You might also like
- Dental CariesDocument18 pagesDental CariesRahayu Sukma Dewi0% (1)
- Oral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood MalignanciesDocument9 pagesOral and Dental Alterations and Growth Disruption Following Chemotherapy in Long-Term Survivors of Childhood MalignanciesGeorgia.annaNo ratings yet
- Developmental Defects of Enamel in Primary TeethDocument8 pagesDevelopmental Defects of Enamel in Primary TeethElizabeth CortésNo ratings yet
- Clinical Decision-Making For Caries Management in Primary TeethDocument10 pagesClinical Decision-Making For Caries Management in Primary TeethbradleycampbellNo ratings yet
- Assessment of Oral Health Status - DMF - 7 PagesDocument8 pagesAssessment of Oral Health Status - DMF - 7 PagesDaniah MNo ratings yet
- Perio PaperDocument9 pagesPerio Paperapi-391478637No ratings yet
- Modern Thoughts On Fissure SealantsDocument5 pagesModern Thoughts On Fissure SealantsSaca AnastasiaNo ratings yet
- Comparison of ICDAS, CAST, Nyvad's Criteria, and WHO-DMFT For Caries DetectionDocument16 pagesComparison of ICDAS, CAST, Nyvad's Criteria, and WHO-DMFT For Caries DetectionMario Troncoso AndersennNo ratings yet
- Caries Process and Prevention StrategiesDocument12 pagesCaries Process and Prevention Strategiesblacknight_81No ratings yet
- Caries Risk Assessment and Management For The Prosthodontic PatientDocument8 pagesCaries Risk Assessment and Management For The Prosthodontic PatientMiguelezp BrunoNo ratings yet
- Wong 2017Document24 pagesWong 2017Ngoc MinhNo ratings yet
- Comprehensive Hospital Dental Clinic, NorthDocument8 pagesComprehensive Hospital Dental Clinic, NorthBarsha JoshiNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Epidemiology of Traumatic Dental Injuries - A 12 Year Review of The LiteratureDocument9 pagesEpidemiology of Traumatic Dental Injuries - A 12 Year Review of The LiteratureLAURA ALEJANDRA LEON CAMPOSNo ratings yet
- D L, H R & L L: Periodontology 2000Document24 pagesD L, H R & L L: Periodontology 2000ph4nt0mgr100% (1)
- Evaluation of Brushing Techniques TaughtDocument5 pagesEvaluation of Brushing Techniques TaughtJavier Cabanillas ArteagaNo ratings yet
- JKPKBPPK GDL Grey 2011 Magdarinad 3690 Missingt ADocument9 pagesJKPKBPPK GDL Grey 2011 Magdarinad 3690 Missingt AIchwan RamadhanNo ratings yet
- Melissa ArticuloDocument11 pagesMelissa ArticuloGLADYS VALENCIANo ratings yet
- ManuscriptDocument24 pagesManuscriptaetuazonNo ratings yet
- Caries Risk Assessment and InterventionDocument5 pagesCaries Risk Assessment and InterventionDelia Guadalupe Gardea ContrerasNo ratings yet
- The Long Term Effect of A Preventive Programme On Caries Periodontal Disease and Tooth Mortality in Individuals With Down SyndromeDocument13 pagesThe Long Term Effect of A Preventive Programme On Caries Periodontal Disease and Tooth Mortality in Individuals With Down SyndromeSaipul AnwarNo ratings yet
- First MDocument14 pagesFirst Mdr parveen bathlaNo ratings yet
- AAPD Policy On Minimally Invasive DentistryDocument4 pagesAAPD Policy On Minimally Invasive DentistryDani BrenerNo ratings yet
- P ProphylaxisDocument5 pagesP ProphylaxisLeticia Quiñonez VivasNo ratings yet
- Gingival RecessionDocument10 pagesGingival RecessionemyNo ratings yet
- TALLER 4selwitz2007Document9 pagesTALLER 4selwitz2007Natalia SplashNo ratings yet
- Erosion Guidelines - 2021 - V4 - MJDocument32 pagesErosion Guidelines - 2021 - V4 - MJAARON DIAZ RONQUILLONo ratings yet
- Tooth Wear 1Document11 pagesTooth Wear 1Kcl Knit A SocNo ratings yet
- Ipi 71009Document16 pagesIpi 71009Sasa YeahNo ratings yet
