You might also like
- Forms BDocument14 pagesForms BDaryl Joshua SaturnoNo ratings yet
- To Be Printed Corpuz Hospi Case Scenario 1Document10 pagesTo Be Printed Corpuz Hospi Case Scenario 1Cezanne CruzNo ratings yet
- Nursing Dummy ChartDocument4 pagesNursing Dummy Chartis_aradanasNo ratings yet
- Heparin Infusion Guideline PDFDocument3 pagesHeparin Infusion Guideline PDFbrigde_xNo ratings yet
- KARDEXDocument2 pagesKARDEXChristine Joy Camacho100% (1)
- Vital Signs Monitoring SheetDocument4 pagesVital Signs Monitoring SheetDenvicNo ratings yet
- IBE, Susanna Martha B. 2014-57561 Ward 1Document4 pagesIBE, Susanna Martha B. 2014-57561 Ward 1WazzupNo ratings yet
- Physician's Examination FormDocument1 pagePhysician's Examination FormMason FrasherNo ratings yet
- IV FormDocument1 pageIV FormcindtanNo ratings yet
- Adult Assessment Tool 2014 (GOOD)Document4 pagesAdult Assessment Tool 2014 (GOOD)Basinga Okinam100% (1)
- 47Document2 pages47Gpe C. BaronNo ratings yet
- Checklist Lungs and Thorax 1Document2 pagesChecklist Lungs and Thorax 1Marianne CasamaNo ratings yet
- Patient Monitoring SheetDocument8 pagesPatient Monitoring SheetAndrea Sibayan SorianoNo ratings yet
- Vascularaccess 508 PDFDocument4 pagesVascularaccess 508 PDFVina YuwandaNo ratings yet
- Administration of MedicationDocument0 pagesAdministration of MedicationAmanda's GardenNo ratings yet
- Chest Physiotherapy Evaluation ChecklistDocument3 pagesChest Physiotherapy Evaluation ChecklistJojo JustoNo ratings yet
- Adverse Anaesthesia Event FormDocument2 pagesAdverse Anaesthesia Event FormHarsh100% (1)
- Temperature Pulse and Respiration Rate ChartDocument1 pageTemperature Pulse and Respiration Rate ChartLyons MacNo ratings yet
- Demonstrating Theory in Practice Examples of The McGill Model of NursingDocument10 pagesDemonstrating Theory in Practice Examples of The McGill Model of NursingFerdy LainsamputtyNo ratings yet
- Muscle Strength TestingDocument3 pagesMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Mechanical Ventilation 8.2.17Document41 pagesMechanical Ventilation 8.2.17SyafiqAziziNo ratings yet
- Miracle of LifeDocument3 pagesMiracle of Lifespankey0809No ratings yet
- Labor AssessmentDocument14 pagesLabor AssessmentShay DayNo ratings yet
- Actual SoapiesDocument8 pagesActual SoapiesBeverlyn AsparoNo ratings yet
- Demo Teaching Physical Health AssessmentDocument5 pagesDemo Teaching Physical Health AssessmentJulie May SuganobNo ratings yet
- Midsayap Doctors Specialist Hospital, Inc.: Clinical Cover SheetDocument2 pagesMidsayap Doctors Specialist Hospital, Inc.: Clinical Cover SheetRemej SilutgamNo ratings yet
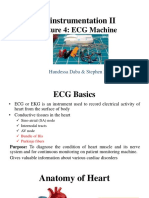
- Bioinstrumentation II: Lecture 4: ECG MachineDocument30 pagesBioinstrumentation II: Lecture 4: ECG MachineHundessa DabaNo ratings yet
- Final Thesis With CV (For Bookbind)Document138 pagesFinal Thesis With CV (For Bookbind)Bea Marie Eclevia100% (1)
- Preoperative Preparation of Patient For SurgeryDocument23 pagesPreoperative Preparation of Patient For SurgeryFauzi SebunyaNo ratings yet
