Professional Documents
Culture Documents
Headache Emergency Medicine
Headache Emergency Medicine
Uploaded by
Mohamed OsmanCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Headache Emergency Medicine
Headache Emergency Medicine
Uploaded by
Mohamed OsmanCopyright:
Available Formats
OCTOBER 2023 | VOLUME 25 | ISSUE 10
Emergency Medicine Practice Evidence-Based Education • Practical Application
CLINICAL CHALLENGES:
• What are the first-line parenteral
treatments for migraine?
• How are nerve blocks for acute
headache pain performed?
• What is the latest evidence on
managing cluster headaches?
• How is medication overuse
headache identified and treated?
Authors
Reema Panjwani, MD
Department of Emergency Medicine;
Montefiore-Einstein Medical Center, Albert
Einstein College of Medicine, Bronx, NY
Amritpal S. Saini, MD
Department of Emergency Medicine;
Montefiore-Einstein Medical Center, Albert
Einstein College of Medicine, Bronx, NY
Maia Winkel, MD
Department of Emergency Medicine;
Evidence-Based Emergency
Montefiore-Einstein Medical Center, Albert
Einstein College of Medicine, Bronx, NY
Department Management
Benjamin Friedman, MD, MS
Professor of Emergency Medicine, Albert
of Migraine and Other
Einstein College of Medicine, Montefiore-
Einstein Medical Center, Bronx, NY
Primary Headaches
Peer Reviewers n Abstract
Headache is the fifth most common presenting chief complaint
David Cherkas, MD, FACEP
Associate Professor of Emergency Medicine, in emergency departments, and it is vital to quickly rule out
Icahn School of Medicine at Mount Sinai, life-threatening secondary causes. Though there are many
New York, NY; Associate Director, Emergency medications, new and old, that can be used to treat primary
Medicine, Elmhurst Hospital Center, Queens, NY headache, the evidence for their effectiveness can be conflicting.
Edward Sloan, MD, MPH, FACEP This review describes the pathology, workup, and treatment
Professor Emeritus, Department of Emergency for migraine and other primary headaches based on the best
Medicine, University of Illinois at Chicago, available evidence, including novel medications, nerve blocks, and
Chicago, IL; Medical Director, Physician Assistant
strategies for preventing postdrome recurrence. Other headache
Studies Program, Dominican University, River
Forest, IL disorders, including cluster headache, medication overuse
headache, and chronic migraine are also reviewed.
Prior to beginning this activity, see “CME
Information” on page 2.
For online For mobile
access: app access:
This issue is eligible for CME credit. See page 2. EBMEDICINE.NET
CME Information
Date of Original Release: October 1, 2023. Date of most recent review: September 10, 2023. Termination date: October 1, 2026.
Accreditation: EB Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide
continuing medical education for physicians.
EVIDENCE-BASED
Credit Designation: EB Medicine designates this enduring material for a maximum of 4 AMA PRA Category 1 CreditsTM. Physi-
cians should claim only the credit commensurate with the extent of their participation in the activity.
PEER-REVIEWED
Specialty CME: Included as part of the 4 credits, this CME activity is eligible for 2 Pharmacology CME credits and 1 Pain Management credit.
ACEP Accreditation: Emergency Medicine Practice is approved by the American College of Emergency Physicians for 48 hours of ACEP Cat-
egory I credit per annual subscription.
AAFP Accreditation: The AAFP has reviewed Emergency Medicine Practice, and deemed it acceptable for AAFP credit. Term of approval is from
07/01/2023 to 06/30/2024. Physicians should claim only the credit commensurate with the extent of their participation in the activity. This session,
Evidence-Based Emergency Department Management of Migraine and Other Primary Headaches is approved for 4.0 enduring material AAFP
Prescribed credits.
AOA Accreditation: Emergency Medicine Practice is eligible for 4 Category 2-B credit hours per issue by the American Osteopathic Association.
Needs Assessment: The need for this educational activity was determined by a practice gap analysis; a survey of medical staff, including the
editorial board of this publication; review of morbidity and mortality data from the CDC, AHA, NCHS, and ACEP; and evaluation responses from
prior educational activities for emergency physicians.
EVIDENCE-BASED
Target Audience: This enduring material is designed for emergency medicine physicians, physician assistants, nurse practitioners, and residents.
Goals: Upon completion of this activity, you should be able to: (1) identify areas in practice that require modification to be consistent with current
evidence in order to improve competence and performance; (2) develop strategies to accurately diagnose and treat both common and critical ED
PEER-REVIEWED
presentations; and (3) demonstrate informed medical decision-making based on the strongest clinical evidence.
CME Objectives: Upon completion of this activity, you should be able to: (1) describe effective parenteral treatments for migraine; (2) perform
the sphenopalatine ganglion nerve block and the greater occipital nerve blocks; (3) discuss management strategies for medication overuse head-
ache; and (4) describe effective treatments for cluster headache.
Discussion of Investigational Information: As part of the activity, faculty may be presenting investigational information about pharmaceutical
products that is outside Food and Drug Administration approved labeling. Information presented as part of this activity is intended solely as
continuing medical education and is not intended to promote off-label use of any pharmaceutical product.
Disclosure: It is the policy of EB Medicine to ensure objectivity, balance, independence, transparency, and scientific rigor in all CME activities.
All individuals in a position to control content have disclosed all financial relationships with ACCME-defined ineligible companies. EB Medicine
has assessed all relationships with ineligible companies disclosed, identified those financial relationships deemed relevant, and appropriately
mitigated all relevant financial relationships based on each individual’s role(s). Please find disclosure information for this activity below:
Planners Faculty
• DanielEVIDENCE-BASED
J. Egan, MD (Course Director): Nothing to Disclose • Reema Panjwani, MD (Author): OrganiGram Holdings, Inc
• Andy Jagoda, MD (Editor-in-Chief): (stocks in publicly traded company)
l Pfizer (Consultant/Advisor) • Amritpal S. Saini, MD (Author): Nothing to Disclose
l
PEER-REVIEWED
Janssen (Consultant/Advisor) • Maia Winkel, MD (Author): Nothing to Disclose
l Abbott Laboratories (Consultant/Advisor) • Benjamin Friedman, MD, MS (Author): Nothing to Disclose
l AstraZeneca (Consultant/Advisor) • David Cherkas, MD (Peer Reviewer): Nothing to Disclose
• Kaushal Shah, MD (Associate Editor-in-Chief): Nothing to Disclose • Edward Sloan, MD, MPH (Peer Reviewer): Nothing to Disclose
• Aimee Mishler, PharmD (Pharmacology Editor): Nothing to Disclose
• Joseph D. Toscano, MD (Research Editor): Nothing to Disclose
• Dorothy Whisenhunt, MS (Content Editor): Nothing to Disclose
• Cheryl Belton, PhD (Content Editor): Nothing to Disclose
Commercial Support: This issue of Emergency Medicine Practice did not receive any commercial support.
Earning CME Credit: Go online to https://www.ebmedicine.net/CME and click on the title of the test you wish to take. When completed, a CME
certificate will be emailed to you.
Additional Policies: For additional policies, including our statement of conflict of interest, source of funding, statement of informed consent, and
statement of human and animal rights, visit https://www.ebmedicine.net/policies
EVIDENCE-BASED
PEER-REVIEWED
Chief Executive Officer: Stephanie Williford Director of Operations: Robin Wilkinson
Publisher: Suzanne Verity Director of Technology: Anna Motuz, MBA
Direct all inquiries to: Director of Editorial Quality: Dorothy Whisenhunt, MS Account Executive: Dana Stenzel
Phone: 678-366-7933 Senior Content Editor: Cheryl Belton, PhD, ELS Marketing Specialist: Joshua Devou, MBA
Fax: 770-500-1316 Managing Editor: Angie Wallace Marketing Specialist: Valerie Yuhouse
5600 Spalding Drive, Unit 921697 CME & Content Coordinator: Kristen Raynor, MEd Education Coordinator: Kandis Slater
Norcross, GA 30010-1697 Editorial Assistant: Lindsay Petracek Customer Service Representative:
E-mail: ebm@ebmedicine.net Database Administrator: Jose Porras Katie Resumovic
Website: www.ebmedicine.net
EVIDENCE-BASED EB Medicine’s Statement on the Use of Artificial Intelligence (AI) Tools in Content Production
At EB Medicine, we produce content for emergency medicine and urgent care clinicians that is evidence-based and peer reviewed,
and at the same time infused with an understanding of the realities of clinical practice, human behavior, and institutional and social
PEER-REVIEWED limitations that only humans can apply. For these reasons, EB Medicine assures our readers and subscribers that all authors of our
content have certified that they have not used generative AI-assisted technology in the writing of their manuscript and that clinical
pathways and images are human-designed. For more information, go to www.ebmedicine.net.org/AI
ISSN information and disclaimer:
Emergency Medicine Practice (ISSN Print: 1524-1971, ISSN Online: 1559-3908, ACID-FREE) is published monthly (12 times per year) by EB Medicine
(5600 Spalding Drive, Unit 921697, Norcross, GA 30010-1697). Opinions expressed are not necessarily those of this publication. Mention of products
or services does not constitute endorsement. This publication is intended as a general guide and is intended to supplement, rather than substitute,
professional judgment. It covers a highly technical and complex subject and should not be used for making specific medical decisions. The materials
contained herein are not intended to establish policy, procedure, or standard of care. Copyright © 2023 EB Medicine. All rights reserved. No part of
this publication may be reproduced in any format without written consent of EB Medicine. This publication is intended for the use of the individual
subscriber only and may not be copied in whole or part or redistributed in any way without the publisher’s prior written permission.
