You might also like
- The Body Keeps The Score: Brain, Mind, and Body in The Healing of Trauma - Bessel Van Der Kolk M.D.Document4 pagesThe Body Keeps The Score: Brain, Mind, and Body in The Healing of Trauma - Bessel Van Der Kolk M.D.xutagybu6% (198)
- The Body Keeps The ScoreDocument52 pagesThe Body Keeps The ScoreMichele Cosi100% (1)
- Mind Over Mood Change How You Feel by CH PDFDocument6 pagesMind Over Mood Change How You Feel by CH PDFRoaida Meen6% (17)
- It Didn't Start With You: How Inherited Family Trauma Shapes Who We Are and How To End The Cycle - Mark WolynnDocument4 pagesIt Didn't Start With You: How Inherited Family Trauma Shapes Who We Are and How To End The Cycle - Mark Wolynnxezodapy7% (152)
- Preview of How To Be An Adult A Handbook For Psychological and Spiritual IntegrationDocument10 pagesPreview of How To Be An Adult A Handbook For Psychological and Spiritual Integrationmillywanilly50% (2)
- It Didn't Start ....Document16 pagesIt Didn't Start ....tigerlo7513% (53)
- The Two Million Year Old SelfDocument163 pagesThe Two Million Year Old Selfoftaran100% (20)
- Daring Greatly: How The Courage To Be Vulnerable Transforms The Way We Live, Love, Parent, and Lead - Brené BrownDocument5 pagesDaring Greatly: How The Courage To Be Vulnerable Transforms The Way We Live, Love, Parent, and Lead - Brené Brownxygujiji0% (16)
- Scared SickDocument320 pagesScared SickChapali100% (5)
- Welding SymbolsDocument8 pagesWelding SymbolsRaoFarhan100% (1)
- WellermanDocument2 pagesWellermanIsa100% (7)
- The Child in You - Stefanie StahlDocument222 pagesThe Child in You - Stefanie StahlVi Ha100% (9)
- Compassionate Inquiry Gabor MateDocument6 pagesCompassionate Inquiry Gabor MateIoana100% (2)
- Guide to Bessel van der Kolk's, MD The Body Keeps the ScoreFrom EverandGuide to Bessel van der Kolk's, MD The Body Keeps the ScoreRating: 4.5 out of 5 stars4.5/5 (12)
- 11xe Science of ConsciousnessDocument6 pages11xe Science of ConsciousnessInes De CastroNo ratings yet
- Summary of Mark Wolynn's It Didn't Start with YouFrom EverandSummary of Mark Wolynn's It Didn't Start with YouRating: 4.5 out of 5 stars4.5/5 (13)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma | A Guide To Bessel van der Kolk's BookFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma | A Guide To Bessel van der Kolk's BookNo ratings yet
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (252)
- Simple Fancy - Two Raw SistersDocument5 pagesSimple Fancy - Two Raw SistersAllen & UnwinNo ratings yet
- Emotions Revealed by Paul Ekman1 PDFDocument285 pagesEmotions Revealed by Paul Ekman1 PDFAlexandru Ivan100% (2)
- Presence: Bringing Your Boldest Self To Your Biggest Challenges - Amy CuddyDocument4 pagesPresence: Bringing Your Boldest Self To Your Biggest Challenges - Amy Cuddygirewote0% (8)
- Healing Traumatic Reenactment - Wheatley-CrosbieDocument10 pagesHealing Traumatic Reenactment - Wheatley-CrosbieYuldashNo ratings yet
- Bromberg Standing in The SpacesDocument24 pagesBromberg Standing in The SpacesTiberiuNo ratings yet
- Summary of Bruce D. Perry and Maya Szalavitz's The Boy Who Was Raised as a DogFrom EverandSummary of Bruce D. Perry and Maya Szalavitz's The Boy Who Was Raised as a DogRating: 2 out of 5 stars2/5 (1)
- Yes To Life in Spite of Everything - HolocaustDocument5 pagesYes To Life in Spite of Everything - HolocausthixadacoNo ratings yet
- SIGMUND FREUD Ultimate Collection: Psychoanalytic Studies, Theoretical Essays & Articles: The Interpretation of Dreams, Psychopathology of Everyday Life, Dream Psychology, Three Contributions to the Theory of Sex, Beyond the Pleasure Principle, Totem and Taboo, Leonardo da Vinci…From EverandSIGMUND FREUD Ultimate Collection: Psychoanalytic Studies, Theoretical Essays & Articles: The Interpretation of Dreams, Psychopathology of Everyday Life, Dream Psychology, Three Contributions to the Theory of Sex, Beyond the Pleasure Principle, Totem and Taboo, Leonardo da Vinci…No ratings yet
- The Collected Works of Sigmund Freud: The Interpretation of Dreams, Psychopathology of Everyday Life, Dream PsychologyFrom EverandThe Collected Works of Sigmund Freud: The Interpretation of Dreams, Psychopathology of Everyday Life, Dream PsychologyNo ratings yet