- Turning and Re PositioningDocument13 pagesTurning and Re Positioningclaudia03No ratings yet
- Concept MapDocument6 pagesConcept Mapapi-499028250No ratings yet
- Multiple Choice Question Acn FinalDocument11 pagesMultiple Choice Question Acn FinalIqra rizwanNo ratings yet
- PERIOPERATIVE NURSING PHASESDocument11 pagesPERIOPERATIVE NURSING PHASESDa BondadNo ratings yet
- CS ShockDocument5 pagesCS ShockJuliusSerdeñaTrapal0% (5)
- Intake and Output ChartDocument2 pagesIntake and Output ChartViral Chann3LNo ratings yet
- Health and Wellness ConceptsDocument38 pagesHealth and Wellness ConceptsKathrina AlfonsoNo ratings yet
- Trach Suction ChecklistDocument2 pagesTrach Suction ChecklistJE MagbanuaNo ratings yet
- DispencingDocument19 pagesDispencingushaeatakotaNo ratings yet
- Complications of Intravenous TherapyDocument47 pagesComplications of Intravenous TherapyKateAngeliRebosuraNo ratings yet
- Nursing Assessment Gordon's PatternsDocument3 pagesNursing Assessment Gordon's PatternsJelai DNo ratings yet
- 10 1056@NEJMcpc1913468 PDFDocument10 pages10 1056@NEJMcpc1913468 PDFAbdelkader HociniNo ratings yet
- Routes of Drug Students)Document5 pagesRoutes of Drug Students)yabaeve100% (1)
- Acute Care MapDocument11 pagesAcute Care Mapapi-301727553No ratings yet
- NURSES NOTES With CaseDocument4 pagesNURSES NOTES With CaseGrape JuiceNo ratings yet
- Rle Week 11Document3 pagesRle Week 11Roselyn Yu QuintoNo ratings yet
- Assessing Peripheral PulseDocument1 pageAssessing Peripheral PulseJAN ELMER L. LABESORESNo ratings yet
- Needle Stick Injury FormatDocument1 pageNeedle Stick Injury Formatquality qualityNo ratings yet
- CARDOS NAUSEA FDAR-formatDocument3 pagesCARDOS NAUSEA FDAR-formatGabrielle CardosNo ratings yet
- Pharmacology Test 1: Questions and RationalesDocument52 pagesPharmacology Test 1: Questions and RationalesElla ReyesNo ratings yet
- Antepartum Record Labor WatchDocument4 pagesAntepartum Record Labor WatchMaryJoy rosalesNo ratings yet
- Master Intradermal Injection TechniqueDocument8 pagesMaster Intradermal Injection TechniqueAlfun HidayatullohNo ratings yet
- O2 Therapy ChecklistDocument3 pagesO2 Therapy ChecklistKathlyn PactorananNo ratings yet
- 01 Nursing Note SampleDocument1 page01 Nursing Note Sampletesttest testNo ratings yet
- Wound Care: Section I: Assessing Your UnderstandingDocument12 pagesWound Care: Section I: Assessing Your UnderstandingkeyonaNo ratings yet
- 24 Hour ReportDocument2 pages24 Hour ReportEduardo AnerdezNo ratings yet
- Nurse'S Notes: Date-Shift Focus Data - Action - ResponseDocument5 pagesNurse'S Notes: Date-Shift Focus Data - Action - ResponseRenea Joy ArruejoNo ratings yet
- Cardiac NSG DiagnosisDocument5 pagesCardiac NSG DiagnosisShreyas WalvekarNo ratings yet
- ChesttubedrainageDocument65 pagesChesttubedrainagejerinthomasrajanNo ratings yet
- KARDEXDocument4 pagesKARDEXJemuel DalanaNo ratings yet
- Redoble Medical Clinic Case NoDocument1 pageRedoble Medical Clinic Case Noapi-3836762No ratings yet
- Case 3: Aortic StenosisDocument11 pagesCase 3: Aortic StenosisfmNo ratings yet