OCTOBER 2023 • www.ebmedicine.net 2 ©2023 EB MEDICINE
Case Presentations
A 36-year woman presents with a pounding left-sided headache associated with nausea that has
persisted for 12 hours…
• She reports having similar headaches about twice monthly, and though they usually resolve with
sumatriptan, she typically visits the ED about once a year for refractory events. This headache
CASE 1
began gradually 12 hours prior and, despite use of oral sumatriptan 100 mg, ibuprofen 800 mg, and
acetaminophen 1000 mg, it has not improved.
• Her physical examination is unremarkable, including normal vital signs, a normal fundoscopic and
visual field examination, and a normal neurologic examination. A point-of-care urine pregnancy test is
negative.
• You administer metoclopramide 10 mg IV and ketorolac 15 mg IV, but she reports only minimal relief.
You wonder what your best next treatment option is…
A 45-year man with a history of infrequent, episodic migraine presents with an unremitting headache
for 1 week…
• He reports an average of 3 severe headaches per year since high school, and they usually resolve
completely with 10 mg oral rizatriptan. For the past 5 months, in association with increased stress at
work, he reports an increase in headache frequency. At first, they were occurring about once per week
CASE 2
and responding to ibuprofen, but over the last month, he has had headaches nearly every day. Initially,
he was getting relief with a combination of 10 mg oral rizatriptan once daily and 800 mg ibuprofen
twice daily, but now these medications are not working at all. His headaches are associated with
photophobia and phonophobia, and they are preventing him from functioning at work.
• His medical history is unremarkable, and the review of systems is otherwise normal. His physical
examination, including vital signs, ophthalmologic, and neurologic examinations are normal.
• You wonder what you can offer him in the ED that might help…
A 53-year woman with migraine presents with a severe headache. She reports a history of 4
headache days per week, which has been going on for more than 10 years...
• She typically manages her headaches with oral eletriptan, naproxen, acetaminophen, Excedrin®
CASE 3
migraine, and a combination butalbital/acetaminophen/caffeine drug. In the past she has been treated
with botulinum toxin injections and oral topiramate. She is typically forced to present to an ED 3 times
per year for management of severe headache, but because she has previously experienced dystonic
reactions, she is reluctant to receive an antidopaminergic medication.
• As you begin your evaluation, she says, “Doc, just give me my Dilaudid.” You can see she is in severe
pain, but you wonder whether giving opioids is the best option in her care…
n Introduction leaves the ED with a better understanding of the
Nearly 5 million emergency department (ED) visits expected course and the range of their treatment
for headache occur in United States annually, options. This issue of Emergency Medicine Practice
making headache the fifth most common chief reviews management strategies for migraine, chronic
complaint that emergency clinicians will encounter.1 migraine, cluster headache, and medication overuse
While emergency clinicians are expert at thoughtful headache, based on the best available evidence.
diagnostic workups, management of headache
can be challenging, particularly when first-line
medications such as nonsteroidal anti-inflammatory n Critical Appraisal of the Literature
drugs (NSAIDs) or antidopaminergic antiemetics are A literature search was performed in PubMed using
not effective. A nuanced understanding of the range the following search terms: (headache or migraine
of headache diagnoses and available treatments can (title)) and (emergency medicine or emergency
help emergency clinicians improve pain outcomes, department) and randomized. This search generated
expedite throughput, and safely avoid expensive, 411 results. From these search results, a list of 63
unnecessary workups. A more precise specific randomized controlled trials (RCTs) and 7 meta-
diagnosis may also benefit the patient who then analyses were selected and used as the basis for
OCTOBER 2023 • www.ebmedicine.net 3 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
most of the management recommendations. Relevant (characterized by temporary paralysis or weakness
clinical policy statements and guidelines from on one side of the body), and retinal migraine
authoritative medical societies were searched, using (characterized by temporary vision loss or blindness
the following PubMed search terms: (headache (title) in 1 eye). Migraine without aura is the most common
or migraine (title)) AND (policy (publication type) type and is usually moderate to severe headache
OR clinical guideline (publication type)). This search pain without the presence of visual or sensory
identified 57 items, of which 4 were also used to symptoms that occur with aura. Migraine with aura
develop recommendations presented here. is characterized by the presence of visual, sensory,
or other neurological symptoms that precede or
accompany the headache. Chronic migraine is
n Etiology And Pathophysiology defined as headache occurring on 15 or more days
When thinking about headache diagnosis, it is per month for at least 3 months, with at least 8 of
best to consider the rubric of the International these days being associated with migraine features.
Classification of Headache Disorders (ICHD).2 The An acute migraine attack typically occurs in 4 of-
ICHD is a comprehensive and authoritative consensus ten overlapping phases: (1) premonitory, (2) aura, (3)
document that describes clinical characteristics, headache, and (4) postdrome. The premonitory phase
symptoms, and diagnostic criteria for every headache can occur as early as 3 days prior to the headache.
diagnosis. The third edition of the International During this phase, patients experience fatigue, yawn-
Classification of Headache Disorders (ICHD-3) lists ing, food cravings, polyuria, irritability, and difficulty
14 types of primary headache disorders. These concentrating. The aura phase generally precedes the
primary headache types include migraine, tension- headache by an hour and consists of reversible neuro-
type headache, trigeminal autonomic cephalalgias logical phenomenon, most typically visual or sensory
(eg, cluster headache and paroxysmal hemicrania), phenomena. The headache itself generally lasts 4 to
and other types of primary headache such as new 72 hours if untreated. The migraine postdrome can
daily persistent headache, hemicrania continua, and last several days, and leaves patients feeling fatigued
primary stabbing headache. In addition to primary and unable to concentrate.5 ED patients report head-
headache disorders, the ICHD-3 also describes aches up to 1 week after the ED visit.6
secondary headache disorders, such as medication Positron emission tomography (PET) and
overuse headache. functional magnetic resonance imaging (MRI) scans
demonstrate a change in the activity of multiple areas
Tension-Type Headache of the brain, including the hypothalamus, brainstem,
Tension-type headache, the most common type of limbic system, and cortex, during the premonitory
primary headache disorder, affects nearly half of the phase of migraines. (See Figure 1, page 5.) The aura
general population, though it is a less common cause phase is characterized by the presence of cortical
of ED visits because, by diagnostic criteria, it is never spreading depression, a slow propagating wave of
severe or functionally impairing. The pathophysiology neuronal and glial depolarization, followed by 30
of tension-type headache is poorly understood but minutes of cortical activity inhibition. Propagation of
is thought to involve activation of peripheral muscu- the wave of depolarization matches the movement
loskeletal tissue-based nociceptors with progression of visual aura through a patient’s field of vision. The
to central nervous system activation and sensitiza- headache is thought to begin in the meninges, where
tion.3 Tension-type headache is typically characterized inflammatory mediators activate the trigeminal nerve.
by bilateral, pressing, or tightening pain of mild to The nociceptive fibers from the trigeminal nerve
moderate intensity that is not aggravated by routine originate from the trigeminal ganglion and end in
physical activity. Tension-type headache may be infre- the trigeminal cervical complex in the brainstem,
quent, frequent, or chronic, with chronic tension-type where they activate second-order neurons. Pathways
headache being defined as headache occurring on 15 from the trigeminal cervical complex transmit signals
or more days per month for at least 3 months. to multiple nuclei in the brainstem, basal ganglia,
hypothalamus, and thalamus, which project into
Migraine multiple cortical areas causing the photophobia,
Migraine is the most common specific headache phonophobia, allodynia, and cognitive dysfunction
diagnosis associated with ED visits.4 Migraine is associated with migraine.7 Calcitonin gene-related
usually accompanied by a variety of associated peptide (CGRP) is a neuropeptide that is a potent
symptoms including nausea, vomiting, and sensitivity vasodilator and enhances synaptic transmission in
to light and sound. There are several types of migraine. It is believed that CGRP acts at multiple
migraine, including migraine without aura, migraine steps along the trigeminovascular pathway, as well
with aura, and chronic migraine. Rarer types of as within the meninges, causing inflammation of the
migraine include: vestibular migraine (characterized meningeal nociceptors.8 CGRP release is inhibited
by vertigo or dizziness); hemiplegic migraine by the activation of serotonin 5-HT1B and 5-HT1D
OCTOBER 2023 • www.ebmedicine.net 4 ©2023 EB MEDICINE
receptors, thus explaining, in part, the mechanism of eye, drooping of the eyelid, and nasal congestion
action of triptan medications.9 or discharge. The attacks can occur multiple times
per day, lasting 15 minutes to 3 hours. Because the
Cluster Headache acute attack does not last more than 3 hours, the
Cluster headache is relatively uncommon, even in pain may have dissipated by the time the emergency
the ED.4 It is characterized by severe, unilateral pain clinician evaluates the patient, so it is imperative for
that occurs in cycles, typically lasting several weeks the clinician to recognize the ongoing cluster cycle.
to months. The pain is often described as a sharp, The pathophysiology of cluster headache is not fully
burning, or piercing sensation, and is usually located understood.10 There is activation of the trigeminal
around the eye, temple, or forehead. Cluster head- nerve, which is responsible for the release of inflamma-
aches are also associated with other symptoms on tory mediators and vasodilation of the blood vessels
the affected side, such as redness and tearing of the supplying the face and scalp. Additionally, dysfunc-
tion of the hypothalamus,
a region of the brain that
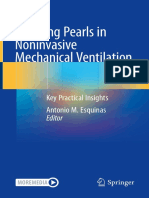
Figure 1. Pathophysiology of Migraine regulates the sleep-wake
Cortex Release of CGRP and PACAP cycle, is thought to explain
Cortical spreading depolarization, altered Multiple potential sources or sites of action the cyclical nature of cluster
connectivity Headache and other symptoms headache attacks.
