You might also like
- New Vet Jumpstart Guide: Twenty common general practice cases simplifiedFrom EverandNew Vet Jumpstart Guide: Twenty common general practice cases simplifiedNo ratings yet
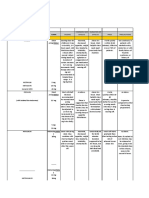
- Medication ChartDocument6 pagesMedication ChartMax ImoNo ratings yet
- Risperidone - Drug Information - UpToDateDocument81 pagesRisperidone - Drug Information - UpToDateEduardo AguilarNo ratings yet
- Pediatric Intake:: Suggested DosingDocument2 pagesPediatric Intake:: Suggested DosingcarlosenriqueaaNo ratings yet
- Dudley Dementia Prescribing Guidance Final 1626174181Document9 pagesDudley Dementia Prescribing Guidance Final 1626174181Abdualaziz AlmalkiNo ratings yet
- Neuropathic Pain TreatmentDocument8 pagesNeuropathic Pain TreatmentIrimes MariaNo ratings yet
- bpj18 Methadone PageDocument6 pagesbpj18 Methadone PageJaesen TameleNo ratings yet
- ADHD Medication Chart 2004Document4 pagesADHD Medication Chart 2004M PatrickNo ratings yet
- Buprenorphine/Suboxone Micro-Initionation Induction While Using Fentanyl (Burnese Method)Document23 pagesBuprenorphine/Suboxone Micro-Initionation Induction While Using Fentanyl (Burnese Method)Hunter J. WadeNo ratings yet
- Ranitidine - 1aDocument5 pagesRanitidine - 1aRichard OonNo ratings yet
- Drug Study CNS StimulantsDocument10 pagesDrug Study CNS StimulantsJames Emman ClementeNo ratings yet
- Methylphenidate Card#6Document2 pagesMethylphenidate Card#6USMCDOCNo ratings yet
- Pcal Lab NotesDocument21 pagesPcal Lab NotesJerome Delos ReyesNo ratings yet
- Immediate Release - (Methylphenidate)Document4 pagesImmediate Release - (Methylphenidate)MaryNguyenNo ratings yet
- PocketGuide FINAL6 PDFDocument2 pagesPocketGuide FINAL6 PDFSolomon Seth SallforsNo ratings yet
- FAQ Drug Info - TirzepatideDocument9 pagesFAQ Drug Info - Tirzepatideraea.dobsonNo ratings yet
- Desipramine Drug Information - UpToDateDocument32 pagesDesipramine Drug Information - UpToDateWilliam OmarNo ratings yet
- Stim Adult DosingchartDocument4 pagesStim Adult DosingchartMina JoonNo ratings yet
- Neuropathic Pain Guidance April 2023 v1.2Document6 pagesNeuropathic Pain Guidance April 2023 v1.2Germán Bernate ObandoNo ratings yet
- Drugs That Require Loading Doses Table FinalDocument1 pageDrugs That Require Loading Doses Table Finalandirio7486No ratings yet
- Teicoplanin Dosing and Monitoring in AdultsDocument3 pagesTeicoplanin Dosing and Monitoring in Adultsdps_1976No ratings yet
- Adapted From CDC Guideline: Assess Pain & FunctionDocument2 pagesAdapted From CDC Guideline: Assess Pain & FunctionSolomon Seth SallforsNo ratings yet
- Tuberculosis Treatment GuidelinesDocument2 pagesTuberculosis Treatment GuidelinesMaverick CaoileNo ratings yet
- MethylphenidateDocument3 pagesMethylphenidateAyhan CiftciNo ratings yet
- Ppolypharmacy 2020 ENsDocument26 pagesPpolypharmacy 2020 ENsRegina PunNo ratings yet
- Domperidone 1Document17 pagesDomperidone 1Miftah Nur AndamsariNo ratings yet
- Niim Hrec Aps MC Dosing GuidelinesDocument1 pageNiim Hrec Aps MC Dosing Guidelinestammy.shattockNo ratings yet
- Buccal Midazolam GuidelineDocument5 pagesBuccal Midazolam GuidelineAnwarrudin AsniNo ratings yet
- Effect DoseDocument30 pagesEffect DoseXyprus Darina VeloriaNo ratings yet
- Loading Doses Primary CareDocument3 pagesLoading Doses Primary CareGalih AsaNo ratings yet
- Alprazolam (Systemic)Document14 pagesAlprazolam (Systemic)RIRINo ratings yet
- Clinical Policy: Modafinil (Provigil) : Revision LogDocument7 pagesClinical Policy: Modafinil (Provigil) : Revision LogGabriel GuimarãesNo ratings yet
- Pediatric Dosage CalculationsDocument5 pagesPediatric Dosage CalculationsLovely Anjenell MacalingaNo ratings yet
- RisperidoneDocument2 pagesRisperidoneIsabella JosephineNo ratings yet