- Introduction in Skeletal System1Document11 pagesIntroduction in Skeletal System1joana cortezNo ratings yet
- Epi NotesDocument5 pagesEpi NoteshoneykrizelNo ratings yet
- Your Peak Flow Diary PDFDocument11 pagesYour Peak Flow Diary PDFkalli987No ratings yet
- English For Careers Medicine 2 Student's BookDocument145 pagesEnglish For Careers Medicine 2 Student's BookSt87% (15)
- Near DrowningDocument53 pagesNear DrowningDr. Anish GolchhaNo ratings yet
- Ischialgia Case Report by GaluhDocument22 pagesIschialgia Case Report by GaluhDwi Ulfa AnnisaNo ratings yet
- SouvenirDocument86 pagesSouvenirMohak AroraNo ratings yet
- Evidence Supporting Broader AccessDocument4 pagesEvidence Supporting Broader Accessedi_wsNo ratings yet
- Clinical Intake and MSEDocument5 pagesClinical Intake and MSEkashish behlNo ratings yet
- Psychosis: Is It A Medical Problem?: Dowden Health MediaDocument6 pagesPsychosis: Is It A Medical Problem?: Dowden Health MediaJagdishVankarNo ratings yet
- Lecture-31 Instrumental DeliveryDocument33 pagesLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaNo ratings yet
- Drug Study On PpudDocument3 pagesDrug Study On PpudLezelle Mandane CardinoNo ratings yet
- IV Pyelography procedure and nursing responsibilitiesDocument2 pagesIV Pyelography procedure and nursing responsibilitiesShaina Angelique SaliNo ratings yet
- Kounis Syndrome A Pediatric PerspectiveDocument10 pagesKounis Syndrome A Pediatric PerspectiveAna Belén Artero CastañoNo ratings yet
- HA Integument ChecklistDocument10 pagesHA Integument ChecklistMa Joanna Elizabeth S. PizarroNo ratings yet
- Psychosocial Report (Psychological Report)Document4 pagesPsychosocial Report (Psychological Report)Aerin90% (10)
- Ice TherapyDocument5 pagesIce TherapyDiane CastillonNo ratings yet
- Choledochal CystDocument68 pagesCholedochal CystSyed Waqas HasanNo ratings yet
- Puberty Self-CareDocument13 pagesPuberty Self-CareAira MendozaNo ratings yet
- (Grade 9) MAPEH (Health) - Drugs (2nd)Document3 pages(Grade 9) MAPEH (Health) - Drugs (2nd)KenNo ratings yet
- From Chronic To Critical: A Latino Family Confronts End-of-Life DecisionsDocument2 pagesFrom Chronic To Critical: A Latino Family Confronts End-of-Life DecisionsRoyKimNo ratings yet
- Plasmodium Parasite Life Cycle and SpeciesDocument36 pagesPlasmodium Parasite Life Cycle and SpeciesHibaaq AxmedNo ratings yet
- DNB General Surgery Paper3 examDocument4 pagesDNB General Surgery Paper3 examMalavika RaoNo ratings yet
- Liver CancerDocument233 pagesLiver CancerandikhgNo ratings yet
- Indications For Gingivoectomy and GingivoplastyDocument4 pagesIndications For Gingivoectomy and Gingivoplastyade ismailNo ratings yet
- Viral Diseases MechanismsDocument105 pagesViral Diseases MechanismspolypeptideNo ratings yet
- IPC VS Pulpotomy PDFDocument7 pagesIPC VS Pulpotomy PDFnikitha100% (1)
- Final 2nd Announcement Konas Perdatin Perdici 2019 - WebsiteDocument65 pagesFinal 2nd Announcement Konas Perdatin Perdici 2019 - Websitetia_drNo ratings yet
- Daepoch Protocolo BccancerDocument9 pagesDaepoch Protocolo BccancerLuiz MeloNo ratings yet