Migraine aura and cognitive symptoms Target for small-molecule antagonists and
Target for neuromodulation antibodies
Medication Overuse
Headache
Medication overuse head-
ache is a secondary head-
ache disorder that occurs as
a result of excessive use of
analgesics, triptans, or other
medications for headache.11
The amount that qualifies
as “excessive” use varies
from individual to individual,
but at a minimum involves
consistently taking medica-
Thalamus tion for headache for more
Sensitization and alteration of than 2 days every week
thalamo-cortical circuits
for more than 2 months.
Sensory sensitivity and allodynia
Target for neuromodulation Medication overuse head-
ache is a common and often
Trigemino-cervical complex underrecognized condition,
Pain transmission or sensitization affecting up to 5% of the
Hypothalamus
Headache and neck pain
Activation in premonitory phase
Target for medications and
general population. The
Premonitory symptoms
neuromodulation pathophysiology of medi-
Target for hypothalamic peptides cation overuse headache
and modulators
is complex and not fully
understood. Prolonged use
of analgesics, triptans, or
Upper cervical nerves other headache medica-
Pain transmission or sensitization tions can lead to changes
Neck pain and head pain
in pain processing and
Target for local injections and
neuromodulation
neuroplasticity in the central
nervous system, resulting
in a sensitization of pain
Migraine involves the simultaneous alteration in function of multiple components of the central nervous system pathways and perpetuation
and peripheral nervous system, some of which are represented in this diagram. Each of these components of headache symptoms.
could be responsible for different symptoms of migraine, and each could represent a specific therapeutic
The diagnosis of medica-
target in individual patients. Red arrows indicate sensory inputs from the trigeminal nerve and upper cervical
nerve roots, which converge in the trigemino-cervical complex.
tion overuse headache is
Abbreviations: CGRP, calcitonin gene-related peptide; PACAP, pituitary adenylate cyclase-activating polypeptide. typically made based on the
Reprinted from The Lancet Neurology. Volume 17, Issue 2. Andrew Charles. The pathophysiology of migraine: patient’s history of frequent
implications for clinical management. Pages 174-182. Copyright 2018, with permission from Elsevier. or daily use of analgesics or
OCTOBER 2023 • www.ebmedicine.net 5 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
other headache medications, in conjunction with the as these include medication overuse headache,
presence of headache symptoms. idiopathic intracranial hypertension, cryptococcal
meningitis, space-occupying lesions, and giant cell
arteritis. Chronic migraine, in particular, is highly
n Differential Diagnosis prevalent, affecting nearly 2% of the United States
The emergency clinician should be attuned to population, and is common among ED patients who
differences between episodic headaches and make frequent use of the ED.12 Awareness of this
chronic headaches. (See Table 1.) For the purpose diagnosis, as well as medication overuse headache,
of this discussion and consistent with the paradigm (with which chronic migraine is often comorbid),
established in the ICHD-3, episodic headaches are will allow the emergency clinician to have a marked
defined as those that occur on fewer than 15 days per impact on a patient’s life if that patient can be
month and chronic headaches are those that occur on provided with or referred to appropriate care.
15 or more days per month. Most chronic headaches
are headache disorders that have progressed from
episodic to chronic, such as chronic migraine, chronic n Prehospital Care
tension-type headache, and chronic cluster headache. Prehospital clinicians should address the pain, associ-
ated symptoms, and anxiety associated with head-
Episodic Headaches ache while maintaining an awareness of secondary
Episodic headaches include migraine, tension-type causes of headache, including stroke, posttraumatic
headache, and cluster headache, as well as less- intracranial hemorrhage, meningitis, and carbon
common headaches including paroxysmal hemicrania monoxide poisoning. As always, prehospital clinicians
and primary stabbing headache. The emergency should assess the scene for safety and use appropri-
clinician should use the description of the headache ate personal protective equipment when managing
itself, the frequency and timing of previous similar patients with symptoms of an infectious process. If
headaches, and associated features such as nausea, the headache is accompanied by other neurological
photophobia, and functional impairment to make the signs such as weakness, aphasia, or visual loss, and
correct diagnosis. the headache is not part of a recurrent headache
syndrome, the prehospital clinician should consider
Chronic Headaches transport to a stroke center.
Chronic headaches that the emergency clinician All efforts should be made to minimize external
may encounter include chronic migraine, new daily stimuli that may exacerbate the headache. Migraine,
persistent headache, and hemicrania continua. in particular, is associated with sensitivity to a variety
Secondary headaches that may be misdiagnosed of sensory inputs including lights, noises, and odors.
Table 1. Headache Differential Diagnosis
Headache Type Possible Clinical Features
Episodic Headache
Migraine Unilateral, pulsating, functionally disabling; associated with nausea, photophobia, and phonophobia.
Cluster Unilateral, periorbital, severe; relatively short duration (up to 3 hours); associated with other periorbital symptoms
such as lacrimation, conjunctival injection, or ptosis.
Tension-type headache Bilateral pressure or tightness; associated with pericranial muscle tenderness; pain is rarely worse than moderate.
Paroxysmal hemicrania Brief (up to 30 minutes) unilateral headaches that recur multiple times during the day. Similar to cluster headache,
associated with unilateral perioribital symptoms. Usually responsive to indomethacin.
Primary stabbing headache Very brief, recurrent pain that can occur, without associated symptoms, in any part of the head.
Chronic Headache
Chronic migraine Headache of ≥15 days/month for at least 3 months. At least half of these headaches must have migraine features.
New daily persistent headache Persistent and unremitting headache lasting at least 3 months that has a clearly remembered moment of origin.
Hemicrania continua Unilateral headache for at least 3 months with either cluster-like periorbital symptoms or a sense of agitation or
restlessness.
Primary nummular headache Mild or moderate pain felt in a rounded or elliptical area. Pain is chronic and continuous, though it may be
interrupted by spontaneous remissions.
Medication overuse headache Headache occurring at least 15 days/month in a patient with a pre-existing headache disorder in conjunction with
regular overuse of an analgesic or headache medicine for >3 months.
www.ebmedicine.net
OCTOBER 2023 • www.ebmedicine.net 6 ©2023 EB MEDICINE
Patients with migraine may be uncomfortable • Quality: descriptors such as pounding or
because of nausea and vomiting. Patients with cluster pulsating are more typical of migraine, while
headache may feel agitated and restless and may pressure or tightness are more typical for tension-
need to pace. Prehospital clinicians should do their type headache.
best to make the patient comfortable. • Radiates: involvement of the neck may suggest
Prehospital clinicians with access to the medica- the diagnosis of occipital neuralgia or a cervical
tions discussed in the “Treatment” section (beginning radiculopathy.
on page 8) can initiate treatment while en route. In • Severity: an understanding of the severity can
general, opioids should be avoided when treating help the clinician decide treatment strategies.
primary headaches.13 Oxygen delivered at a rate of • Timing: details and patterns can be useful for
15 L/min through a nonrebreather mask effectively understanding the impact of headache on the
treats cluster headache. Exploratory data analysis patient’s life.
indicates that oxygen may be useful for migraine • Under care by anyone: how has the patient been
as well.14 When treating nausea associated with treated?
headache, choose an antidopaminergic medication
that also treats headache, such as metoclopramide Physical Examination
10 mg intravenously/intramuscularly (IV/IM), Physical examination of the patient with headache
prochlorperazine 10 mg IV/IM, or droperidol 2.5 mg should be used to exclude secondary causes of
IV/IM; 4 mg of oral ondansetron or oral disintegrating the headache. Abnormal vital signs may suggest a
tablets may be used to treat nausea, but it is unlikely systemic process, such as an infection or a toxic or
to improve the headache. metabolic disorder. Elevated blood pressure may be
a cause or an effect of the headache. Tachycardia
may be an indication of fever, infection, dehydration,
n Emergency Department Evaluation or stimulant use. Particularly important is a focused
History neurological examination, in which attention is paid
The initial focus of the history should be identifying to an examination of the eyes, including a pupillary
the headache pattern. The clinician should deter- examination, extraocular musculature, and visual
mine the circumstances in which the acute headache fields. A retinal examination may give insight into
began, how often the patient experiences head- evidence of elevated intracranial pressure. Dilating
aches, and whether and how the current headache the pupils with 1 drop of tropicamide 0.5% may
differs from previous headaches. For patients with facilitate a retinal examination if there is concern for
very frequent headaches, inquire about whether the papilledema. A sensory and motor examination of the
headaches progressed from infrequent episodes to face, though low-yield, can give information about
frequent episodes and factors that may have contrib- space-occupying lesions or demyelinating processes.
