You might also like
- ClaimForm PDFDocument1 pageClaimForm PDFSameer MandgeNo ratings yet
- Practical 5 JKKP Form 7 Ve - jkkp7 Report of OccD OccPoisoning EngDocument2 pagesPractical 5 JKKP Form 7 Ve - jkkp7 Report of OccD OccPoisoning EngAyub KasyfiNo ratings yet
- Domiciliary Claim Form (Employee Id: 382470) Claim No: D0602190382470A003Document1 pageDomiciliary Claim Form (Employee Id: 382470) Claim No: D0602190382470A003Anonymous Yw2XhfXvNo ratings yet
- Mediassist Claim FormDocument5 pagesMediassist Claim FormsureshNo ratings yet
- eSickLeaveCertificate 10668363972Document1 pageeSickLeaveCertificate 10668363972chemical SectionNo ratings yet
- Attachment RQ4355503 Online Requisition FormDocument1 pageAttachment RQ4355503 Online Requisition FormGenetic Clinic UKMNo ratings yet
- ContentDocument1 pageContentST ANNE GENERAL HOSPITAL INC (SAFETY DEPARTMENT)No ratings yet
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationGoutam HotaNo ratings yet
- Pre-Hospitalisation Claim Form (Employee Id: 915438) Claim No: H0507160915438A002Document1 pagePre-Hospitalisation Claim Form (Employee Id: 915438) Claim No: H0507160915438A002Yogesh ChhaprooNo ratings yet
- Domiciliary Claim Form (Employee Id: 399184) Claim No: D0407170399184E002Document1 pageDomiciliary Claim Form (Employee Id: 399184) Claim No: D0407170399184E002Parag IOTETNo ratings yet
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationNitin FardeNo ratings yet
- 20210308-0043-B Lur No.: Laboratory / Radiology / Ultrasound Request FormDocument1 page20210308-0043-B Lur No.: Laboratory / Radiology / Ultrasound Request FormMarvin VerdadNo ratings yet
- 3-Gmc Claim Form HDFC ErgoDocument3 pages3-Gmc Claim Form HDFC ErgoDT worldNo ratings yet
- Med CC Appln - 126 01082019Document4 pagesMed CC Appln - 126 01082019Gireesh Kumar AllaNo ratings yet
- Medical Reimbursemen APPLICATION SETDocument5 pagesMedical Reimbursemen APPLICATION SETLeelakrishna GvNo ratings yet
- NFC Chss 01 2022 1510Document4 pagesNFC Chss 01 2022 1510srihariNo ratings yet
- Refferalform1Document1 pageRefferalform1ikshikachristian2000No ratings yet
- Employee's State Insurance Corporation: Patient RegistrationDocument2 pagesEmployee's State Insurance Corporation: Patient RegistrationafakraipurNo ratings yet
- JKKP 7Document1 pageJKKP 7SwanBellaNo ratings yet
- 1597040657146-OPF Form CovertDocument4 pages1597040657146-OPF Form Covertmehrotraprashant06No ratings yet
- Medical Claim Form: If The Claim Amount Is More Then Rs 800 Please Attach Prescription of Doctor / PhysicianDocument1 pageMedical Claim Form: If The Claim Amount Is More Then Rs 800 Please Attach Prescription of Doctor / PhysicianZaheer Ahmed TanoliNo ratings yet
- Bajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdDocument2 pagesBajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdvkbasavaNo ratings yet
- Medical Reimbursement Claim Form For Outdoor TreatmentDocument1 pageMedical Reimbursement Claim Form For Outdoor TreatmentHimanshu YadavNo ratings yet
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDocument1 pageThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesRajesh KumarNo ratings yet
- 02022019BB0009R PDFDocument1 page02022019BB0009R PDFRajesh KumarNo ratings yet
- Reliance Health Claim FormDocument4 pagesReliance Health Claim FormarijitnirmalNo ratings yet
- Referral Letter: Employees State Insurance CorporationDocument1 pageReferral Letter: Employees State Insurance CorporationafakraipurNo ratings yet
- ClaimFormDocument1 pageClaimFormankit ojhaNo ratings yet
- Domiciliary Claim Form (Employee Id: 1100156) Claim No: D3105201100156E001Document1 pageDomiciliary Claim Form (Employee Id: 1100156) Claim No: D3105201100156E001Biswajit DattaNo ratings yet
- Group Mediclaim - Associate, Family & Parents Tracking No: H150420191046544383Document1 pageGroup Mediclaim - Associate, Family & Parents Tracking No: H150420191046544383rameshNo ratings yet