- Into the Abyss: A neuropsychiatrist's notes on troubled mindsFrom EverandInto the Abyss: A neuropsychiatrist's notes on troubled mindsRating: 4 out of 5 stars4/5 (9)
- What Happened To You? Conversations On Trauma, Resilience, and HealingDocument3 pagesWhat Happened To You? Conversations On Trauma, Resilience, and HealingRares Apastasoaiei50% (2)
- Trauma and Faith, Reading The Narrative of The Hemorrhaging WomanDocument26 pagesTrauma and Faith, Reading The Narrative of The Hemorrhaging WomanXiaxia Xue100% (1)
- SPE 153072 Production Data Analysis in Eagle Ford Shale Gas ReservoirDocument0 pagesSPE 153072 Production Data Analysis in Eagle Ford Shale Gas ReservoirFernando Montes de OcaNo ratings yet
- Commentary A Beautiful MindDocument2 pagesCommentary A Beautiful MindJosefina100% (1)
- The Disease To Please (Uncovering Our Mask)Document4 pagesThe Disease To Please (Uncovering Our Mask)Oladiran InnioluwaNo ratings yet
- Help For The Helper: The Psychophysiology of Compassion Fatigue and Vicarious Trauma - Babette RothschildDocument4 pagesHelp For The Helper: The Psychophysiology of Compassion Fatigue and Vicarious Trauma - Babette Rothschildrizozoxy0% (3)
- Anthony Stevens - The Two Million-Year-Old Self PDFDocument80 pagesAnthony Stevens - The Two Million-Year-Old Self PDFCiprian Cătălin Alexandru0% (1)
- Psychological DisordersDocument48 pagesPsychological DisordersBrian WuNo ratings yet
- The Collected Works of Sigmund Freud: Psychoanalytical Studies, Articles & Theoretical EssaysFrom EverandThe Collected Works of Sigmund Freud: Psychoanalytical Studies, Articles & Theoretical EssaysNo ratings yet
- Landslide Contingency Plan (Final) PDFDocument36 pagesLandslide Contingency Plan (Final) PDFRodgelyn Francisco100% (6)
- OPT B2 Unit Test 8 StandardDocument6 pagesOPT B2 Unit Test 8 StandardPopa PatriciaNo ratings yet
- Positively Misguided: The Myths & Mistakes of The Positive Thinking Movement. by Steve SalernoDocument9 pagesPositively Misguided: The Myths & Mistakes of The Positive Thinking Movement. by Steve SalernoevanLeNo ratings yet
- Complexes ArchetypesDocument8 pagesComplexes ArchetypesPsicologia e ReflexõesNo ratings yet
- Psychophysiological Study of Out-of-the-Body Experiences in A Selected SubjectDocument7 pagesPsychophysiological Study of Out-of-the-Body Experiences in A Selected SubjectIno MoxoNo ratings yet
- How Psychics Cope With Hearing Voices Could Help People With Psychotic Disorders - The AtlanticDocument14 pagesHow Psychics Cope With Hearing Voices Could Help People With Psychotic Disorders - The Atlanticpujarze2No ratings yet
- The Collected Works of Sigmund Freud: Psychoanalytic Studies, Theoretical Essays & Articles: The Interpretation of Dreams, Psychopathology of Everyday Life, Dream Psychology, Three Contributions to the Theory of Sex, The History of the Psychoanalytic Movement, Leonardo da Vinci…From EverandThe Collected Works of Sigmund Freud: Psychoanalytic Studies, Theoretical Essays & Articles: The Interpretation of Dreams, Psychopathology of Everyday Life, Dream Psychology, Three Contributions to the Theory of Sex, The History of the Psychoanalytic Movement, Leonardo da Vinci…Rating: 3 out of 5 stars3/5 (1)
- What Near-Death Experiences Reveal About The BrainDocument11 pagesWhat Near-Death Experiences Reveal About The BraindiegoNo ratings yet
- Rhetorical Analysis EssayDocument5 pagesRhetorical Analysis Essayapi-746633505No ratings yet
- Reflections On Women, Depression, and The Soul-Image: by Karen HodgesDocument36 pagesReflections On Women, Depression, and The Soul-Image: by Karen HodgesAndrew HartmanNo ratings yet
- The Psychodynamics of Psychosis: ArticleDocument8 pagesThe Psychodynamics of Psychosis: ArticleGabriela ComanescuNo ratings yet
- Borderline and PTSDDocument11 pagesBorderline and PTSDContención Emocional CIASNo ratings yet
- Is Life After Death Possible?: Written By: Scott Mendelson, M. D. (Author of Beyond Alzheimer)Document5 pagesIs Life After Death Possible?: Written By: Scott Mendelson, M. D. (Author of Beyond Alzheimer)IVy Michelle BunganNo ratings yet