uted to the progression. Specific patterns should be A functional neurological examination should be
queried. For example, does the headache worsen performed to determine whether the patient can sit,
with position or is it related to dietary habits? Also walk, talk, hear, speak, and move. Localized infection
important is information about previous diagnostic of the scalp and structures of the head and face
workups and treatment strategies that have been ef- should be sought as well, as localized tenderness
fective and those that have not. in the musculature and supporting structures of the
Attention should be paid to headache-associated head and neck. In older patients, check for temporal
features, which may also help identify secondary artery tenderness.
headaches or assign the correct primary headache
diagnosis. It is particularly important to identify
the presence of neurological symptoms, including n Diagnostic Studies
visual changes, sensory disturbances, motor Laboratory Studies
weakness, or speech disturbances. Also important Laboratory studies are rarely helpful for most patients
is information about symptoms of infection and who present to the ED with a primary headache; his-
symptoms that commonly accompany the primary tory and physical examination will dictate the need
headaches, including nausea, vomiting, photophobia, for further workup if they suggest the presence of a
phonophobia, osmophobia, lacrimation, conjunctival secondary headache. For patients with migraine or
injection, and ptosis. cluster headache, a pregnancy test will guide treat-
The OPQRSTU mnemonic may be used to obtain ment decisions. Electrolytes should be checked in
a detailed history. patients with dehydration secondary to associated
• Onset: what are the circumstances in which the vomiting and anorexia. For patients aged ≥50 years,
headache began? erythrocyte sedimentation rate (ESR) and a C-reactive
• Provokes or Palliates: what aggravates or protein testing may be useful to exclude the diag-
alleviates the headache? nosis of giant cell arteritis; however, these laboratory
OCTOBER 2023 • www.ebmedicine.net 7 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
tests are not sufficient to exclude the diagnosis of tients with smaller bleeds presenting >6 hours after
giant cell arteritis in patients with vision loss.15 the event, may not be apparent on a noncontrast
head CT, as sensitivity drops to <95% beyond 6 hours
Clinical Decision Rules and <90% beyond 24 hours.13 For the latter patients,
For patients for whom the history does not suggest a lumbar puncture is required to exclude the diagno-
a primary headache disorder, clinical decision rules sis. While the lumbar puncture detects blood in the
such as the Ottawa subarachnoid hemorrhage rule cerebrospinal fluid, an underlying aneurysm may be
may be used to exclude intracranial hemorrhage screened for by using cerebrovascular imaging such
among patients with abrupt-onset headache. (See as MR angiography or CT angiography.
Table 2.) In a multicenter validation study with Similarly, elevated intracranial pressure is often
2131 participants, the rule was 100% sensitive for not seen on a noncontrast head CT. For diagnosis of
aneurysmal subarachnoid hemorrhage.16 idiopathic intracranial hypertension, a lumbar punc-
ture is required to assess cerebrospinal fluid pressure.
Imaging Studies Values >25 cm H2O are abnormal. Early experimental
For patients with an established diagnosis of migraine data indicate that this diagnosis may also be evaluat-
or other primary headache disorders, neuroimaging ed using point-of-care ultrasound19 or MRI20 to assess
is generally not required for typical exacerbations. optic nerve sheath diameter.
For patients aged <50 years, new-onset headache Finally, a noncontrast head CT will often miss the
requires thoughtful consideration of potential sec- diagnosis of venous sinus thrombosis and cervical
ondary causes of headache, use of the Ottawa artery dissection. Both of these rare diagnoses require
subarachnoid hemorrhage rule (See Table 2), and specific imaging. Venous sinus thrombosis can be
appropriate follow-up to ensure that rare malignant diagnosed with CT or MR venography and cervical
headaches that may be missed in the ED will be diag- artery dissection requires CT or MR angiography or
nosed expeditiously. ultrasound of the vasculature of the neck.
For patients aged ≥50 years, new-onset head-
ache almost always requires neuroimaging, though
this needs to be performed emergently in the ED n Treatment
only for patients with focal neurological findings, al- The immediate goals of ED treatment for headache
tered mental status, or acute onset. For patients who are rapid and complete relief of pain, if possible,
do not receive neuroimaging in the ED, it should be with a minimum of adverse medication effects, and
completed on an outpatient basis within 1 week.17 prompt return of the patient to work or usual activi-
With the exception of the limitations discussed ties. ED treatment should also focus on minimizing
following, a noncontrast computed tomography (CT) postdrome headaches in the days after the ED visit.
scan of the head is the most appropriate test for Finally, emergency clinicians should understand that
ED patients with headache. A noncontrast head CT primary headaches such as migraine or cluster head-
will identify most pathological causes of headache, aches will continue to plague patients in the weeks,
but may be overused among ED patients. National months, and years after the ED visit, and any advice
data from a probabilistic sample of all United States or educational interventions delivered in the ED may
EDs indicate that approximately 95% of ED patients have a lasting impact on the patient’s wellbeing.
with headache who receive a head CT do not have a
pathological cause of headache identified.18 Intravenous Antidopaminergic Antiemetics
It is increasingly accepted in the emergency medi-
Limitations of Head Computed Tomography cine community and established in the medical
Multicenter cohort data indicate that aneurysmal literature that the IV antidopaminergics are highly
subarachnoid hemorrhage, particularly among pa- effective treatment for migraine as monotherapy.21
Antidopaminergics with the best evidence support-
ing use are metoclopramide,22 prochlorperazine,23
Table 2. Ottawa Subarachnoid
and droperidol,24 though the class effect extends to
Hemorrhage Rule for Headache Patients16 haloperidol,25 chlorpromazine, and oral olanzapine.26
For patients aged ≥15 years with new nontraumatic headache that (See Table 3, page 9.) Data to support the use of
peaked in intensity within 1 hour, assess 1 point for each item:
• Age ≥40 years
these medications comes from several dozen meth-
• Neck pain or stiffness odologically rigorous RCTs in which these medica-
• Witnessed loss of consciousness tions were compared to placebo and active compara-
• Onset during exertion tors. In a meta-analysis of 13 studies that included
• Thunderclap onset 3 studies with 185 participants with migraine, IV
• Limited neck flexion on examination
metoclopramide was nearly 3 times more likely than
If any of the criteria are positive (a score of ≥1), subarachnoid placebo to result in significant pain reduction.27 In
hemorrhage cannot be ruled out. a meta-analysis of 11 studies involving 771 partici-
OCTOBER 2023 • www.ebmedicine.net 8 ©2023 EB MEDICINE
pants, prochlorperazine was more than 7 times more pants experienced functionally impairing headaches
effective than placebo with regard to headache during the 48 hours after ED discharge, regardless
relief.23 In a meta-analysis of 5 studies involving 349 of headache diagnosis.37 Dexamethasone can de-
participants who received either prochlorperazine or crease the frequency of these recurrent headaches.
chlorpromazine, the active medications were 9 times In a meta-analysis of 7 studies with 738 individuals,
more likely than placebo to result in clinical success.28 dexamethasone decreased the frequency of head-
Because of these data, the American Headache ache recurrence with a number needed to treat (NNT)
Society recommended both prochlorperazine and of approximately 10.36 In this meta-analysis, medica-
metoclopramide as first-line therapy for migraine.29 tion-related adverse events did not differ substantially
Unfortunately, IV antidopaminergic medica- between dexamethasone and placebo. Therefore,
tions frequently cause side effects, including dizzi- dexamethasone 10 mg IV or IM is an appropriate
ness and extrapyramidal symptoms, most notably treatment for all ED patients with migraine who do
acute akathisia, which occurs in 5% to 10% of pa- not have a contraindication to dexamethasone.
tients administered IV metoclopramide.30,31 Emer-
gency clinicians often co-administer anticholinergic Dihydroergotamine
medications to prevent these symptoms. However, Another antimigraine agent worth mentioning is
primary analysis of a meta-analysis that included 7 dihydroergotamine, an older medication commonly
studies with 1393 participants found that prophy- used for management of status migrainosus. It may
lactic diphenhydramine did not prevent develop- be considered along with the antidopaminergics
ment of extrapyramidal symptoms.32 Infusing the for patients admitted to the hospital with migraine
antidopaminergic agent over 15 minutes rather than refractory to first-line treatment.38 As is true with
as an IV push may decrease the incidence of acute many older medications that were commonly used
extrapyramidal symptoms.33,34 If akathisia develops, it before the modern era of pharmaceutical trials, there
may be treated with IV diphenhydramine 25 mg to 50 is a paucity of high-quality data to define its role.
