You might also like
- NSSCO - Mathematics Paper 2 6131-2 - First Proof 08.04.2022Document20 pagesNSSCO - Mathematics Paper 2 6131-2 - First Proof 08.04.2022Auwanga Enkali100% (1)
- Ifn Si LupusDocument1 pageIfn Si LupusdeliaNo ratings yet
- Dengue Fever With Hepatitis E and Hepatitis A Infection PDFDocument2 pagesDengue Fever With Hepatitis E and Hepatitis A Infection PDFAMENDBENo ratings yet
- PancreatitisDocument5 pagesPancreatitisPanchito2000100% (1)
- Lupus Dupa InterferonDocument3 pagesLupus Dupa InterferondeliaNo ratings yet
- Lupus Si Ifn GeneralitatiDocument3 pagesLupus Si Ifn GeneralitatideliaNo ratings yet
- Letters Correspondence: To EditorDocument1 pageLetters Correspondence: To EditorAraNo ratings yet
- Manifestaciones Extrahepaticas Hepatitis CDocument15 pagesManifestaciones Extrahepaticas Hepatitis CSMIBA MedicinaNo ratings yet
- Hemophagocytic Syndrome Due To Infection by H1N1 Influenza VirusDocument5 pagesHemophagocytic Syndrome Due To Infection by H1N1 Influenza VirusAnonymous zENwrie4No ratings yet
- A Case Report of Invasive Aspergillosis in A Patient Treated With RuxolitinibDocument3 pagesA Case Report of Invasive Aspergillosis in A Patient Treated With RuxolitinibJongga SiahaanNo ratings yet
- Polirradiculo SifilisDocument2 pagesPolirradiculo SifilisBatgirl xoxoNo ratings yet
- Mycobacterium Other Than Tuberculosis (MOTT) Infection: An Emerging Disease in Infliximab-Treated PatientsDocument4 pagesMycobacterium Other Than Tuberculosis (MOTT) Infection: An Emerging Disease in Infliximab-Treated PatientsFahmi Afif AlbonehNo ratings yet
- IVIG Treatment in HIVDocument2 pagesIVIG Treatment in HIVovirosNo ratings yet
- 5.5.4 BMJ Case Reports 2019 Pizzarossa RodríguezDocument3 pages5.5.4 BMJ Case Reports 2019 Pizzarossa RodríguezAna PizzarossaNo ratings yet
- Annals of Clinical Case Reports: Hemolytic Anemia - A Rare Case ReportDocument3 pagesAnnals of Clinical Case Reports: Hemolytic Anemia - A Rare Case ReportDumindu PereraNo ratings yet
- Oral Presentations 26 September 2019 I7Document2 pagesOral Presentations 26 September 2019 I7dentsavvyNo ratings yet
- Preprints202009 0544 v2Document10 pagesPreprints202009 0544 v2matsuyamateoNo ratings yet
- Staphy 2Document5 pagesStaphy 2Alexandra MariaNo ratings yet
- HSV2Document5 pagesHSV2daniela_chrc9100No ratings yet
- Evan Syndrome A Case ReportDocument3 pagesEvan Syndrome A Case ReportEditor IJTSRDNo ratings yet
- Publicacion ArticulosDocument3 pagesPublicacion ArticulosANy CastRoNo ratings yet
- Late Ebola Virus Relapse Causing Meningoencephalitis 2016Document6 pagesLate Ebola Virus Relapse Causing Meningoencephalitis 2016AlvaroGuerreroNo ratings yet
- Recurrent Aseptic Meningitis in A Child: Case ReportDocument3 pagesRecurrent Aseptic Meningitis in A Child: Case ReportAprimadhansari FarzimNo ratings yet
- Management of HemophagocyticDocument10 pagesManagement of HemophagocyticAlexander CanoNo ratings yet
- A Chronic Lymphocytic Leukemia Patient With Progressive Multifocal Leukoencephalopathy Caused by John Cunningham VirusDocument8 pagesA Chronic Lymphocytic Leukemia Patient With Progressive Multifocal Leukoencephalopathy Caused by John Cunningham VirusYtyNo ratings yet
- FullDocument9 pagesFulldeliaNo ratings yet
- De Novo Aih After LT GuidoDocument11 pagesDe Novo Aih After LT GuidoEmma SaelensNo ratings yet
- Hepatitis C Mixed Cryoglobulinemia With Undetectable Viral Load: A Case SeriesDocument4 pagesHepatitis C Mixed Cryoglobulinemia With Undetectable Viral Load: A Case SeriesNicoleta ChipailaNo ratings yet
- Wang 2017 KKKDocument5 pagesWang 2017 KKKTais LineNo ratings yet
- Guillain-Barre Syndrome or Is It?Document4 pagesGuillain-Barre Syndrome or Is It?ThimiNo ratings yet
- Ma 2010Document8 pagesMa 2010Lizeth Rincon DelgadoNo ratings yet
- 74 Year Old Woman With Fatigue, Anorexia, and AbdoDocument6 pages74 Year Old Woman With Fatigue, Anorexia, and AbdoRamiro Arraya MierNo ratings yet
- PIIS1198743X14652605Document3 pagesPIIS1198743X14652605Gerald NacoNo ratings yet