- The Fault in Our Stars PaperDocument9 pagesThe Fault in Our Stars Paperapi-490173413No ratings yet
- Freud'sDocument8 pagesFreud'sZahraa QahtanNo ratings yet
- Tart 1978eDocument7 pagesTart 1978eIno MoxoNo ratings yet
- Psychoanalytics Behind Bacatan'S "Smaller and Smaller Circles"Document13 pagesPsychoanalytics Behind Bacatan'S "Smaller and Smaller Circles"Miggy MirandaNo ratings yet
- Brain Stains Scientific American Mind, Vol 18, Issue 5 2007Document8 pagesBrain Stains Scientific American Mind, Vol 18, Issue 5 2007Ming ThắngNo ratings yet
- A Tale of Mental Illness by Elyn SaksDocument6 pagesA Tale of Mental Illness by Elyn SaksAnalia WriterNo ratings yet
- Sigmund Freud: Collected Works: Psychoanalytic Studies, Essays & Articles: The Interpretation of Dreams, Dream Psychology…From EverandSigmund Freud: Collected Works: Psychoanalytic Studies, Essays & Articles: The Interpretation of Dreams, Dream Psychology…No ratings yet
- Usa Bergler 10Document8 pagesUsa Bergler 10andres19712No ratings yet
- Summary of The Body Keeps The Score: Brain, Mind, and Body in the Healing of Trauma- A Guide To Bessel Van der Kolk's BookFrom EverandSummary of The Body Keeps The Score: Brain, Mind, and Body in the Healing of Trauma- A Guide To Bessel Van der Kolk's BookNo ratings yet
- Slide 1Document4 pagesSlide 1api-233454550No ratings yet
- Vol13 No1 5Document19 pagesVol13 No1 5man cuiNo ratings yet
- PBS Baits E - Book Version 1Document48 pagesPBS Baits E - Book Version 1Dirk Henn0% (1)
- The Names We BearDocument246 pagesThe Names We BearBob ChaffeeNo ratings yet
- Cardiac Anatomy and PhysiologyDocument2 pagesCardiac Anatomy and PhysiologyKarina YurchenkoNo ratings yet
- Download: Chanakya Arthashastra Telugu PDF Free Download HitDocument2 pagesDownload: Chanakya Arthashastra Telugu PDF Free Download HitWik ÀzNo ratings yet
- PotatoDocument29 pagesPotatoenzo abrahamNo ratings yet
- Urtec 2020 2581 MsDocument18 pagesUrtec 2020 2581 MsAlejandro MonroyNo ratings yet
- Architectural Acoustics Assignment - 5Document5 pagesArchitectural Acoustics Assignment - 5SharanyaNo ratings yet
- CVM-NRG96: Power AnalyzerDocument38 pagesCVM-NRG96: Power AnalyzerDepto SandhyNo ratings yet
- Legaledge Classroom Handout: Current AffairsDocument4 pagesLegaledge Classroom Handout: Current AffairsHarsh SrivastavaNo ratings yet
- MinerologyDocument38 pagesMinerologyGOPALNo ratings yet
- Virologyintro 180422150307 PDFDocument30 pagesVirologyintro 180422150307 PDFSam AbuGhozie AhmadinovNo ratings yet
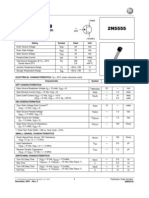
- 2n5555 JfetDocument9 pages2n5555 JfetRamon CubillaNo ratings yet
- UHSAA Preparticipation FormDocument4 pagesUHSAA Preparticipation FormThe Salt Lake TribuneNo ratings yet
- Ramanan M: ObjectiveDocument3 pagesRamanan M: ObjectiveRamanan MNo ratings yet
- Experiment 2 The P-N Junction. DiodesDocument5 pagesExperiment 2 The P-N Junction. DiodesIrene SarpongNo ratings yet
- CY7C64215Document33 pagesCY7C64215rocky liuNo ratings yet
- 1570741459076Document1 page1570741459076Josué JuárezNo ratings yet
- TECH NINJO EN RevBDocument54 pagesTECH NINJO EN RevBMoreno TittarelliNo ratings yet
- Come Let Us Worship/ O Come Let Us Adore HimDocument3 pagesCome Let Us Worship/ O Come Let Us Adore HimdecidophobicNo ratings yet
- Maj Michael Hemker U. S. Army Dental Corps: Comprehensive DentistryDocument101 pagesMaj Michael Hemker U. S. Army Dental Corps: Comprehensive DentistryVincent ReyesNo ratings yet
- Group No 7 - Kingfisher AirlinesDocument10 pagesGroup No 7 - Kingfisher AirlinesPankaj SinghNo ratings yet
- Plating - Interpharm PDFDocument4 pagesPlating - Interpharm PDFvasudev_nNo ratings yet
- CH3340E - Lab Report - 20202-đã chuyển đổiDocument34 pagesCH3340E - Lab Report - 20202-đã chuyển đổiThắng Linh NguyễnNo ratings yet
- Verdad® Clean Label Antimicrobials For Meat & Culiinary: Opportunities & ChallengesDocument14 pagesVerdad® Clean Label Antimicrobials For Meat & Culiinary: Opportunities & ChallengesAjeng KurniasihNo ratings yet