mg or IV midazolam 2 mg.35 In a meta-analysis of 4 lower-quality studies involv-
ing 254 participants, IV or IM dihydroergotamine
Dexamethasone (dosed 0.5-1 mg) was 3 times more effective than
Data from the National Hospital Ambulatory Medi- parenteral meperidine, an opioid.39 Overall, adverse
cal Care Survey indicate that the most underutilized medication events, most commonly drowsiness and
evidence-based medication in the ED management dizziness, were similar between the groups. There-
of migraine is dexamethasone.1 Although dexmetha- fore, dihydroergotamine may have a role to play in
sone does not appear likely to improve pain out- the ED as a second-line medication to be used prior
comes in the ED, it does decrease the frequency of to opioids or when deciding on admission to the
recurrent headaches,36 a very common and frequently hospital. Dihydroergotamine should not be given to
unrecognized problem after ED discharge.37 In an patients with cardiovascular risk factors or those who
observational study of 309 patients with headache are pregnant.40
who were discharged from the ED, 50% of partici-
Triptans
Triptan medications have never found a major role
in emergency management of migraine, but they
Table 3. Intravenous Antidopaminergic are evidence-based, widely used medications in the
Antiemetics for Acute Headache outpatient setting.9 The American Headache Soci-
Drug Dosage Comments ety has recommended subcutaneous sumatriptan
Metoclopramide 10 mg IV, up to May cause akathisia for use as a first-line medication in the ED, based on
3 doses 15 placebo-controlled studies with more than 2000
Prochlorperazine 10 mg IV May cause akathisia participants.29 However, in multiple comparative ef-
Droperidol 5 mg IV May cause akathisia; ficacy studies, subcutaneous sumatriptan 6 mg was
caution with prolonged not as efficacious as the antidopaminergic medica-
QTc tions metoclopramide and prochlorperazine.39,42-44
Haloperidol 5 mg IV May cause akathisia; Subcutaneous sumatriptan may cause chest pain and
caution with prolonged palpitations, and it should not be used in patients
QTc
with cardiovascular risk factors. Furthermore, patients
Chlorpromazine 25 mg IV May cause akathisia; who initially respond to triptans may have recurrence
may cause orthostatic
of headache in the 24 hours after discharge. Oral
hypotension
triptans are appropriate for use in the ED among
Olanzapine 5 mg PO May cause akathisia
patients who do not require parenteral therapy and
Abbreviations: IV, intravenous; PO, oral. have already failed NSAIDs, or for treatment of post-
www.ebmedicine.net discharge headache. Familiarity with the medications
OCTOBER 2023 • www.ebmedicine.net 9 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
in the triptan class will give the emergency clinician fine the role of novel oral migraine medications for ED
more prescribing options when patients are ready for patients. Though they are FDA-approved for migraine,
discharge. (See Table 4.) their use in the ED should generally be reserved for
patients who do not respond to other medications.
Novel Oral Migraine Medications
5-HT1F Receptor Agonist Opioids
Lasmiditan (REYVOW™) is the first oral serotonin It is now also widely accepted that opioids should not
5-HT1F receptor agonist approved by the United be used as first-line therapy for migraine headache
States Food and Drug Administration (FDA), made patients.29 Database analyses link opioid use to a
available for use in 2020. Recommended dose is a sin- multitude of undesirable outcomes, including increas-
gle dose of 50 mg, 100 mg, or 200 mg, with no more ing the frequency of symptoms of the underlying
than 1 dose in 24 hours.45 It has been demonstrated headache disorder and increasing the frequency of
to be effective versus placebo in the outpatient return visits to the ED.48 Furthermore, opioids are not
setting, but its role in the ED has yet to be defined. as effective as antidopaminergic medication. In a ran-
For now, it can be considered prior to admission for domized study of IV prochlorperazine 10 mg versus
patients refractory to other medications, though clini- IV hydromorphone 1 mg, participants who received
cians should be aware that it caused central nervous prochlorperazine were twice as likely to achieve
system side effects, including dizziness, paresthesias, sustained headache relief.49 Therefore, use of opioids
and fatigue in more than one-third of patients.46 should be reserved for patients who do not respond
to evidence-based first-line therapies.
Anticalcitonin Gene-Related Peptide Medications
Anticalcitonin gene-related peptide (CGRP) medica- Nerve Blocks
tions come in a variety of forms. Various monoclonal As an alternative to systemic therapy for headaches,
antibodies targeting CGRP and its receptor have treating migraine with nerve blocks using local
been approved as migraine preventive medications. anesthetics can be considered. These procedures
CGRP receptor antagonists (gene-related peptide are easy to learn, effective, and generally very well
receptor antagonists, sometimes called “gepants”) tolerated. Minor side effects reported with peripheral
are oral medications approved for acute treatment nerve blocks include a brief burning sensation from
of migraine. In general, they are well tolerated, the local anesthetic, numbness in the distribution of
though they are not as efficacious as currently used the targeted nerve, lightheadedness, and pain from
parenteral treatments. needle injection.50
The novel oral migraine medications are sum- A systematic review and meta-analysis of 9 stud-
marized in Table 5. A systematic review and ies evaluated adults who presented to any clinical
meta-analysis of 64 randomized clinical trials of setting for primary headache disorders.50 It examined
patients experiencing migraine headaches compared the effectiveness of peripheral nerve blocks (greater
the 5-HT1F receptor agonist (lasmiditan), and CGRP occipital nerve block, sphenopalatine ganglion block,
antagonists to triptans and placebo for migraine pain and trigger-point injections) to provide pain relief
relief or freedom from pain.47 The 5-HT1F receptor within 120 minutes versus placebo, sham, or standard
agonist and CGRP antagonists were associated with headache therapy. Compared to placebo, patients
greater odds ratios for pain relief and pain freedom who received nerve blocks had lower pain scores at
compared to placebo, but lower odds ratios com- 1, 5, 15, and 30 minutes. Limited by methodological
pared to triptans. At this time, there are no data to de- heterogeneity (different headache types and differ-
ent techniques for performing the procedures), the
analysis could not assess the effectiveness of nerve
Table 4. Triptan Medications for Acute blocks against standard treatment, but demonstrated
Migraine
Name Dosage Route of Administration
Sumatriptan 6 mg once Subcutaneous injection Table 5. Novel Oral Migraine Medications
Sumatriptan 100 mg once Oral Name Dosage Mechanism of Action
Rizatriptan 10 mg once Oral Lasmiditan 50, 100, and 200 mg, Serotonin 5-HT1F
Almotriptan 12.5 mg once Oral (REYVOW™) once every 24 hr receptor agonist
Eletriptan 40 mg once Oral Ubrogepant 100 mg CGRP receptor
(Ubrelvy®) antagonist
Frovatriptan 2.5 mg once Oral
Rimegepant 75 mg CGRP receptor
Naratriptan 2.5 mg once Oral (Nurtec®) antagonist
Zolmitriptan 2.5 mg Oral
Abbreviation: CGRP, calcitonin gene-related peptide.
www.ebmedicine.net www.ebmedicine.net
OCTOBER 2023 • www.ebmedicine.net 10 ©2023 EB MEDICINE
that, compared to placebo or sham, nerve blocks are bupivacaine 0.5% is infused into the area. Ideally, the
indeed efficacious for migraine and other primary anesthetic will flow over the middle turbinate and
headache disorders. collect in the pterygopalatine fossa, in which lies the
Greater Occipital Nerve Block
Tang et al identified 6 randomized controlled trials Figure 2. Greater Occipital Nerve Block
in a meta-analysis that reviewed the effect of greater
occipital nerve blocks on migraine compared to
placebo or sham injection. Among 180 participants,
greater occipital nerve blocks reduced pain severity,
the number of days the headache persisted, and the
need for other medication.51 Greater
The procedure begins with the patient sitting with occipital
nerve
their neck flexed so that the chin is touching the chest Occipital
or, alternatively, with their forehead resting on a pad- Occipital
protuberance
ded table. Locate the patient’s superior nuchal line artery
and, in the midline, the occipital protuberance, which
is the most prominent bony feature in the midline of Mastoid
the occiput. Then locate the mastoid process. If one process
draws a line between the occipital protuberance and
the mastoid process, the greater occipital nerve is
one-third of the distance, going medially to laterally
along this line. (See Figure 2.) One can confirm the
position by palpating the occipital artery (the greater
occipital nerve is medial to the occipital artery). Draw
up the local anesthetic and prepare to inject with the
smallest needle gauge available (we prefer 27G) and Reprinted from Headache: The Journal of Head and Face Pain. Volume
length (depending on the size of the patient) but suf- 60, Issue 10. E. John Gallagher, Polly E. BIjur, Michael Del Valle, et
ficient to nearly reach to the skull. Insert the needle al. A randomized, double-dummy, emergency department-based
90° toward the occipital bone. Pull back several study of greater occipital nerve block with bupivacaine vs intravenous
metoclopramide for treatment of migraine. Copyright 2020. Used by
millimeters when the bone is encountered. We inject permission of John Wiley and Sons.
1 mL of the local anesthetic at the anatomical spot
identified above, 1 mL medial to the spot, and 1 mL
laterally, with the goal of ensuring sufficient anesthet- Figure 3. Sphenopalatine Ganglion Block
ic enveloping the greater occipital nerve. As with the
sphenopalatine block, many procedural questions re-
main, including which type of anesthetic to use, how
much to administer, and whether bilateral technique
results in better outcomes than unilateral technique.