- Medical Reimbursement Claim FormDocument2 pagesMedical Reimbursement Claim Formaftabs07No ratings yet
- Iffco-Tokio General Insurance Company LimitedDocument1 pageIffco-Tokio General Insurance Company LimitedakshatmalhotraNo ratings yet
- Philippine Charity Sweepstakes OfficeDocument1 pagePhilippine Charity Sweepstakes OfficeRandy Ramos FloresNo ratings yet
- ReimbursementDocument1 pageReimbursementraviNo ratings yet
- 769-Phy 065936 PDFDocument1 page769-Phy 065936 PDF9NDRF HOSPNo ratings yet
- Reimbursement Claim Form Employee (In BLOCK Letters)Document6 pagesReimbursement Claim Form Employee (In BLOCK Letters)Navneet SinghNo ratings yet
- Claim Form - OPD TreatmentDocument2 pagesClaim Form - OPD Treatmentsovan kumar pattasaniNo ratings yet
- Appendix-Ii Application For Claiming Refund of Medical Expenses Incurred in Connection On With Medical Attendance and or Treatment of Government Servant and Their FamiliesDocument1 pageAppendix-Ii Application For Claiming Refund of Medical Expenses Incurred in Connection On With Medical Attendance and or Treatment of Government Servant and Their FamiliesVinay TataNo ratings yet
- GsisDocument3 pagesGsisPecu MT ProvinceNo ratings yet
- Medical ReumbercementDocument21 pagesMedical ReumbercementSatish HMNo ratings yet
- Federal Staff Relief Fund FormDocument1 pageFederal Staff Relief Fund Formkazmi_jeNo ratings yet
- Pramod Chandrakant VairatDocument3 pagesPramod Chandrakant VairatDipak ShelkeNo ratings yet
- Giri DharDocument1 pageGiri Dharpavanyagatigmail.com laxmibhaskarrakshithNo ratings yet
- Medical Report Application: Jabatan Rekod Perubatan Hospital PutrajayaDocument2 pagesMedical Report Application: Jabatan Rekod Perubatan Hospital PutrajayahaasviniNo ratings yet
- Book No MLC No Hospital NameDocument6 pagesBook No MLC No Hospital NameUmair KhaliqNo ratings yet
- Shahid Nijam ShaikhDocument3 pagesShahid Nijam ShaikhDipak ShelkeNo ratings yet
- Job Appli From SabahDocument4 pagesJob Appli From SabahNurshaziana Mohd SalahudinNo ratings yet
- I Personal Particulars: Medical Examination ReportDocument1 pageI Personal Particulars: Medical Examination ReportRahmatul LailiNo ratings yet
- Lonpac Maid Medical ClaimDocument3 pagesLonpac Maid Medical ClaimYl EdianonNo ratings yet
- Transfers ApplicationDocument2 pagesTransfers Applicationganesh.pabbisettyNo ratings yet
- Santosh Subhash KindreDocument3 pagesSantosh Subhash KindreDipak ShelkeNo ratings yet
- Ioacon Registration Format Doctor Details: Sr. No Division Region HQ PSO Name Title (DR)Document13 pagesIoacon Registration Format Doctor Details: Sr. No Division Region HQ PSO Name Title (DR)Debangshu KumarNo ratings yet
- Report ViewerDocument1 pageReport ViewerHamid HassanNo ratings yet
- Hospitalisation Claim Form: Borang Tuntutan HospitalDocument2 pagesHospitalisation Claim Form: Borang Tuntutan HospitalMohd Azizee Bin SukorNo ratings yet
- Honorary Application Form 2021ppp0Document15 pagesHonorary Application Form 2021ppp0fidhaNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceVasudevan KunjithapathamNo ratings yet
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationGoutam HotaNo ratings yet
- Medical Reimbursemet PrintDocument1 pageMedical Reimbursemet Printdaviduecw12No ratings yet
- Yu, Rachelle B. Jd-Ii: Labor LawDocument3 pagesYu, Rachelle B. Jd-Ii: Labor Lawjolina cumpioNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- GRP4Integrated Application Form XLSX FormatDocument15 pagesGRP4Integrated Application Form XLSX FormatIsabel PeraltaNo ratings yet
- Functionality of Barangay Anti-Drug Abuse Council: Its Roles and Responsibilities Under Dilg Memorandum Circular No. 2015-66Document21 pagesFunctionality of Barangay Anti-Drug Abuse Council: Its Roles and Responsibilities Under Dilg Memorandum Circular No. 2015-66Angelie Regie J EstorqueNo ratings yet
- Ipe - Neuro - Kelompok 8aDocument20 pagesIpe - Neuro - Kelompok 8aHanis NandaNo ratings yet
