You might also like
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Obgyn Revalida Review 2022 RcsDocument248 pagesObgyn Revalida Review 2022 RcsSophia SaquilayanNo ratings yet
- Modes of Ventilation Chart - 1Document5 pagesModes of Ventilation Chart - 1Khamra SalahuddinNo ratings yet
- Hypertensive Disorders in PregnancyDocument81 pagesHypertensive Disorders in PregnancyarunshreerajendranNo ratings yet
- Ob Revalida Review 2017 PDFDocument71 pagesOb Revalida Review 2017 PDFMara Medina - BorleoNo ratings yet
- 8TH Edition TNM Classification and Significance of Depth of InvasionDocument75 pages8TH Edition TNM Classification and Significance of Depth of InvasionDR. ISHITA SINGHAL50% (2)
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJeffrey Ramos100% (1)
- Module Four Wellness PlanDocument12 pagesModule Four Wellness Plankayle mylerNo ratings yet
- Manage Hypertension in PregnancyDocument70 pagesManage Hypertension in PregnancyYibelu BazezewNo ratings yet
- Nasw Code of Ethics Exam For ElearningDocument4 pagesNasw Code of Ethics Exam For Elearningapi-97308101No ratings yet
- Anacardium OrientaleDocument21 pagesAnacardium OrientaleAlexandre Funcia100% (1)
- Gestational Diabetes Case Study With Questions For The Undergraduate NurseDocument46 pagesGestational Diabetes Case Study With Questions For The Undergraduate NurseAndrea Donmyer100% (1)
- The High Risk Prenatal ClientDocument46 pagesThe High Risk Prenatal ClientPaul Albert Agunod100% (2)
- Epidemiology MCQDocument122 pagesEpidemiology MCQሌናፍ ኡሉም100% (1)
- Case Study GDM Complete 2017Document34 pagesCase Study GDM Complete 2017GANESANNo ratings yet
- Antenatal Principles of Antenatal Care 2017Document60 pagesAntenatal Principles of Antenatal Care 2017JanielWright100% (3)
- DM in PregDocument32 pagesDM in Pregbryanpei23No ratings yet
- Hypertension Disorder in PregnancyDocument42 pagesHypertension Disorder in Pregnancyholly girlchy JastinNo ratings yet
- Pre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPre-eclampsia, (Pregnancy with Hypertension And Proteinuria) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- GDMDocument11 pagesGDMNikki GarlejoNo ratings yet
- Cataract Case GuideDocument3 pagesCataract Case GuideVetrivel Tamizh100% (1)
- GDMDocument38 pagesGDMAbhishiktaAbhi100% (1)
- Diabetes in Pregnancy: DR Chippy Tess MathewDocument29 pagesDiabetes in Pregnancy: DR Chippy Tess MathewSamanmala Senarath100% (1)
- Gestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro IbadanDocument40 pagesGestational Diabetes: Dr. Oyeyiola Oyebode Registrar Obstetrics and Gynaecology Ola Catholic Hospital, Oluyoro Ibadanoyebode oyeyiolaNo ratings yet
- OME Ob NotesDocument28 pagesOME Ob NotesDori100% (1)
- Gestational ConditionDocument26 pagesGestational ConditionDilausan B MolukNo ratings yet
- In The Name of GodDocument23 pagesIn The Name of GodNinaNo ratings yet
- Hyperglycemias of Pregnancy: Awareness Prevents Catastrophe Early Intervention Prevents ComplicationsDocument57 pagesHyperglycemias of Pregnancy: Awareness Prevents Catastrophe Early Intervention Prevents ComplicationsKazi SiamNo ratings yet
- Management of Pre - EclampsiaDocument22 pagesManagement of Pre - Eclampsiaapi-3705046No ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensioncfgrtwifhNo ratings yet
- 11.pregnancy & Diabetes MellitusDocument23 pages11.pregnancy & Diabetes Mellituskume senbetaNo ratings yet
- Diabetes in Pregnancy GuideDocument7 pagesDiabetes in Pregnancy GuideSalman KhanNo ratings yet
- Gestational DiabetesDocument42 pagesGestational Diabetesjohn jumborock100% (1)
- History, P.E., & Follow-Up of High-Risk Pregnancies: Gestational Diabetes Mellitus PreeclampsiaDocument48 pagesHistory, P.E., & Follow-Up of High-Risk Pregnancies: Gestational Diabetes Mellitus PreeclampsiatabatchNo ratings yet
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateDocument22 pages1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonNo ratings yet
- Diabetes Mellitus in Pregnancy (Int)Document27 pagesDiabetes Mellitus in Pregnancy (Int)zizsatriaNo ratings yet