- A Quien Punzar en NEURO SIFILISDocument10 pagesA Quien Punzar en NEURO SIFILISMellissa García ParedesNo ratings yet
- Clinical Nephrology and Renal Care: ClinmedDocument3 pagesClinical Nephrology and Renal Care: ClinmedChandan VishwakarmaNo ratings yet
- Case Series of Syphilis and HIV Co-InfectionsDocument3 pagesCase Series of Syphilis and HIV Co-InfectionsZakia DrajatNo ratings yet
- RdkcjaDocument13 pagesRdkcjamilmrch523No ratings yet
- Immune Reconstitution Inflammatory Syndrome and Cerebral ToxoplasmosisDocument2 pagesImmune Reconstitution Inflammatory Syndrome and Cerebral ToxoplasmosisFirda PotterNo ratings yet
- Fulminant Hemophagocytic Lymphohistiocytosis Induced by Pandemic A (H1N1) Influenza: A Case ReportDocument4 pagesFulminant Hemophagocytic Lymphohistiocytosis Induced by Pandemic A (H1N1) Influenza: A Case ReportrahNo ratings yet
- Annrheumd00265 0070Document7 pagesAnnrheumd00265 0070Ravi KiranNo ratings yet
- Nefrita Lupica Care Mimeaza Nefropatie Asociata Virus CDocument5 pagesNefrita Lupica Care Mimeaza Nefropatie Asociata Virus CdeliaNo ratings yet
- Polimorfismo Interferon Com VirusDocument4 pagesPolimorfismo Interferon Com Viruslouisehip UFCNo ratings yet
- Nelson 2017Document28 pagesNelson 2017Santiago GonzalezNo ratings yet
- The Spectrum Evan SydromDocument4 pagesThe Spectrum Evan SydromMohankummar MuniandyNo ratings yet
- Zika Virus Infection Complicated by Guillain-Barré Syndrome - Case Report, French Polynesia, December 2013Document3 pagesZika Virus Infection Complicated by Guillain-Barré Syndrome - Case Report, French Polynesia, December 2013mikeb92556No ratings yet
- EnovaraDocument4 pagesEnovaraenilNo ratings yet
- HIV N Leprosy 2011Document4 pagesHIV N Leprosy 2011Nur CameliaNo ratings yet
- Norovirus 1Document11 pagesNorovirus 1AnisaLFNo ratings yet
- Ramsay Hunt SyndromeDocument3 pagesRamsay Hunt SyndromepicassowaffleNo ratings yet
- Meyer 2015Document5 pagesMeyer 2015Nasrin Akther ShopnaNo ratings yet
- Case Report Herpes EncephalitisDocument3 pagesCase Report Herpes EncephalitisAyu WindyaningrumNo ratings yet
- Interferon Alpha Gene Expression and Serum Level Association With Low Vitamin D Levels in Egyptian Female Patients With Systemic Lupus ErythematosusDocument11 pagesInterferon Alpha Gene Expression and Serum Level Association With Low Vitamin D Levels in Egyptian Female Patients With Systemic Lupus ErythematosusLizeth Rincon DelgadoNo ratings yet
- Elena HepDocument2 pagesElena HepMirela IoanaNo ratings yet
- 2761 8144 1 SMDocument6 pages2761 8144 1 SMAnnisa apriliaNo ratings yet
- Case Report: Acute Hepatitis E in A Pediatric Traveler Presenting With Features of Autoimmune Hepatitis: A Diagnostic and Therapeutic ChallengeDocument4 pagesCase Report: Acute Hepatitis E in A Pediatric Traveler Presenting With Features of Autoimmune Hepatitis: A Diagnostic and Therapeutic Challengeanjingbasah 24No ratings yet
- Terapia Antifungica en Pacientes Con Neutropenia Febril PersistenteDocument7 pagesTerapia Antifungica en Pacientes Con Neutropenia Febril PersistenteMargarita MejiaNo ratings yet
- 429715457-Serological Markers of Autoimmunity in Children With Hepatitis A, Fulminant PresentaciónDocument9 pages429715457-Serological Markers of Autoimmunity in Children With Hepatitis A, Fulminant PresentaciónChristian RosalesNo ratings yet
- Lupus SeverDocument3 pagesLupus SeverdeliaNo ratings yet
- HivDocument29 pagesHivSUTHAN100% (2)
- Human Herpes Virus-6Document3 pagesHuman Herpes Virus-64563748635No ratings yet
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementFrom EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouNo ratings yet
- Impact of Immunosuppressive Regimen On Survival Of.20Document6 pagesImpact of Immunosuppressive Regimen On Survival Of.20deliaNo ratings yet
- Outcome Pe Termen Lung La AsociereDocument6 pagesOutcome Pe Termen Lung La AsocieredeliaNo ratings yet
- MMF Si VHC TransplantDocument11 pagesMMF Si VHC TransplantdeliaNo ratings yet