- Medical Writing Jobs - EssayDocument1 pageMedical Writing Jobs - EssayRoselily Flores CoquillaNo ratings yet
- Nursing Care Plan (NCP) 6 SCORES: Patient-Centered (In Priority Order)Document2 pagesNursing Care Plan (NCP) 6 SCORES: Patient-Centered (In Priority Order)WorodNo ratings yet
- Dir ListDocument8 pagesDir ListelclareanoNo ratings yet
- Pemerintah Kota Depok Dinas Pendidikan Dan Kebudayaan Unit Pelayanan Teknis SMK Insan Aqilah 3 Sawangan DepokDocument3 pagesPemerintah Kota Depok Dinas Pendidikan Dan Kebudayaan Unit Pelayanan Teknis SMK Insan Aqilah 3 Sawangan Depokaden galangNo ratings yet
- Rod of AsclepiusDocument8 pagesRod of AsclepiusMulya EchaNo ratings yet
- CP-07 Workflow For Daycare Ambulatory CareDocument1 pageCP-07 Workflow For Daycare Ambulatory CareNatasha BhasinNo ratings yet
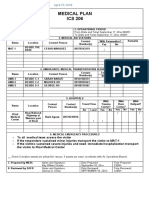
- Ics 206Document1 pageIcs 206Ldrrmo RamonNo ratings yet
- Physical Stability and Activity of Cream W/O Etanolik Fruit EXTRACT MAHKOTA DEWA (Phaleria Macrocarph (Scheff.) Boerl,) AS A SunscreenDocument9 pagesPhysical Stability and Activity of Cream W/O Etanolik Fruit EXTRACT MAHKOTA DEWA (Phaleria Macrocarph (Scheff.) Boerl,) AS A SunscreenNur RohmahNo ratings yet
- Doble, Adam - Martin, Ian L. - Nutt, David J - Calming The Brain Benzodiazepines and Related Drugs From Laboratory To Clinic-CRC Press (2020)Document192 pagesDoble, Adam - Martin, Ian L. - Nutt, David J - Calming The Brain Benzodiazepines and Related Drugs From Laboratory To Clinic-CRC Press (2020)Priscielly Marcelo CristovãoNo ratings yet
- Afp Case Investigation FormDocument3 pagesAfp Case Investigation Formአብይ በላይነሽ ጥላሁንNo ratings yet
- List Pengadaan Obat Apotek BaruDocument11 pagesList Pengadaan Obat Apotek Barudea angguniaNo ratings yet
- Cranial Nerves AssessmentDocument3 pagesCranial Nerves AssessmentNursesLabs.comNo ratings yet
- Ental Echnology: Direct Core Buildup Using A Preformed Crown and Prefabricated Zirconium Oxide PostDocument3 pagesEntal Echnology: Direct Core Buildup Using A Preformed Crown and Prefabricated Zirconium Oxide PostSudhanshu Kumar KashyapNo ratings yet
- Padmaja Devi - FEMALE - 62 Yrs APJ1.0013308310 1779459Document2 pagesPadmaja Devi - FEMALE - 62 Yrs APJ1.0013308310 1779459John DaveNo ratings yet
- CTK Products at A Glance Rev 7.0Document2 pagesCTK Products at A Glance Rev 7.0peter marcoNo ratings yet
- Gambaran Kejadian Medication Error Di Instalasi Gawat Darurat Rsu Elim RantepaoDocument7 pagesGambaran Kejadian Medication Error Di Instalasi Gawat Darurat Rsu Elim RantepaoRahmi Eka PutriNo ratings yet
- Alps-Our Recent Projects and List of Clients - 2022Document2 pagesAlps-Our Recent Projects and List of Clients - 2022Alps EngineeringNo ratings yet
- All in One...Document261 pagesAll in One...Dr. Mahmoud Tawfik ElSorady100% (1)
- Vikram Covid Vaccine Certificate1666801329239Document1 pageVikram Covid Vaccine Certificate1666801329239DR nagar gamerNo ratings yet
- Hiro System Procedure PDFDocument8 pagesHiro System Procedure PDFsnehaNo ratings yet
- Artic - NEJM - Tricomicosis Axilaris - 2022Document1 pageArtic - NEJM - Tricomicosis Axilaris - 2022Michelle OlveraNo ratings yet
- A. Establishing A Relationship.: Read The Following Dialog and Answer The Questions !Document10 pagesA. Establishing A Relationship.: Read The Following Dialog and Answer The Questions !lisaNo ratings yet
- Rangs Childrens Fractures (3rd Edition) PDFDocument326 pagesRangs Childrens Fractures (3rd Edition) PDFairbear1115No ratings yet
- Question Bank: ESSAY ONE - Theme: EducationDocument3 pagesQuestion Bank: ESSAY ONE - Theme: EducationCELL IELTSNo ratings yet
- Rishita HealthcareDocument10 pagesRishita HealthcareloyaoviNo ratings yet
- Catheterization: NCM 107 LabDocument4 pagesCatheterization: NCM 107 LabCatherine PradoNo ratings yet
- MedicineDocument12 pagesMedicineaksonarain1 23No ratings yet