83% found this document useful (12 votes)
20K views2 pagesVehicle Safety Inspection Checklist
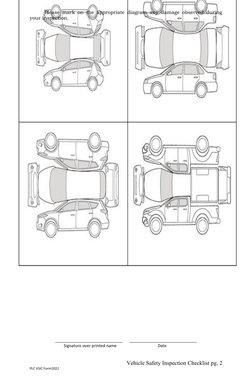
The vehicle safety inspection checklist provides a comprehensive list to inspect the lights, interior, gauges, exterior, and fluid levels of a vehicle. The inspector is to check off items that are in good working condition and note items that need repair or replacement. Any other findings or observations should also be included. Upon completion of the inspection, the operator signs and dates the form to certify that all checked items are in working order. Damage observed during the inspection should also be marked on a diagram.
Uploaded by
ALMEDA INCCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
83% found this document useful (12 votes)
20K views2 pagesVehicle Safety Inspection Checklist
The vehicle safety inspection checklist provides a comprehensive list to inspect the lights, interior, gauges, exterior, and fluid levels of a vehicle. The inspector is to check off items that are in good working condition and note items that need repair or replacement. Any other findings or observations should also be included. Upon completion of the inspection, the operator signs and dates the form to certify that all checked items are in working order. Damage observed during the inspection should also be marked on a diagram.
Uploaded by
ALMEDA INCCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd