You might also like
- KamranDocument1 pageKamranAnonymous BZQOJwWIh6No ratings yet
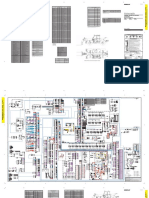
- 793B Truck With VIMS Electrical System: 1HL195-UPDocument2 pages793B Truck With VIMS Electrical System: 1HL195-UPGilvan JuniorNo ratings yet
- Load shedding panel components and devicesDocument1 pageLoad shedding panel components and devicesAnonymous BZQOJwWIh6No ratings yet
- 928G 6XR ElectricoDocument4 pages928G 6XR ElectricoRodney Richardson100% (3)
- TH220BDocument4 pagesTH220BHamilton MirandaNo ratings yet
- 13.8kV AUTO BUS TRANSFER SCHEME PANEL +ABTSDocument1 page13.8kV AUTO BUS TRANSFER SCHEME PANEL +ABTSAnonymous BZQOJwWIh6No ratings yet
- 214690C-000-SOW-1410-0001 - REV A - SignedDocument39 pages214690C-000-SOW-1410-0001 - REV A - SignedMohamed AskarNo ratings yet
- D-1100-Pid-004 Cause and Effect ProcessDocument17 pagesD-1100-Pid-004 Cause and Effect ProcessRizky Perdana PutraNo ratings yet
- 993K Wheel Loader Electrical System: Harness and Wire Electrical Schematic SymbolsDocument6 pages993K Wheel Loader Electrical System: Harness and Wire Electrical Schematic SymbolsLeoNo ratings yet
- RA-159742 001 01 cabinet drawing and BOMDocument1 pageRA-159742 001 01 cabinet drawing and BOMsalman1111aNo ratings yet
- D7H Series II Tractor Electrical SystemDocument2 pagesD7H Series II Tractor Electrical SystemAnonymous KOtSfT6q100% (1)
- Dokumen - Tips Samsung GT E1200 SchematicsDocument7 pagesDokumen - Tips Samsung GT E1200 SchematicsHogir DoskyNo ratings yet
- 1C4 (KSS021-D-528) - Column-R1Document1 page1C4 (KSS021-D-528) - Column-R1mo3azNo ratings yet
- 993K Wheel Loader Electrical System: Harness and Wire Electrical Schematic SymbolsDocument6 pages993K Wheel Loader Electrical System: Harness and Wire Electrical Schematic SymbolsNorman CoetzeeNo ratings yet
- 101 - P&id MGF Acf Ro 30M3HR 17012023Document1 page101 - P&id MGF Acf Ro 30M3HR 17012023Sai Kiran PalikaNo ratings yet
- Ficha J2zzpv4tt5818pxf4ohmm8312xuihlDocument15 pagesFicha J2zzpv4tt5818pxf4ohmm8312xuihlJulio Cruzado SolanoNo ratings yet
- Planoa Electricos de 140mDocument6 pagesPlanoa Electricos de 140mDaniel Castillo Peña100% (1)
- Sis ElectrocaterDocument6 pagesSis Electrocaterndawkhalifaababacar89No ratings yet
- Plano ElectricoDocument2 pagesPlano Electricomauricio suarezNo ratings yet
- Me-2001a (3) - 231004-Basement 2 Layout Plan Sheet ADocument1 pageMe-2001a (3) - 231004-Basement 2 Layout Plan Sheet AhumcanopNo ratings yet
- DFGFGNGDocument1 pageDFGFGNGdianNo ratings yet
- Diagrama Hidraulico Caterpillar 345cDocument2 pagesDiagrama Hidraulico Caterpillar 345cJose Miguel Gary Vargas100% (1)
- AP-1055B ASPHALT PAVER 8BM Diagrama Hidraulico PDFDocument2 pagesAP-1055B ASPHALT PAVER 8BM Diagrama Hidraulico PDFchakroune100% (1)
- 072744C 000 PP 866 - 0 PDFDocument15 pages072744C 000 PP 866 - 0 PDFAbdul FitriNo ratings yet
- TH220Document4 pagesTH220Ventsislav VenevNo ratings yet
- MT Type Esp Installation Manual: 0814 B090 DCCQ 006 0 1/36Document1 pageMT Type Esp Installation Manual: 0814 B090 DCCQ 006 0 1/36rajuNo ratings yet
- 966H Diagrama Electrico 1Document4 pages966H Diagrama Electrico 1Florencio MaximilianoNo ratings yet
- Procedure For Positive Material Identification at Vendor'S WorksDocument7 pagesProcedure For Positive Material Identification at Vendor'S WorksAjay BaggaNo ratings yet
- Technical Specification For Site Preparation Earthworks - Roads & FencingDocument62 pagesTechnical Specification For Site Preparation Earthworks - Roads & FencingAhmed Samir Salim100% (1)
