0% found this document useful (0 votes)
317 views3 pagesCOPD Case Study for Health Students
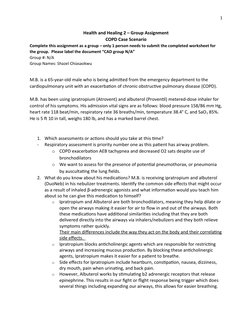
M.B. is a 65-year-old male admitted to the hospital for an exacerbation of COPD with symptoms of tachypnea, low oxygen saturation, and a high heart rate and temperature. His respiratory status is the top priority to assess along with ordering tests like chest x-rays and bloodwork to check for signs of infection or respiratory acidosis. The patient is prescribed various bronchodilators and antibiotics to treat his symptoms and potential infection along with pursed lip breathing techniques and oxygen supplementation.
Uploaded by
shazel chiasaokwuCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
317 views3 pagesCOPD Case Study for Health Students
M.B. is a 65-year-old male admitted to the hospital for an exacerbation of COPD with symptoms of tachypnea, low oxygen saturation, and a high heart rate and temperature. His respiratory status is the top priority to assess along with ordering tests like chest x-rays and bloodwork to check for signs of infection or respiratory acidosis. The patient is prescribed various bronchodilators and antibiotics to treat his symptoms and potential infection along with pursed lip breathing techniques and oxygen supplementation.
Uploaded by
shazel chiasaokwuCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
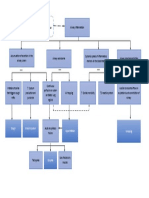
- Introduction to COPD Case: Presents the group's task of assessing and addressing a chronic obstructive pulmonary disease (COPD) case scenario.
- Clinical Features Comparison: Compares clinical features of COPD with other conditions like asthma.
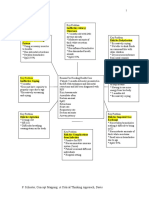
- Intervention Strategy: Details the intervention strategies for the patient's treatment plan focusing on medication order rationales.
- Evaluation of Intervention: Discusses the outcome evaluation, particularly the reduction of breathlessness as an indicator of success.