- Generic DrugsDocument5 pagesGeneric DrugsMonica Joeanne A. BullecerNo ratings yet
- Opioid Tapering Flow Sheet: Start HereDocument2 pagesOpioid Tapering Flow Sheet: Start HeregegeNo ratings yet
- Epilepsy Questions 2021Document5 pagesEpilepsy Questions 2021z_sadiqNo ratings yet
- Anti Dementia Drugs: Moderator: Dr. Ramasubbareddy Sir Presenter: Dr. RavikishoreDocument26 pagesAnti Dementia Drugs: Moderator: Dr. Ramasubbareddy Sir Presenter: Dr. RavikishoreKishore SadulaNo ratings yet
- ConcertatabDocument18 pagesConcertatabaliardaozkan8No ratings yet
- Opioid Calculator - For Health Professionals 2021 GP VictoriaDocument3 pagesOpioid Calculator - For Health Professionals 2021 GP VictoriaJonoffski “Mr Sopping Clam”No ratings yet
- Hypothyroidism DrugsDocument3 pagesHypothyroidism DrugsAisha MarieNo ratings yet
- Handy Summary Chart Comparing The Main Medications For PsychosisDocument3 pagesHandy Summary Chart Comparing The Main Medications For Psychosisrowanpurdy100% (2)
- Symph A To Mimetic SDocument27 pagesSymph A To Mimetic Sjl frusaNo ratings yet
- Medication: Dosing: Daily/PRN: NotesDocument2 pagesMedication: Dosing: Daily/PRN: NotesMaryNguyenNo ratings yet
- Methadone Missed DosesDocument3 pagesMethadone Missed DosesGregNo ratings yet
- Drugs For Adult ADHD - UpToDateDocument3 pagesDrugs For Adult ADHD - UpToDateRob LNo ratings yet
- Common Conversions: Methods of CalculationDocument13 pagesCommon Conversions: Methods of CalculationNormala Macabuntal SaripadaNo ratings yet
- V. Norepinephrine &dopamine ReuptakeDocument2 pagesV. Norepinephrine &dopamine ReuptakeChristine Pialan SalimbagatNo ratings yet
- Nardil (Phenelzine Sulfate) Dose, Indications, Adverse Effects, Interactions... FromDocument42 pagesNardil (Phenelzine Sulfate) Dose, Indications, Adverse Effects, Interactions... Fromdo leeNo ratings yet
- Corticosteroid Guidelines PDFDocument6 pagesCorticosteroid Guidelines PDFMariskaNo ratings yet
- Summary of Product Characteristics 1. Name of The Medicinal ProductDocument13 pagesSummary of Product Characteristics 1. Name of The Medicinal Productddandan_2No ratings yet
- Mekanisme Aksi DiazepamDocument4 pagesMekanisme Aksi DiazepamWijaya Kusuma MaheruNo ratings yet
- HaloperidolDocument2 pagesHaloperidolJordhy ReynaldNo ratings yet
- GentamiciniDocument11 pagesGentamiciniBenjie SisonNo ratings yet
- Haloperidol - Drug Information - UpToDate-1Document5 pagesHaloperidol - Drug Information - UpToDate-1Vh TRNo ratings yet
- ABTC Tapering Your Dose DexamethasoneDocument2 pagesABTC Tapering Your Dose DexamethasonehayyatNo ratings yet
- Health Professionals - TDR FAQsDocument2 pagesHealth Professionals - TDR FAQsngwuelizeNo ratings yet
- Drug of ChoiceDocument12 pagesDrug of ChoiceSEIYADU IBRAHIM KNo ratings yet
- Nursing Responsibilities For METRONIDAZOLEDocument1 pageNursing Responsibilities For METRONIDAZOLEIsrael Soria Espero63% (8)
- Scientific Discussion - En.idDocument9 pagesScientific Discussion - En.idassajadda lizikriNo ratings yet
- OET Reading Test - Chronic Fatigue SyndromeDocument11 pagesOET Reading Test - Chronic Fatigue SyndromeOlive GroupNo ratings yet
- Reading Test 5 - Necrotizing FascilitisDocument8 pagesReading Test 5 - Necrotizing FascilitisOlive GroupNo ratings yet
- Reading Test 2 - Diseases of AffluenceDocument9 pagesReading Test 2 - Diseases of AffluenceOlive GroupNo ratings yet
- Reading Test 4 - Paracetamol OverdoseDocument7 pagesReading Test 4 - Paracetamol OverdoseOlive Group0% (1)
- Reading Test 1 - Junior Sports InjuriesDocument18 pagesReading Test 1 - Junior Sports InjuriesOlive GroupNo ratings yet
- Obstetrics Contents TableDocument2 pagesObstetrics Contents TableKareem SadekNo ratings yet