- M-20103 - Rev.1 (Dry Mortar Mixer) - EnglishDocument2 pagesM-20103 - Rev.1 (Dry Mortar Mixer) - EnglishidilfitriNo ratings yet
- 2495 000 JSD 2200 02 - CDocument31 pages2495 000 JSD 2200 02 - CSinaNo ratings yet
- 6420-6000-Et-5930-4 - Ra Part-1Document259 pages6420-6000-Et-5930-4 - Ra Part-1MayankNo ratings yet
- H019-MND-MHS4-CVS-S-DFM-005 - 494 of 721 - 00Document1 pageH019-MND-MHS4-CVS-S-DFM-005 - 494 of 721 - 00Rahul MahajanNo ratings yet
- Fuse Block WiringDocument4 pagesFuse Block WiringGilson RodriguesNo ratings yet
- W-20101 Rev.1 (Belt Weigher) EnglishDocument2 pagesW-20101 Rev.1 (Belt Weigher) EnglishidilfitriNo ratings yet
- PM-1 FRONT SIDE VIEWDocument1 pagePM-1 FRONT SIDE VIEWdelvi.panjaitan097No ratings yet
- D10T Track-Type Tractor Electrical System: Machine Harness Connector and Component LocationsDocument4 pagesD10T Track-Type Tractor Electrical System: Machine Harness Connector and Component LocationsJorge Armando CortezNo ratings yet
- 422e 428e Hydo PDFDocument2 pages422e 428e Hydo PDFdenis100% (1)
- TECHNIP KT INDIA LIMITED STORAGE MANUALDocument1 pageTECHNIP KT INDIA LIMITED STORAGE MANUALrajuNo ratings yet
- Handling, Transportation and Storage Manual: MT Type EspDocument1 pageHandling, Transportation and Storage Manual: MT Type EsprajuNo ratings yet
- 2495 000 JSD 2200 01 - CDocument26 pages2495 000 JSD 2200 01 - CSinaNo ratings yet
- Rotating Equipment List: A. ProcessDocument2 pagesRotating Equipment List: A. ProcesshungNo ratings yet
- Fuente SeguraDocument4 pagesFuente SeguraAlexander ChillitupaNo ratings yet
- Denah Kusen Pintu Dan Jendela Lantai P2: Tower A Tower BDocument1 pageDenah Kusen Pintu Dan Jendela Lantai P2: Tower A Tower Bharianto al faisNo ratings yet
- Electricity & Gas Infrastructure MalaysiaDocument1 pageElectricity & Gas Infrastructure MalaysiaKoay FTNo ratings yet
- Akh Ymi DD Im10x D Ar DWG 0001 1Document1 pageAkh Ymi DD Im10x D Ar DWG 0001 1Tamrayehu KuremaNo ratings yet
- Motoniveladora 140KDocument2 pagesMotoniveladora 140KAbraão Silva100% (5)
- S781-CV-DWG-00004-01-213036-B - OQ Approved - 14.03.2023Document2 pagesS781-CV-DWG-00004-01-213036-B - OQ Approved - 14.03.2023MDhana SekarNo ratings yet
- Welding Activities ManagementDocument18 pagesWelding Activities ManagementStanley AlexNo ratings yet
- RENR81230001Document2 pagesRENR81230001ANDRESNo ratings yet
- Kenr7125kenr7125-01 Sis PDFDocument2 pagesKenr7125kenr7125-01 Sis PDFHector Dongo ArrayanNo ratings yet
- Instant Assessments for Data Tracking, Grade 1: MathFrom EverandInstant Assessments for Data Tracking, Grade 1: MathRating: 4 out of 5 stars4/5 (1)
- Math Workshop, Grade 3: A Framework for Guided Math and Independent PracticeFrom EverandMath Workshop, Grade 3: A Framework for Guided Math and Independent PracticeNo ratings yet
- Instant Assessments for Data Tracking, Grade 2: MathFrom EverandInstant Assessments for Data Tracking, Grade 2: MathNo ratings yet
- Math Workshop, Grade 1: A Framework for Guided Math and Independent PracticeFrom EverandMath Workshop, Grade 1: A Framework for Guided Math and Independent PracticeNo ratings yet
- Instant Assessments for Data Tracking, Grade 1: Language ArtsFrom EverandInstant Assessments for Data Tracking, Grade 1: Language ArtsNo ratings yet
- Oxidation of CopperDocument21 pagesOxidation of CopperAmeen ShahidNo ratings yet
- Arnold Jacobs: His Global Influence: Midwest Clinic, Thursday, December 17 12:00-1:00pmDocument17 pagesArnold Jacobs: His Global Influence: Midwest Clinic, Thursday, December 17 12:00-1:00pmAlex MoralesNo ratings yet