Sphenopalatine Ganglion Block
Several different techniques have been proposed for
performing this procedure, as published data do not
inform the decision about which technique is optimal.
The technique described here is the one preferred
by the authors because of its ease and reliability.
Patients are placed supine in a slight Trendelenburg
position, positioning the head slightly flexed to a
sniffing position, and then rotated 15° to 20° toward
the side being treated. (See Figure 3.) It is unclear
whether bilateral treatment results in better outcomes
than unilateral treatment. In general, the side with
the worst headache is treated first. A long, 20-gauge
angiocatheter (without the needle) is inserted in
From: Journal of Personalized Medicine. Volume 12, Issue 5. Na Eun
the naris, following the angle of the bridge of the
Kim, Ji Eun Kim, Sook Young Lee, et al. Comparison of temperature and
nose. When resistance is met at the posterior sur- pain changes between the drip and topical methods of administering
face of the nasopharynx, the angiocatheter should the transnasal sphenopalatine ganglion block. © 2022. Published under
be pulled back 1 to 2 mm. Then, 3 mL of topical Creative Commons Attribution 4.0 International License
OCTOBER 2023 • www.ebmedicine.net 11 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
sphenopalatine ganglion. After 5 minutes, the patient pediatric patients.57 In another double-blind study,
should be turned to the other side and the procedure 53 children with migraine were randomized to either
repeated in the opposite naris. The patient is then IV metoclopramide (0.2 mg/kg) + IV ketorolac (0.5
left in the Trendelenburg position for 5 to10 min- mg/kg) or IV metoclopramide + IV placebo.58 There
utes. Many procedural questions are still unanswered were no important differences in efficacy between
and left to the discretion of the emergency clinician the groups in the ED, although headache recurrence
performing the procedure, eg, choice of topical after ED discharge was decreased among those who
anesthetic (we use bupivacaine 0.5%, though others received ketorolac.
have reported success with lidocaine); laterality (it is In a randomized study examining the impact of
not clear whether results are better if the procedure treatment expectation on pain relief, treatment with a
is performed bilaterally rather unilaterally; dose (we 10 mL/kg IV normal saline bolus had minimal impact
use 3 mL, with the goal of ensuring success; however, on pain scores, regardless of whether the children
lower doses may result in less of the unpleasant sen- were prompted to believe that they were treated
sation of oropharyngeal numbness). Clinicians should with IV medication.59 These data indicate that IV
be aware that larger doses are more likely to make fluids should not be used for treatment of migraine
the patient cough or gag, and any dose should be headache among children with migraine who are not
administered slowly. clinically dehydrated.
Older Patients
n Special Populations Migraine can affect individuals of all ages, including
Pediatric Patients older patients, although the prevalence of migraine
Primary headaches are reported by children as young wanes among patients aged ≥60 years.60 The exact
as age 4 years; the median age of children treated reasons for this decrease in migraine frequency are
for migraine in a pediatric ED may be as young as not entirely clear, but may be related to hormonal
12 years.52 Therefore, emergency clinicians need to changes or changes in lifestyle or stress levels. New-
have strategies to treat children in different stages onset migraine can occur among older patients,
of development. Unfortunately, there are very little but this is uncommon and should be a diagnosis of
high-quality data to guide management of children exclusion once pathological causes of headache have
with migraine, and there is a substantial amount of been excluded.
variation in treatment strategies between EDs,53 Older patients with migraine may have other
which reflects the lack of high-quality data. comorbid conditions that can complicate their
Four RCTs conducted among pediatric patients treatment. Furthermore, the management of migraine
are relevant with regard to treatment of children in the elderly can be challenging due to the potential
with migraine. In a double-blind, double-dummy for drug interactions. As a result, treatment plans may
study, 56 children with migraine with a median age need to be adjusted to account for any additional
of 15 years were randomized to treatment with medical conditions or medications.
intranasal ketorolac (1 mg/kg) or IV ketorolac (0.5 Among the medications recommended by the
mg/kg).54 There were no important differences in American Headache Society, metoclopramide and
outcomes in the ED, although some data suggest prochlorperazine remain good choices for older
that 24-hour outcomes were better in the group patients; however, because of their antidopaminergic
that received IV ketorolac. Nevertheless, intranasal activity, they are not appropriate for patients with Par-
ketorolac may be a good treatment option for kinson disease. Because age is an independent risk
patients who would rather not have IV place- factor for cardiovascular disease, sumatriptan is often
ment. Nonrandomized data suggest that intranasal not appropriate for older patients, and triptans should
sumatriptan (20 mg for children weighing ≥40 kg, not be used in patients with cardiovascular disease.
10 mg for children 20-39 kg) may also be a useful The practice of co-administration of an
treatment option for pediatric patients who would anticholinergic medication (such as diphenhydramine)
rather not have IV placement.55 along with an antidopaminergic medication to try to
In a double-blind study, 62 children with a mean decrease extrapyramidal side effects should be con-
age of 14 years were randomized to treatment with sidered carefully for older patients, as anticholinergics
IV ketorolac (0.5 mg/kg) or IV prochlorperazine (0.15 may cause excessive drowsiness and preclude the
mg/kg).56 The children who received prochlorperazine ability to drive home. Dexamethasone 4 mg IV re-
reported substantially more pain relief (NNT for mains an option for older patients with migraine.
treatment success = 3). There were no meaningful Finally, because of the minimal systemic absorp-
adverse medication effects in either study group. tion of local anesthetics, peripheral nerve blocks are
Nonrandomized data also support the use of often an excellent choice for older patients.
prochlorperazine and metoclopramide, both of
which are antidopaminergic medications, for use in
OCTOBER 2023 • www.ebmedicine.net 12 ©2023 EB MEDICINE
Pregnant Patients Nerve Blocks for Cluster Headache
Nearly 25% of females aged in their 20s and 30s suf- Some data suggest that the greater occipital nerve
fer from migraine, so understanding how to address block and the sphenopalatine ganglion block (de-
migraine among persons who are pregnant is essen- scribed on page 11) can also abort acute cluster
tial.60 Pregnancy is known to impact migraine, with headache attacks.61 The data on sphenopalatine
most women experiencing improvement as the preg- ganglion block comes from a population of patients
nancy progresses; however, others may experience with chronic cluster headache who had implanted
worsening or no change in their symptoms. Emer- sphenopalatine neurostimulators. It is unclear whether
gency clinicians may need to alter their antimigraine these data are applicable to ED patients with acute
agents for pregnant patients. The differential diagno- episodic cluster headache who are administered a
sis for headache changes slightly in late pregnancy, as sphenopalatine ganglion block by an emergency
cerebral venous sinus thrombosis becomes relatively clinician. Similarly, open-label studies in patients with
more common, and clinicians need to consider the chronic cluster headache suggest that greater occipi-
diagnosis of pregnancy-induced hypertension. tal nerve blocks may afford some relief, even though
Among the medications for migraine recom- the greater occipital nerve block is performed occipi-
mended by the American Headache Society, tally, and cluster headache is a frontal headache.
metoclopramide is generally considered safe in
pregnancy. Prochlorperazine is also commonly used Other Treatments for Cluster Headaches
in pregnancy and may be used in all trimesters. Be- As with migraine, corticosteroids improve post-ED
cause of the theoretical risk for uterine artery constric- outcomes for patients with cluster headache. The
tion, sumatriptan is often avoided during pregnancy, role of corticosteroids here is not to treat the acute
although accumulated registry data do not indicate attack but instead to stop the ongoing diurnal cluster.
that there is substantial pregnancy risk for women A 2021 multicenter, double-blind, randomized trial
exposed to sumatriptan during the first trimester. of 118 patients by Obermann et al compared oral
Dexamethasone may be used during pregnancy, prednisone versus placebo for short-term preven-
though the timing of dexamethasone administra- tion of episodic cluster headaches within the first
tion should be discussed with the patient’s obstetri- week of treatment.62 Patients were given 100 mg oral
cian if there is any concern for preterm delivery. For prednisone for 5 days, with a taper by 20 mg every
clinicians facile with the various nerve blocks, these 3 days; the control group received placebo tablets.
techniques offer the benefit of antimigraine efficacy The study demonstrated a significant decrease in the
with very little systemic absorption, and so should be number of cluster headache attacks within the first
offered to pregnant women in the ED with migraine. week of treatment, with an average of 2.4 fewer at-
tacks per week in the intervention arm.
