PDF 66141662244037Document41 pagesEctopic Pregnancy and Miscarriage Diagnosis and Initial Management PDF 66141662244037Meera Al AliNo ratings yet
- Pyelonephritis Acute Antimicrobial Prescribing PDF 66141593379781Document32 pagesPyelonephritis Acute Antimicrobial Prescribing PDF 66141593379781Meera Al AliNo ratings yet
- Postnatal Care PDF 2098611282373Document39 pagesPostnatal Care PDF 2098611282373Meera Al AliNo ratings yet
- Fertility Problems Assessment and Treatment PDF 35109634660549Document53 pagesFertility Problems Assessment and Treatment PDF 35109634660549Meera Al AliNo ratings yet
- Weight Management Before During and After Pregnancy PDF 1996242046405Document56 pagesWeight Management Before During and After Pregnancy PDF 1996242046405Meera Al AliNo ratings yet
- Twin and Triplet Pregnancy PDFDocument67 pagesTwin and Triplet Pregnancy PDFTaufik SaadNo ratings yet
- Urinary Tract Infection Lower Antimicrobial Prescribing PDF 66141546350533Document39 pagesUrinary Tract Infection Lower Antimicrobial Prescribing PDF 66141546350533Andres PerezNo ratings yet
- Obesity Identification Assessment and Management PDF 35109821097925Document64 pagesObesity Identification Assessment and Management PDF 35109821097925Meera Al AliNo ratings yet
- Fetal Monitoring in Labour PDF 66143844065221Document41 pagesFetal Monitoring in Labour PDF 66143844065221Meera Al AliNo ratings yet
- Inducing Labour PDF 66143719773637Document41 pagesInducing Labour PDF 66143719773637Meera Al AliNo ratings yet
- Urinary Tract Infection Recurrent Antimicrobial Prescribing PDF 66141595059397Document39 pagesUrinary Tract Infection Recurrent Antimicrobial Prescribing PDF 66141595059397Meera Al AliNo ratings yet
- Plgfbased Testing To Help Diagnose Suspected Preterm Preeclampsia PDF 1053819586501Document27 pagesPlgfbased Testing To Help Diagnose Suspected Preterm Preeclampsia PDF 1053819586501Meera Al AliNo ratings yet
- Multiple Pregnancy Twin and Triplet Pregnancies PDF 2098670068933Document52 pagesMultiple Pregnancy Twin and Triplet Pregnancies PDF 2098670068933Meera Al AliNo ratings yet
- Hypertension in Pregnancy Diagnosis and Management PDF 66141717671365Document62 pagesHypertension in Pregnancy Diagnosis and Management PDF 66141717671365Meera Al AliNo ratings yet
- Intrapartum Care For Healthy Women and Babies PDF 35109866447557Document80 pagesIntrapartum Care For Healthy Women and Babies PDF 35109866447557Mahmoud AbubakrNo ratings yet
- Amniosense For Unexplained Vaginal Wetness in Pregnancy PDF 2285963765213893Document11 pagesAmniosense For Unexplained Vaginal Wetness in Pregnancy PDF 2285963765213893Meera Al AliNo ratings yet
- Abortion Care PDF 66141773098693Document72 pagesAbortion Care PDF 66141773098693Meera Al AliNo ratings yet
- NICE Neonatal-Infection-Antibiotics-For-Prevention-And-Treatment-Pdf-66142083827653Document60 pagesNICE Neonatal-Infection-Antibiotics-For-Prevention-And-Treatment-Pdf-66142083827653Juan Diego Sandoval RojasNo ratings yet
- Antenatal and Postnatal Mental Health Clinical Management and Service Guidance PDF 35109869806789Document58 pagesAntenatal and Postnatal Mental Health Clinical Management and Service Guidance PDF 35109869806789Meera Al AliNo ratings yet
- Heavy Menstrual Bleeding Assessment and Management PDF 1837701412549Document33 pagesHeavy Menstrual Bleeding Assessment and Management PDF 1837701412549Meera Al AliNo ratings yet