- Preschool ADHD QuestionnaireDocument2 pagesPreschool ADHD QuestionnaireAnnaNo ratings yet
- The Impact of Interest Rates On Economic Growth in KenyaDocument41 pagesThe Impact of Interest Rates On Economic Growth in KenyaSAMUEL KIMANINo ratings yet
- Haven, Quantum Social ScienceDocument306 pagesHaven, Quantum Social ScienceMichael H. HejaziNo ratings yet
- ASTM G 38 - 73 r95Document7 pagesASTM G 38 - 73 r95Samuel EduardoNo ratings yet
- Chapter 5Document42 pagesChapter 5Hong AnhNo ratings yet
- Creative 2nd QuarterDocument6 pagesCreative 2nd QuarterJanice CordovaNo ratings yet
- Underwater vessels, sensors, weapons and control systemsDocument1 pageUnderwater vessels, sensors, weapons and control systemsNguyễn ThaoNo ratings yet
- Abstract & Concrete NounsDocument2 pagesAbstract & Concrete NounsSitifatimah92No ratings yet
- Karsten Fatur - "Sagas of The Solanaceae: Speculative Ethnobotanical Perspectives On The Norse Berserkers" (2019)Document8 pagesKarsten Fatur - "Sagas of The Solanaceae: Speculative Ethnobotanical Perspectives On The Norse Berserkers" (2019)Before AfterNo ratings yet
- 1-Knowledge Assurance SM PDFDocument350 pages1-Knowledge Assurance SM PDFShahid MahmudNo ratings yet
- Business LetterDocument196 pagesBusiness LetterNulaNo ratings yet
- Pharmaceutical and Software Development ProjectsDocument6 pagesPharmaceutical and Software Development ProjectsAlexandar123No ratings yet
- ATPL theory summary formulas and guidelines (40 charactersDocument60 pagesATPL theory summary formulas and guidelines (40 charactersJonas Norvidas50% (2)
- Exploratory Factor AnalysisDocument170 pagesExploratory Factor AnalysisSatyabrata Behera100% (7)
- Attendance: Umut KurtoğluDocument2 pagesAttendance: Umut KurtoğluHavvaNo ratings yet
- Analisis Semiotika Pada Cover Novel Trilogi Karya Vira SafitriDocument9 pagesAnalisis Semiotika Pada Cover Novel Trilogi Karya Vira SafitridedydoankNo ratings yet
- LOGIK Fridge Freezer With Water Dispenser LSD55W18 ManualDocument20 pagesLOGIK Fridge Freezer With Water Dispenser LSD55W18 Manualfbunt2777No ratings yet
- Lauren Tarshis - (I Survived 05) - I Survived The San Francisco Earthquake, 1906Document66 pagesLauren Tarshis - (I Survived 05) - I Survived The San Francisco Earthquake, 1906Olga de Ramos100% (1)
- Communalism in India - Causes, Incidents and MeasuresDocument5 pagesCommunalism in India - Causes, Incidents and Measures295Sangita PradhanNo ratings yet
- Lecture Notes in Computer Science-7Document5 pagesLecture Notes in Computer Science-7Arun SasidharanNo ratings yet
- Past Simple Past ContinuousDocument2 pagesPast Simple Past ContinuousEsmeralda Gonzalez80% (5)
- Y10 ICT End of TermDocument7 pagesY10 ICT End of TermIvy Atuhairwe BisoborwaNo ratings yet
- UT Dallas Syllabus For Se2370.501 05s Taught by Weichen Wong (Wew021000)Document1 pageUT Dallas Syllabus For Se2370.501 05s Taught by Weichen Wong (Wew021000)UT Dallas Provost's Technology GroupNo ratings yet
- Does Cash App Have Business Accounts - Google SeaDocument1 pageDoes Cash App Have Business Accounts - Google SeaAdedayo CrownNo ratings yet
- TM Journal Class 5 Pharma Trademarks 2018Document1,192 pagesTM Journal Class 5 Pharma Trademarks 2018Tahir LabbeNo ratings yet
- Innovative Lp1 BlogDocument5 pagesInnovative Lp1 BlogArya ElizabethNo ratings yet
- 14-01 Lista de Laptops - DistribuidoresDocument29 pages14-01 Lista de Laptops - DistribuidoresInkil Orellana TorresNo ratings yet
- TZMmanual PDFDocument8 pagesTZMmanual PDFccardenas3907No ratings yet