- VHC Si LesDocument4 pagesVHC Si LesdeliaNo ratings yet
- Lupus Si Ifn SpaniolaDocument3 pagesLupus Si Ifn SpanioladeliaNo ratings yet
- Outcome Dupa Prednisolon Si CiclofDocument8 pagesOutcome Dupa Prednisolon Si CiclofdeliaNo ratings yet
- MODULE 6 Project ManagementDocument20 pagesMODULE 6 Project ManagementMohammed JeeshanNo ratings yet
- MCQ Anatomy-thorax-Abdo-PelvisDocument100 pagesMCQ Anatomy-thorax-Abdo-PelvisMatt McCannNo ratings yet
- Blockchain & Cyber Security. Let's DiscussDocument14 pagesBlockchain & Cyber Security. Let's DiscussPoojaNo ratings yet
- Chef MimasDocument43 pagesChef Mimassarang shahNo ratings yet
- Utilization and Conservation of Water Resources in BangladeshDocument13 pagesUtilization and Conservation of Water Resources in BangladeshAbir MohammadNo ratings yet
- MOSFET P7NK80ZFP DatasheetDocument17 pagesMOSFET P7NK80ZFP DatasheetYuridia De la RosaNo ratings yet
- Why Invest in A Business To Business (B2B) FranchiseDocument8 pagesWhy Invest in A Business To Business (B2B) FranchiseJourney JerodNo ratings yet
- Junk Food 10aDocument3 pagesJunk Food 10aManastirea ContNo ratings yet
- DELTA Plus Model & Five Stages of Analytics Maturity: A PrimerDocument12 pagesDELTA Plus Model & Five Stages of Analytics Maturity: A Primeroscar andres morales perezNo ratings yet
- Comparative Study Among Parle, Perfetti, Britannia & HLLDocument3 pagesComparative Study Among Parle, Perfetti, Britannia & HLLVijay RaiyaniNo ratings yet
- Evaluation and Program Planning: David J. Peyton, Michael ScicchitanoDocument7 pagesEvaluation and Program Planning: David J. Peyton, Michael Scicchitanoannak guerreroNo ratings yet
- Bower Boiler SteelsDocument3 pagesBower Boiler Steelsraut_1234100% (1)
- Myocardial Infarction and Heart Failure Practice Quiz (70 Questions)Document44 pagesMyocardial Infarction and Heart Failure Practice Quiz (70 Questions)Melodia Turqueza GandezaNo ratings yet
- CV Edward GurningDocument2 pagesCV Edward GurningRidwan GurningNo ratings yet
- Fema306 PDFDocument270 pagesFema306 PDFSuhas MangaloreNo ratings yet
- Corbett Controls To Low Sulphidation Epithermal Au AbDocument4 pagesCorbett Controls To Low Sulphidation Epithermal Au AbAriyanto WibowoNo ratings yet
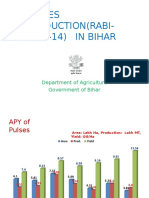
- Pulses Production (Rabi-2013-14) IN BIHAR: Department of Agriculture Government of BiharDocument13 pagesPulses Production (Rabi-2013-14) IN BIHAR: Department of Agriculture Government of BiharviewpawanNo ratings yet
- Issue 64Document20 pagesIssue 64thesacnewsNo ratings yet
- Insurance TrendsDocument19 pagesInsurance TrendsMaithili GuptaNo ratings yet
- World Top 10 Inteligence Agencies - WWW - Theworldtoptens - ComDocument43 pagesWorld Top 10 Inteligence Agencies - WWW - Theworldtoptens - Commahbobullah rahmaniNo ratings yet
- Sample Chit For Sealing VenueDocument3 pagesSample Chit For Sealing Venuepallabothula 789No ratings yet
- Earthing Philosophy 161012H - 34 Pag - 6.11 MB PDFDocument34 pagesEarthing Philosophy 161012H - 34 Pag - 6.11 MB PDFconstantinNo ratings yet
- Hikaru Nara: D E C#M F#M F#MDocument2 pagesHikaru Nara: D E C#M F#M F#MStevan MT PutraNo ratings yet
- Molecular Dynamics Simulation of The Polymer Electrolyte Poly (Ethylene Oxide) / Li CL O 4 - II. Dynamical PropertiesDocument9 pagesMolecular Dynamics Simulation of The Polymer Electrolyte Poly (Ethylene Oxide) / Li CL O 4 - II. Dynamical PropertiesMiguel Iban DelgadoNo ratings yet
- Manual SharpDocument156 pagesManual SharpIon VasilescuNo ratings yet
- Communism: Definition, Characteristics, Pros, Cons & ExamplesDocument17 pagesCommunism: Definition, Characteristics, Pros, Cons & ExamplesJeremie LoyolaNo ratings yet
- 6 Categories of Information SystemDocument10 pages6 Categories of Information SystemCharmaine MagtangobNo ratings yet
- BIAL - Vendor Registration FormDocument2 pagesBIAL - Vendor Registration Formaman3327No ratings yet
- Quiz 12Document6 pagesQuiz 12John Taylor BernasNo ratings yet