Patients With Cluster Headaches In the Obermann trial,62 both groups were
There are several evidence-based treatments avail- concurrently given oral verapamil, which is thought
able for cluster headaches. The first-line treatments to also be effective in preventing cluster headache
for cluster headaches include oxygen and subcu- recurrence in the short-term. Regarding the efficacy
taneous sumatriptan.61 Both of these treatments of verapamil, other data are less compelling: a small
demonstrated efficacy in multicenter RCTs. Based on RCT compared verapamil 120 mg orally 3 times
data from high-quality RCTs, the American Headache per day for 2 weeks to placebo among 30 patients
Society assigned each of these treatments level A with cluster headache. There were no differences in
recommendations.61 With regard to oxygen therapy, outcome during the first week of treatment, but by
the recommended administration is at least 10 L/ min the second week of treatment, those using verapamil
delivered via nonrebreather mask for 15 to 20 min- reported fewer headaches and fewer doses of pain
utes. In one multicenter RCT, oxygen provided com- medication.63 The most bothersome side effect in this
plete relief to about two-thirds of patients within 15 study was constipation.
minutes.61 A benefit of oxygen therapy, as opposed In 2016, the American Headache Society
to the pharmacologic options, is that oxygen is easily published a guideline and systematic review of RCTs
administered without adverse effects. At a dosage of that examined acute and prophylactic treatments
6 mg subcutaneously, sumatriptan provided relief to available for cluster headaches.61 There was no change
75% of patients 15 minutes after administration in a to the previously established level A recommended
multicenter RCT.61 While the triptans can be highly ef- acute treatments: subcutaneous sumatriptan, intranasal
fective in aborting cluster headaches, they should not zolmitriptan, and high-flow oxygen.
be administered to patients with cardiovascular risk As with migraine, opioids are not an appropriate
factors, as they can cause some degree of vasocon- first-line medication for this particular pain presen-
striction. Similarly, subcutaneous sumatriptan should tation. Unfortunately, there are no relevant data to
be avoided in pregnancy. inform best-practice management for patients with
refractory cluster headache. For patients who fail ini-
OCTOBER 2023 • www.ebmedicine.net 13 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
tial therapy, it is reasonable to try a greater occipital migraine prevention.65 These include antibodies
nerve block or, failing that, parenteral opioids. against both the CGRP receptor as well as the CGRP
molecule itself. For patients with high-frequency
Patients With Medication Overuse Headache episodic migraine or chronic migraine, these
Carlsen et al completed a randomized clinical trial of medications typically reduce by half the total number
120 patients with medication overuse headache.64 of migraine days per month, although some patients
The most frequently overused medications were can achieve near-complete elimination of migraine
simple analgesics, combination analgesics, and days.8 If the patient has inadequately treated high-
triptans. They compared 3 treatment strategies: (1) frequency episodic migraine or chronic migraine,
withdrawal from the overused medication + initiation they should be made aware of the existence of these
of headache preventive medication; (2) preventive medications and offered a follow-up appointment
medication alone; and (3) withdrawal alone, with with a neurologist or headache specialist.
optional headache preventive treatment postponed.
The most frequently utilized preventive medications Diagnosis of Headache Disorder
were candesartan, amitriptyline, and metoprolol. Most controversial is whether emergency clinicians
All 3 treatment strategies were equally effective should make the effort to assign a specific headache
in reducing monthly headache days for patients diagnosis to every headache patient who presents to
with medication overuse headache. Although not the ED or whether the diagnosis of “headache not
statistically significantly different, the withdrawal otherwise specified” will suffice. Randomized studies
+ preventive medication group had the greatest have shown that antidopaminergic medication works
numerical reduction in medication use days in well for most patients with headaches who present
addition to decreased headache intensity, making to the ED; besides migraine, metoclopramide has
a combined withdrawal/preventive treatment a demonstrated efficacy for tension-type headache66
reasonable strategy for treating medication overuse and acute posttraumatic headache.67,68 It is likely
headaches. There was no reported association that the antidopaminergics are effective for cluster
between type of preventive strategy and outcomes. headache as well, as nonrandomized data suggest
For more information on initiating preventive that chlorpromazine and olanzapine can confer
treatment in the ED, see the “Disposition” section persistent benefit.69,70 Similarly, corticosteroids are
below. For the emergency clinician, the key actions efficacious for migraine and cluster headaches, as are
are to (1) recognize that medication overuse greater occipital nerve blocks.29,61
headache often coexists with migraine; (2) inform Therefore, an argument can be made that once
the patient that use of medication to treat acute secondary causes of headache have been excluded,
headache more than twice weekly can result in the emergency clinician does not need to provide the
worsening headache; (3) understand that treatment of patient with a specific diagnosis (such as migraine,
medication overuse headache requires discontinuing tension-type headache, cluster headache, or post-
the offending agent; and (4) initiating a preventive traumatic headache), and instead can use the terms
medication is often helpful for improving outcomes in benign headache or headache, not otherwise
these patients. specified, and a specific diagnosis can be provided
subsequently by the primary care physician at
follow-up. While the argument is cogent, safe, and
n Controversies and Cutting Edge sufficient, it embraces a reductivist view of emergency
Development of Novel Drug Treatments medicine. Familiarity with the various headache
Migraine research has progressed dramatically in diagnoses will empower emergency clinicians during
recent years. CGRP was recognized as an important headache encounters and allow them to provide
neurotransmitter in migraine pathophysiology several the patient with specific advice about available
decades ago, when it was noted that markedly treatments. Also, a specific diagnosis may be useful
elevated levels were present in serum samples if first-line treatments do not work. For example,
obtained during an acute attack. The first commercial dihydroergotamine is not appropriate for tension-type
product based on this knowledge was a CGRP headache and corticosteroids are not appropriate for
receptor antagonist that was not approved because posttraumatic headache.
of hepatotoxicity. Two second-generation CGRP
receptor antagonists approved for acute treatment
are modestly effective, with an NNT of about 10.65 n Disposition
(See Table 5, page 10.) These 2 medications each Disposition and ED dwell time will vary from hospital
proved safe and effective in the 2 phase 3 RCTs to hospital, depending on the needs of the commu-
required for FDA approval.65 Subsequent to approval nity, the type of hospital, the availability of specialty
of the initial CGRP receptor antagonist, various services, and the wishes of the patients. Admission to
monoclonal antibodies have been approved for the hospital is appropriate for patients with a debili-
OCTOBER 2023 • www.ebmedicine.net 14 ©2023 EB MEDICINE
tating migraine attack that lasts longer than 72 hours who used sumatriptan.71 For patients with either
and does not respond to first-line oral medications chronic migraine or very frequent episodic migraine,
(status migrainosus) or for patients with headache re- initiation of a migraine preventive medication can
fractory to 2 rounds of IV medication. However, if the make a substantial and lasting positive impact on the
patient does not wish to be admitted and the ED has patient’s wellbeing and can be considered for pa-
the resources to do so, some EDs will keep headache tients who will not be prescribed these medications
patients for as long as 12 hours, while administering elsewhere. Various oral medications used for migraine
multiple rounds of IV medications. For hospitals with prevention are listed in Table 6; however, these
observation units, these may be appropriate for head- medications are prescribed only infrequently by emer-
ache patients who do not respond to initial therapy. gency clinicians.5 These patients should be offered
Recommendations
Patients with chronic migraine and concomitant rapid follow-up with aTo Applycare
primary in Practice
provider who can
medication overuse headache may be particularly dif- continue to work with the patient to identify the ideal
ficult to treat effectively in the ED. It may be appropriate type and dosage of migraine prevention.
to admit these patients for “detoxification” from the 5 Recommendations
overused medication and initiation of a new medica- To Apply in Practice
tion regimen. However, the vast majority of headache
patients will respond to typical ED treatment and will be 5 Things That Will Change
appropriate for discharge with continuing care from out- 5 Recommendations
patient clinicians. It is essential to arrange follow-up for
Your Practice
To Apply in Practice
these patients with a primary care provider or a neurolo-
gist or headache specialist. 1. Use peripheral nerve blocks for migraine
Even patients whose headache is treated suc- and cluster headache. As emergency
cessfully in the ED are likely to experience reucrrence clinicians become more facile with these
during the days and weeks after the ED visit. Patients procedures and they become more
should be provided with appropriate medication to widely used, patient throughput will be
treat these recurrent headaches until they can access expedited, and more patients will be able
outpatient care. While dexamethasone administered to immediately return to work and usual
in the ED can decrease the frequency of postdrome activities.
“aftershock”headaches, post-ED headaches, con- 2. Consider the role of novel anti-CGRP
tinue in up to half of discharged ED patients who medications for ED patients. In the
receive corticosteroids.6 Naproxen 500 mg orally outpatient setting, these medications have
and sumatriptan 100 mg orally are comparably useful proven effective for many patients; however,
to treat these headaches. In a randomized study of their role in the ED is still uncertain. Costing
410 patients treated in the ED for primary headache, around $100 per pill, these medications
51% used naproxen or sumatriptan for treatment of should not replace medications with a
headache recurrence after ED discharge. For patients reliable track record.
using naproxen, 75% achieved effective treatment of 3. A more widespread use of corticosteroids
headache recurrence compared to 68% of patients in the ED will improve post-ED outcomes,
thus benefiting ED patients after discharge,
many of whom continue to suffer from post-
drome “aftershock” headaches long after
Table 6. Oral Medications Used for their ED visit.
Migraine Prevention72 4. Awareness of medication overuse headache
Medication and Dose Class Considerations and management strategies for this diagno-
Propranolol 40 mg PO Beta blocker Fatigue sis will allow a more streamlined experience
daily in 1-4 divided doses for ED patients, many of whom will not need
Metoprolol tartrate 25 mg Beta blocker Fatigue an ED workup once the diagnosis is apparent.
PO BID 5. Decrease opioid use among ED patients.