- Oral Health: Samuel Zwetchkenbaum, DDS, MPH, and L. Susan Taichman, RDH, MPH, PHDDocument20 pagesOral Health: Samuel Zwetchkenbaum, DDS, MPH, and L. Susan Taichman, RDH, MPH, PHDwesamkhouriNo ratings yet
- Newer Concept of Measuring Dental Caries - A ReviewDocument5 pagesNewer Concept of Measuring Dental Caries - A ReviewNadya AyuNo ratings yet
- s41415 023 5624 0 LibreDocument6 pagess41415 023 5624 0 LibreAZWATEE BINTI ABDUL AZIZNo ratings yet
- Dental Caries Management in Children and AdultsDocument6 pagesDental Caries Management in Children and AdultsMitha Ratu amandaNo ratings yet
- 2014 Impacted Wisdom TeethDocument18 pages2014 Impacted Wisdom TeethkaarlaamendezNo ratings yet
- Effect of A School-Based Fluoride Mouth-Rinsing Programme On Dental CariesDocument6 pagesEffect of A School-Based Fluoride Mouth-Rinsing Programme On Dental CariesAishwarya AntalaNo ratings yet
- Archive of SID: Dental Erosion and Its Risk Factors in 12-Year-Old School Children in MashhadDocument6 pagesArchive of SID: Dental Erosion and Its Risk Factors in 12-Year-Old School Children in MashhadAamir BugtiNo ratings yet
- 1.3 Siow, 2023Document10 pages1.3 Siow, 2023Juan Ernesto Del Rosal BethencourtNo ratings yet
- 0108 021011 PDFDocument8 pages0108 021011 PDFKhairunnisa SihotangNo ratings yet
- Caries in Portuguese Children With Down Syndrome: Clinical ScienceDocument4 pagesCaries in Portuguese Children With Down Syndrome: Clinical ScienceDavid AndradeNo ratings yet
- 173-Research Results-582-2-2-20220511Document6 pages173-Research Results-582-2-2-20220511panduutamidrgNo ratings yet
- Contemporary Diagnosis and Management of Dental ErosionDocument10 pagesContemporary Diagnosis and Management of Dental ErosionAndreea AddaNo ratings yet
- Guidelines BookDocument16 pagesGuidelines BookAdel ElaroudNo ratings yet
- Inequalities of Caries Experience in Nevada Youth Expressed by DMFT Index vs. Significant Caries Index (Sic) Over TimeDocument10 pagesInequalities of Caries Experience in Nevada Youth Expressed by DMFT Index vs. Significant Caries Index (Sic) Over TimeSOMVIR KUMARNo ratings yet
- Distribution of White Spot Lesions Among Orthodontic Patients Attending Teaching Institutes in KhartoumDocument7 pagesDistribution of White Spot Lesions Among Orthodontic Patients Attending Teaching Institutes in Khartoumlilik eka radiatiNo ratings yet
- Dental CariesDocument41 pagesDental Cariescopy smartNo ratings yet
- KennedyDocument4 pagesKennedyCristinaNo ratings yet
- Studii GermaniaDocument5 pagesStudii Germaniahritcu anaNo ratings yet
- Research Article: Tooth-And Patient-Related Conditions May Influence Root Canal Treatment IndicationDocument10 pagesResearch Article: Tooth-And Patient-Related Conditions May Influence Root Canal Treatment IndicationIrzam PratamaNo ratings yet
- Comprehensive Review of Caries Assessment Systems Developed Over The Last DecadeDocument6 pagesComprehensive Review of Caries Assessment Systems Developed Over The Last DecadeAmelia RosyidaNo ratings yet
- Dental and Oral Condition in Leprosy Patients From Serra, BrazilDocument8 pagesDental and Oral Condition in Leprosy Patients From Serra, BrazilSudhakar NaiduNo ratings yet
- Longetivity of DentureDocument9 pagesLongetivity of DentureShyam DangarNo ratings yet
- Analysis of Extracted and Retreated Root Canal Treatment Failures in A Nigerian University Teaching HospitalDocument6 pagesAnalysis of Extracted and Retreated Root Canal Treatment Failures in A Nigerian University Teaching HospitalMakko Makoto PNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG Denpasar PDFZaenuriNo ratings yet
- Pengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG DenpasarDocument11 pagesPengaruh Aplikasi Topical Dengan Larutan NaF Dan SnF2 Dalam Pencegahan Karies Ni Made Sirat JKG DenpasarZaenuriNo ratings yet