- Personality Trait, Postpartum DepressionDocument13 pagesPersonality Trait, Postpartum DepressionMeera Al AliNo ratings yet
- Gestational DiabetesDocument7 pagesGestational DiabetesQueenie PuzonNo ratings yet
- Postterm Pregnancy Risks & Management OptionsDocument5 pagesPostterm Pregnancy Risks & Management OptionsOmar MohammedNo ratings yet
- Diabetes Acog 2017Document15 pagesDiabetes Acog 2017Holger Vicente Guerrero Guerrero100% (1)
- Post Mature Neonate, Infant of Diabetic and Substance Abuse MotherDocument14 pagesPost Mature Neonate, Infant of Diabetic and Substance Abuse MotherShilpa JoshiNo ratings yet
- Cost-Effectiveness Analysis of Induction of Labor at 39 Weeks for Low-Risk Nulliparous WomenDocument10 pagesCost-Effectiveness Analysis of Induction of Labor at 39 Weeks for Low-Risk Nulliparous WomenRosiNo ratings yet
- High Risk Newborn CareDocument5 pagesHigh Risk Newborn Carewerismy daddyNo ratings yet
- Nursing Care of The Client With High-Risk Labor & DeliveryDocument10 pagesNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanNo ratings yet
- Neonatal Birth InjuriesDocument22 pagesNeonatal Birth InjuriesPauli Monsálvez ElissaldeNo ratings yet
- Shoulder DystociaDocument9 pagesShoulder DystociaRorschach VargasNo ratings yet
- Obesity in PregnancyDocument9 pagesObesity in PregnancydarkkryNo ratings yet
- Shoulder Dystocia: Incidence, Mechanisms, and Management StrategiesDocument10 pagesShoulder Dystocia: Incidence, Mechanisms, and Management Strategiesfarida nur ainiNo ratings yet
- 2003 2008 MCQDocument81 pages2003 2008 MCQIshola Segun SamuelNo ratings yet
- Newborn Nursing Care GuideDocument72 pagesNewborn Nursing Care GuideCathreen Agatha FuleNo ratings yet
- Newborn Needs and Care of High-Risk InfantsDocument12 pagesNewborn Needs and Care of High-Risk InfantsIan CarodanNo ratings yet
- Shoulder DystociaDocument63 pagesShoulder Dystociaapi-3841435100% (3)
- M NewbornDocument13 pagesM NewbornDonaJeanNo ratings yet
- OBMQ2 (3) Endocrine Diseases in Pregnancy - Dr. CandelarioDocument8 pagesOBMQ2 (3) Endocrine Diseases in Pregnancy - Dr. Candelarioqsd clinicNo ratings yet
- Managing Type 1 Diabetes in PregnancyDocument34 pagesManaging Type 1 Diabetes in Pregnancyሌናፍ ኡሉምNo ratings yet
- High Risk Newborn I StudentsDocument69 pagesHigh Risk Newborn I Studentsmichelle alvaradoNo ratings yet
- Fetal MacrosomiaDocument11 pagesFetal MacrosomiaLady Jane CaguladaNo ratings yet
- Abnormal Labor - ClinicalKeyDocument32 pagesAbnormal Labor - ClinicalKeyJunior KenNo ratings yet
- Birth TraumaDocument44 pagesBirth TraumasreekalaNo ratings yet
- RCPI Diabetes GuidelinesDocument88 pagesRCPI Diabetes GuidelinesJohn Smith100% (1)
- DystociaDocument12 pagesDystociaKimberly Teofe KwanNo ratings yet
- The Infant of A Diabetic MotherDocument19 pagesThe Infant of A Diabetic MotherapolismarNo ratings yet
- 2019 Canadian Guideline For Physical Activity Throughout PregnancyDocument8 pages2019 Canadian Guideline For Physical Activity Throughout PregnancynirchennNo ratings yet
- Shoulder DystociaDocument37 pagesShoulder DystociaClaudia SanchezNo ratings yet
- Assessment of High Risk New BornDocument31 pagesAssessment of High Risk New BornVarna MohanNo ratings yet
- Diabetes in PregnancyDocument38 pagesDiabetes in Pregnancybdzq3i12No ratings yet
- Nursing Care of High-Risk NewbornsDocument83 pagesNursing Care of High-Risk NewbornsChari RivoNo ratings yet