- Almendras - Argumentative EssayDocument4 pagesAlmendras - Argumentative EssayJhon AlmendrasNo ratings yet
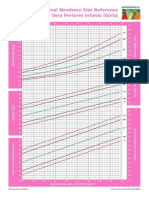
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- 87% of Animals Does Not Have Anti-Rabies Injection: GoalDocument3 pages87% of Animals Does Not Have Anti-Rabies Injection: GoalDan HizonNo ratings yet
- CE 312 - Sewage Disposal in Unsewered Areas PDFDocument9 pagesCE 312 - Sewage Disposal in Unsewered Areas PDFkennysawegNo ratings yet
- Rainwaterguide 2Document2 pagesRainwaterguide 2Ana Bella RosarioNo ratings yet
- Dr. Risa Etika, DR., Spa (K) : ApplicationDocument9 pagesDr. Risa Etika, DR., Spa (K) : ApplicationninaNo ratings yet
- Cot 2 Health 6 - Lesson PlanDocument10 pagesCot 2 Health 6 - Lesson PlanAnna Clarissa TapallaNo ratings yet
- Emilio Jose Plaza Alava Course: 7: Essay-Covid 19 NameDocument2 pagesEmilio Jose Plaza Alava Course: 7: Essay-Covid 19 NameEmilio PlazaNo ratings yet
- Decolonizing International Health - India and Southeast Asia 1930-65 - Amrith (2006)Document276 pagesDecolonizing International Health - India and Southeast Asia 1930-65 - Amrith (2006)shahadat115No ratings yet
- Mitanin Study FINALDocument37 pagesMitanin Study FINALAshok DadasNo ratings yet
- Encyclopedia of WaterDocument966 pagesEncyclopedia of Watersasa.vukoje33% (3)
- Three in A Row A Case Series of Cervical TuberculosisDocument6 pagesThree in A Row A Case Series of Cervical TuberculosisJonelle baloloyNo ratings yet
- Interim Guideline For Prevention and Control of Human Rabies in Malaysia PDFDocument17 pagesInterim Guideline For Prevention and Control of Human Rabies in Malaysia PDFvcweeNo ratings yet
- Kursus Asas Minda Sihat Zon PuduDocument65 pagesKursus Asas Minda Sihat Zon PuduslevsterNo ratings yet
- Etextbook 978 1133599692 Principles and Labs For Physical FitnessDocument61 pagesEtextbook 978 1133599692 Principles and Labs For Physical Fitnessruby.thornley305100% (46)
- Listeriosis PDFDocument3 pagesListeriosis PDFShubhendu ChattopadhyayNo ratings yet
- Factors Associated With Acceptance of Provider-Initiated Hiv Testing and Counseling Among Pregnant Women in EthiopiaDocument9 pagesFactors Associated With Acceptance of Provider-Initiated Hiv Testing and Counseling Among Pregnant Women in EthiopiaSyarifah Radiatul AnnissaNo ratings yet
- Global Manual On Surveillance of AEFIDocument128 pagesGlobal Manual On Surveillance of AEFIHarold JeffersonNo ratings yet
- Toilet Requirement For HospitalDocument2 pagesToilet Requirement For HospitalArjun Chaugule100% (2)
- 2019-20 Coronavirus PandemicDocument80 pages2019-20 Coronavirus PandemicBob LablaNo ratings yet
- NCP Case 1Document6 pagesNCP Case 1boomer SeargeNo ratings yet
- پارتوگرافDocument49 pagesپارتوگرافdr jai gurungNo ratings yet
- PowepoinntDocument7 pagesPowepoinntapi-319343807No ratings yet
- A Sociology of Food and Nutrition by John Germov Lauren Williams (Giped)Document314 pagesA Sociology of Food and Nutrition by John Germov Lauren Williams (Giped)Nurhaerati100% (2)
- Occupational Health and Safety Assessment of The Industries in Bhutan: A Three Years' Trend AnalysisDocument7 pagesOccupational Health and Safety Assessment of The Industries in Bhutan: A Three Years' Trend AnalysisAdvanced Research PublicationsNo ratings yet
- Audio Visual Media For Education of Washing Hands PDFDocument3 pagesAudio Visual Media For Education of Washing Hands PDFastrid berlianNo ratings yet
- Muna Tahlak, MD, FACOG Latifa HospitalDocument44 pagesMuna Tahlak, MD, FACOG Latifa HospitalNur Rahmat Wibowo100% (1)
- Chapter IDocument3 pagesChapter IsophiasaphireNo ratings yet
- COVID 19 HR Action Plan Email Templates - Workable 1Document5 pagesCOVID 19 HR Action Plan Email Templates - Workable 1Gunjan KhuranaNo ratings yet