- Cetoacidosis Diabética Normoglicémica en El Embarazo. Caso ClínicoDocument5 pagesCetoacidosis Diabética Normoglicémica en El Embarazo. Caso ClínicoLvis Zevallos MavricioNo ratings yet
- Management For RDSDocument85 pagesManagement For RDSNurhafizoh HussinNo ratings yet
- Medical Disorders in PXDocument49 pagesMedical Disorders in PXSemon YohannesNo ratings yet
- Infant of Diabetic MotherDocument41 pagesInfant of Diabetic Mothermohdmaghyreh100% (8)
- e Obgyn อยากสอนDocument187 pagese Obgyn อยากสอนSurasit SukseeluangNo ratings yet
- CHBP Progress NoteDocument1 pageCHBP Progress NoteNelson R. PouNo ratings yet
- Hypertensive Conditions in PregnancyDocument59 pagesHypertensive Conditions in PregnancyStanford MarangwandaNo ratings yet
- Maternal Risk Factors and Fetal AssessmentDocument88 pagesMaternal Risk Factors and Fetal AssessmentLeofe CorregidorNo ratings yet
- Cardiac, DM, Substance Abuse LECDocument65 pagesCardiac, DM, Substance Abuse LECFarmisa MannanNo ratings yet
- 1 DMDocument49 pages1 DMDrMohammad KhadrawyNo ratings yet
- GDMDocument61 pagesGDMHaleluya LeulsegedNo ratings yet
- BSN 2C MCN Lec Transes 1 1Document4 pagesBSN 2C MCN Lec Transes 1 1Shahina ShayneNo ratings yet
- Chapter 9: Diabetes During PregnancyDocument2 pagesChapter 9: Diabetes During Pregnancymorasaki003No ratings yet
- Normal Pregnancy and ComplicationsDocument9 pagesNormal Pregnancy and Complicationsoscar sabirNo ratings yet
- Gestational DMDocument32 pagesGestational DMKatNo ratings yet
- Diabetes in Pregnancy: A Case Study and ReviewDocument42 pagesDiabetes in Pregnancy: A Case Study and ReviewToivo S DiegoNo ratings yet
- Maternal Condition Affecting NeonateDocument60 pagesMaternal Condition Affecting NeonateJolmajas JoharNo ratings yet
- Vicente Sotto Memorial Medical Center Department of Obstetrics & GynecologyDocument9 pagesVicente Sotto Memorial Medical Center Department of Obstetrics & GynecologyIrah FloresNo ratings yet
- Counseling Case Presentation - GDMDocument28 pagesCounseling Case Presentation - GDMapi-581342636No ratings yet
- Umanand Prasad School of Medicine and Health ScienceDocument13 pagesUmanand Prasad School of Medicine and Health ScienceShakshi RainaNo ratings yet
- Case Title: PreeclampsiaDocument6 pagesCase Title: PreeclampsiaLanaNo ratings yet
- Nursing Care of The High Risk Pregnancy ClientDocument7 pagesNursing Care of The High Risk Pregnancy ClientJoash Karlo De GuzmanNo ratings yet
- 21.diabetes Mellitus in PregnancyDocument47 pages21.diabetes Mellitus in Pregnancydeneke100% (1)
- Antenatal CareDocument41 pagesAntenatal CareHani NadiahNo ratings yet
- Lecture 2 Dm in PregnancyDocument28 pagesLecture 2 Dm in Pregnancybazuu mbwegzeNo ratings yet
- Preeclampsia EclampsiaDocument40 pagesPreeclampsia EclampsiaPurnama WatiNo ratings yet
- Diabetes in PregnancyDocument75 pagesDiabetes in PregnancyArchana KumariNo ratings yet
- DiabetesDocument41 pagesDiabetesWai Kwong ChiuNo ratings yet
- The Stories That End Badly Are Sad, Sadder Still Are The Ones That Never BeganDocument77 pagesThe Stories That End Badly Are Sad, Sadder Still Are The Ones That Never Begankim soohyunNo ratings yet
- M Kaavya Sree Balaji Medical College and Hospital IndiaDocument33 pagesM Kaavya Sree Balaji Medical College and Hospital IndiaNailahRahmahNo ratings yet
- M Kaavya Sree Balaji Medical College and Hospital IndiaDocument33 pagesM Kaavya Sree Balaji Medical College and Hospital Indiakiritokazuto35No ratings yet
- Maternal Fetal Physiology & Pregnancy ComplicationsDocument28 pagesMaternal Fetal Physiology & Pregnancy ComplicationsHaadi AliNo ratings yet
- ObstetricsDocument216 pagesObstetricsሌናፍ ኡሉምNo ratings yet
- Cerebral Circulation and Cerebrospinal Fluid (CSF) : By: Biruk A September, 2021Document37 pagesCerebral Circulation and Cerebrospinal Fluid (CSF) : By: Biruk A September, 2021ሌናፍ ኡሉምNo ratings yet
- RM AnesthesiaDocument137 pagesRM Anesthesiaሌናፍ ኡሉምNo ratings yet
- Patient Knowledge and Attitude Towards AnesthesiaDocument26 pagesPatient Knowledge and Attitude Towards Anesthesiaሌናፍ ኡሉምNo ratings yet
- Retrospective Review of Elective Gynecologic SurgeriesDocument33 pagesRetrospective Review of Elective Gynecologic Surgeriesሌናፍ ኡሉምNo ratings yet