- Pediatric Dental Care: Open Access: Dental Erosion in 8 and 15-Year-Old School Children and Associated FactorsDocument7 pagesPediatric Dental Care: Open Access: Dental Erosion in 8 and 15-Year-Old School Children and Associated FactorsR Muhammad Reza RamadhanNo ratings yet
- Murthy Untreated Caries 2014Document5 pagesMurthy Untreated Caries 2014Kugendran VRNo ratings yet
- Dental Trauma GuidelinesDocument16 pagesDental Trauma GuidelinesKhushbu AggarwalNo ratings yet
- Dorsal SlitDocument5 pagesDorsal SlitarikaNo ratings yet
- Hiroshi Do I InterviewDocument0 pagesHiroshi Do I InterviewAurelian CurinNo ratings yet
- 12 Pipes and CisternDocument40 pages12 Pipes and Cisternhemanth kumarNo ratings yet
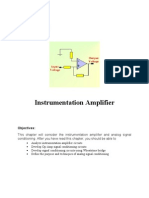
- Chapter-3 Op AmpDocument19 pagesChapter-3 Op Ampmubs73No ratings yet
- Transpo Vrc2010 Tester Manual 2021Document780 pagesTranspo Vrc2010 Tester Manual 2021frederick.lucas4154No ratings yet
- SLK20R - Data SheetDocument2 pagesSLK20R - Data SheetAhmed MijwilNo ratings yet
- MTM Ingliz Tili Ish RejaDocument3 pagesMTM Ingliz Tili Ish RejaUmidaNo ratings yet
- Prolift 430R: Opener ForDocument12 pagesProlift 430R: Opener ForNatasha GlennNo ratings yet
- More Serious Health ProblemsDocument3 pagesMore Serious Health ProblemsYassin KhanNo ratings yet
- Essential Medical Supplies and EquipmentsDocument41 pagesEssential Medical Supplies and EquipmentsKashif BashirNo ratings yet
- Survey of Techniques For Pulmonary Disease Classification Using Deep LearningDocument5 pagesSurvey of Techniques For Pulmonary Disease Classification Using Deep LearningAbdul MoaizNo ratings yet
- Work 2dos - Indigenous and Piñata-6 NovDocument1 pageWork 2dos - Indigenous and Piñata-6 NovDoris50% (2)
- Xdeed3qtt - 1 - Concepts in The Care of at Risk and Sick Adult ClientsDocument14 pagesXdeed3qtt - 1 - Concepts in The Care of at Risk and Sick Adult ClientsCamille GuintoNo ratings yet
- The Western Desert Versus Nile Delta A C PDFDocument17 pagesThe Western Desert Versus Nile Delta A C PDFSohini ChatterjeeNo ratings yet
- CHAPTER 7 Project Management and Network AnalysisDocument31 pagesCHAPTER 7 Project Management and Network AnalysisNitinNo ratings yet
- Blood Grouping (Ashish Singh)Document3 pagesBlood Grouping (Ashish Singh)Ashish SinghNo ratings yet
- Lab Report DilatometerDocument7 pagesLab Report DilatometerTaqqi HaiderNo ratings yet
- N304DN/15 JUL/RBR-TBT: - Not For Real World NavigationDocument21 pagesN304DN/15 JUL/RBR-TBT: - Not For Real World NavigationFrancisco FortesNo ratings yet
- Project Proposal Form (Edexcel) 2Document3 pagesProject Proposal Form (Edexcel) 2Максим КарплюкNo ratings yet
- ValdorDocument1 pageValdorprojectkmoNo ratings yet
- Ref 12Document12 pagesRef 12Tiago BaraNo ratings yet
- Wildlife Checklist Aug15 Low Res Locked For Web 2Document2 pagesWildlife Checklist Aug15 Low Res Locked For Web 2api-703566868No ratings yet
- Tube Filling Machines: TFS 80-1 TFS 80-2Document8 pagesTube Filling Machines: TFS 80-1 TFS 80-2mhafizanNo ratings yet
- 2.1 Pre Lab Stage 2019Document61 pages2.1 Pre Lab Stage 2019Mohd Hilmi Bin MalekNo ratings yet
- IMSA GTD Spec Scrutineering Manual v0.3Document42 pagesIMSA GTD Spec Scrutineering Manual v0.3emanuelNo ratings yet
- Gulf of Mannar Guide PDFDocument78 pagesGulf of Mannar Guide PDFDrVarghese Plavila JohnNo ratings yet
- 23Document61 pages23api-193870757No ratings yet
- Isuzu Pick UpDocument6 pagesIsuzu Pick UpjibooryNo ratings yet
- About WELDA Anchor PlateDocument1 pageAbout WELDA Anchor PlateFircijevi KurajberiNo ratings yet
- 3 Module in Arts Week 3 4Document8 pages3 Module in Arts Week 3 4ARVEE DAVE GIPANo ratings yet