- NeoplasmDocument76 pagesNeoplasmሌናፍ ኡሉምNo ratings yet
- Introduction To Dentistry & Anatomy of Orofacial Structures: by Moges Tesfaye (DMDDocument96 pagesIntroduction To Dentistry & Anatomy of Orofacial Structures: by Moges Tesfaye (DMDሌናፍ ኡሉምNo ratings yet
- Patient Knowledge and Attitude Towards AnesthesiaDocument26 pagesPatient Knowledge and Attitude Towards Anesthesiaሌናፍ ኡሉምNo ratings yet
- Prenatal Care & Maternal MortalityDocument56 pagesPrenatal Care & Maternal Mortalityሌናፍ ኡሉምNo ratings yet
- Prenatal Care & Maternal MortalityDocument56 pagesPrenatal Care & Maternal Mortalityሌናፍ ኡሉምNo ratings yet
- Prenatal Care & Maternal MortalityDocument56 pagesPrenatal Care & Maternal Mortalityሌናፍ ኡሉምNo ratings yet
- Case Report on 44-Year-Old Woman with Excessive Menstrual BleedingDocument16 pagesCase Report on 44-Year-Old Woman with Excessive Menstrual Bleedingሌናፍ ኡሉምNo ratings yet
- IdentificationDocument4 pagesIdentificationTefera LeteboNo ratings yet
- Obs Case ReportDocument11 pagesObs Case Reportሌናፍ ኡሉምNo ratings yet
- Introduction To ICU: Habtamu G. Dec/2020Document20 pagesIntroduction To ICU: Habtamu G. Dec/2020ሌናፍ ኡሉምNo ratings yet
- Suraksha Final Project Work ModifiedDocument73 pagesSuraksha Final Project Work Modifiedavn6No ratings yet
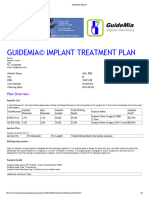
- GuideMia Sample Report - EnglishDocument9 pagesGuideMia Sample Report - Englishzhiao liuNo ratings yet
- Positioning and Drafting ReviewerDocument4 pagesPositioning and Drafting ReviewerKathrina Mendoza HembradorNo ratings yet
- Deeper Root Academy HandbookDocument18 pagesDeeper Root Academy HandbookAdminNo ratings yet
- Sip InformationDocument111 pagesSip InformationakashNo ratings yet
- Revision 2Document7 pagesRevision 2Maina JonnNo ratings yet
- LFD CommunityDocument2 pagesLFD CommunityKryza B. CASTILLONo ratings yet
- OCP - 15 - GrindingDocument2 pagesOCP - 15 - GrindingNagendra Kumar SinghNo ratings yet
- The Zone Issue 27Document16 pagesThe Zone Issue 27Jeff Clay GarciaNo ratings yet
- Oum Business School: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreDocument6 pagesOum Business School: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreInspire28No ratings yet
- Drug Presentation On: Aminoven: Submitted To Submitted byDocument6 pagesDrug Presentation On: Aminoven: Submitted To Submitted byShilpi SinghNo ratings yet
- 22-23 Pan Sloan Canyon Student Parent HandbookDocument81 pages22-23 Pan Sloan Canyon Student Parent Handbookapi-470026636No ratings yet
- The University of Melbourne Tuition Fees 2020: Tuition Fee Tables For International StudentsDocument32 pagesThe University of Melbourne Tuition Fees 2020: Tuition Fee Tables For International StudentsRuchi ChinfhaChinthaNo ratings yet
- Strategies For Minimizing Dispensing ErrorsDocument3 pagesStrategies For Minimizing Dispensing ErrorsAnah MayNo ratings yet
- Name:Muhammad Mustafa REG NO.12397 Assighment:Behavioural Science Topic:Conflict ManagementDocument15 pagesName:Muhammad Mustafa REG NO.12397 Assighment:Behavioural Science Topic:Conflict Managementmustafa wazirNo ratings yet
- How To Know If U Need Ortho TTDocument3 pagesHow To Know If U Need Ortho TTSubhajit SahaNo ratings yet
- Spa CuisineDocument11 pagesSpa CuisineNamanraj Singh JollyNo ratings yet
- Xerox Wc423 SMDocument600 pagesXerox Wc423 SMkerintNo ratings yet
- Lyon, G. R., Shaywitz, S. E., & Shaywitz, B. A. (2003) - A Definition of Dyslexia. Annals of Dyslexia, 53 (1), 1-14 PDFDocument14 pagesLyon, G. R., Shaywitz, S. E., & Shaywitz, B. A. (2003) - A Definition of Dyslexia. Annals of Dyslexia, 53 (1), 1-14 PDFCharitini PetridouNo ratings yet
- Week 12-13-Group Activity-Conceptualizing A Possible GMODocument5 pagesWeek 12-13-Group Activity-Conceptualizing A Possible GMOAlexandra MandrezaNo ratings yet
- Gingival Recession PerioDocument42 pagesGingival Recession PerioFourthMolar.com100% (3)
- Medication Booklet and TicketDocument3 pagesMedication Booklet and TicketCayanne ChuaNo ratings yet
- HKGC Booklet FinalDocument95 pagesHKGC Booklet FinalAtik Badshah SHAIKHNo ratings yet