Valproate 500 mg PO daily Antiepileptic Need to monitor liver Opioid use in the ED, across all indications
in 1-2 divided doses drug enzymes; may cause and specifically for headache, has decreased
pancreatitis
substantially in the last 10 years. This trend is
Topiramate 25 mg PO Antiepileptic May impair memory
likely to continue, improving the experience
daily drug and concentration
for both patients and emergency clinicians,
Amitriptyline 25 mg PO Tricyclic May cause weight
and making the experience less painful for
daily antidepressant gain
those patients with headache refractory to
Note: these medications may require 1 month of treatment and up- everything but opioids.
titration to see efficacy.
Abbreviations: BID, 2 times per day; PO, oral.
OCTOBER 2023 • www.ebmedicine.net 15 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
Risk Management Pitfalls for Managing Primary
Headaches in the Emergency Department
1. “Opioids are a good treatment option 6. “Our pharmacy does not have any triptan
for migraines.” Though historically used for medications.” Oral sumatriptan is now widely
management of migraine in the ED, it has available in a generic version.
become increasingly clear that opioids should
be used only rarely for patients with primary 7. “Performing nerve blocks on pediatric patients
headache disorders. Opioids are associated with is difficult.” Nerve blocks are equally safe and
worsening the underlying headache disorder. If efficacious for children as they are for adults.
poor outcomes occur to patients who receive The greater occipital nerve block may be more
opioids, the emergency clinician may be blamed successful with younger children, as they will
for using an inappropriate medication. In our not need to remain still after administration
practice, we use opioids only for patients with of medication. The main difference is patient
migraine who fail to improve after receiving at cooperation. For older children, the setup and
least 3 parenteral treatments and also a greater procedure may be similar to that for performing
occipital nerve block. the nerve block on adults. For younger children,
using similar immobilization techniques (ie,
2. “The actual diagnosis doesn’t matter.” While parent holding the child or papoosing the child
it is not imperative for emergency clinicians to in a sheet or blanket) may be beneficial while
attribute headache characteristics to a specific performing ganglion blocks.
diagnosis, it can aid in acute treatment of the
patient’s symptoms, as well as for recommending 9. “There is no role for greater occipital nerve
outpatient treatment and patient education. blocks or sphenopalatine ganglion nerve
blocks in patients with cluster headaches.”
3. “For pregnant patients with headache, you There are reports of relief or improvement of
can only give acetaminophen.” Though many pain in patients with cluster headaches after
medications are contraindicated in pregnancy, nerve blocks. If there is no termination of cluster
acetaminophen, metoclopramide, and peripheral headaches with oxygen and triptan use, it may be
nerve blocks are all viable treatment options. In worthwhile to perform a nerve block, as the side
addition, dexamethasone can be given, when effects are relatively benign.
done in conjunction with recommendations from
the patient’s obstetrician. 10. “Standard headache medications don’t have
any serious side effects.” Emergency clinicians
4. “Medication overuse headache is a fake term.” must be aware of medication side effects that
Medication overuse headache is defined as may impact their headache patients. Triptans
headache occurring ≥15 days/month in people and dihydroergotamine are contraindicated
with a known headache disorder who have been in patients with cardiovascular disease and
using 1 or more headache relief medications >2 should be used carefully in patients at risk
days per week for >3 months. The long-term for cardiovascular disease. Antidopaminergic
treatment is detoxification of the offending medications may cause a range of extrapyramidal
medications. side effects.
5. “The patient states that they took triptans for
their migraine, but it didn’t improve the pain.”
Oral triptans are most efficacious within the first
few hours of the migraine attack.
OCTOBER 2023 • www.ebmedicine.net 16 ©2023 EB MEDICINE
Case Conclusions
For the 36-year-old woman with a history of migraine who presented with 12 hours of headache and
nausea…
You determined that this patient had no risk factors for intracranial pathology, so a diagnostic workup was
not appropriate, even though she did not respond to first-line management. The 1 atypical feature in her
CASE 1
presentation was that she did not respond to metoclopramide + ketorolac, a regimen that is effective at
relieving headache and associated symptoms in the vast majority of patients with migraine. You ordered
another dose of 10 mg IV metoclopramide, combined with 1 mg IV dihydroergotamine, and you added 10
mg IV dexamethasone to prevent recurrence of headache the next day. When she improved, you advised
her to continue to use 100 mg oral sumatriptan, 600 mg oral ibuprofen, or the combination of the 2 for any
migraine recurrence. You cautioned her not to use sumatriptan within 24 hours of taking dihydroergotamine,
and you discharged her with primary care follow-up.
For the 45-year old man with a history of infrequent migraine who presented to the ED with 1 week
of unremitting headache…
Because this patient reported that he had been experiencing headache nearly every day for the past month
and had been using a triptan and ibuprofen on a daily basis, you determined that he had medication
CASE 2
overuse headache. You ordered 10 mg IV metoclopramide + 10 mg IV dexamethasone. You explained that
the overuse of his medication was causing the headache, and advised him to avoid NSAIDs and triptans.
You prescribed the combination of 10 mg oral metoclopramide + 1000 mg oral acetaminophen as his
new abortive regimen and advised him not to take these medications more than 2 or 3 times per week. In
addition, you prescribed 20 mg oral propranolol to be taken twice daily every day to prevent headaches.
You discharged him with rapid neurology follow-up.
For the 53-year-old woman with a history of frequent headaches for more than 10 years, now
presenting with severe headache and requesting an opioid…
This patient met criteria for chronic migraine because she was experiencing headaches more days than not.
CASE 3
You performed bilateral greater occipital nerve blocks, using a total of 6 mL of 0.5% bupivacaine to block
both her right and left greater occipital nerves. You also performed bilateral sphenopalatine ganglion blocks
by administering 3 mL of 0.5% bupivacaine into each naris. You obtained consult with a neurologist, who
saw the patient in the ED, restarted daily oral topiramate 25 mg for headache prevention, oral eletriptan
40 mg to be used not more than twice weekly, and agreed to see the patient in his office the next day for
continuing care.
n Summary n Time- And Cost-Effective Strategies
• There are a large number of evidence-based • Patients with migraine and other primary
treatments available for migraine. Opioids headaches often do not require diagnostic
should be used only as a last resort. Familiarity testing. Effective management of patients
with novel oral migraine therapeutics will give with headache can be performed efficiently
the emergency clinician additional tools in the by minimizing diagnostic workups and using
armamentarium against migraine. parenteral therapy only when required.
• Dexamethasone should be considered for • Some patients do not require an injection. The
patients with migraine who present to the ED. emergency clinician should be familiar with
• Nerve blocks are easy to perform and can provide evidence-based migraine medications that
relief for patients with migraine while causing few do not require an IV, including subcutaneous
side effects and not impairing the patient’s ability sumatriptan, oral triptans, and newer oral
to work, drive, and return to usual activities. medications including serotonin 5-HT1F agonists
• For patients with cluster headache, consider (lasmiditan) and CGRP-receptor antagonists.
treatment with oxygen and sumatriptan, and • Contrary to common management, IV fluids do
consider starting the patient on corticosteroids to not seem to help patients with migraine feel
break the cluster. better. In a nonrandomized study of 570 ED
• For patients with medication overuse headache, patients treated with IV metoclopramide, those
recognizing the diagnosis and initiating detoxifica- who received IV fluid reported less pain relief on
tion treatment can help break the cycle of pain. a 0 to 10 scale.73
OCTOBER 2023 • www.ebmedicine.net 17 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
Clinical Pathway for Managing Primary Headaches in
the Emergency Department
Patient presents with headache, and malignant secondary
causes of headache have been ruled out
Is this patient suffering from a cluster headache?
YES NO
Treat for cluster headache with
Does the patient need parenteral treatment?
high-flow oxygen and sumatriptan (Class I)
NO YES
Administer oral NSAID, oral triptan (sumatriptan 100 mg PO
or eletriptan 80 mg PO) or both (Class I)
• Administer metoclopramide 10 mg IV and dexamethasone
10 mg mg IV (Class I)
• Alternatively, consider greater occipital nerve block or
Reassess. Is the headache sufficiently improved? NO sphenopalatine ganglion block (Class II)
• For tension-type headache, do not use corticosteroids
Reassess. Is the headache sufficiently improved? • Administer additional metoclopramide 10 mg IV and
NO
ketorolac 15 mg IV (Class II)
• Administer additional metoclopramide 10 mg IV and
Reassess. Is the headache sufficiently improved? NO
dihydroergotamine 1 mg IV (Class III)
• For tension-type headache, do not use dihydroergotamine
Consider treatment with 1 of the following:
Reassess. Is the headache sufficiently improved? NO • Anti-CGRP medication (Class II)
• Lasmiditan (Class II)
• Opioid (Class III)
YES
Reassess. Is the headache sufficiently improved? NO Admit patient for further management
YES
Is this patient suffering from medication overuse headache? NO Arrange appropriate outpatient follow-up
YES
Patient will require inpatient or outpatient detoxification
Abbreviations: CGRP, calcitonin gene-related peptide; IV, intravenous; NSAID, nonsteroidal anti-inflammatory drug; PO, orally.
For Class of Evidence Definitions, see page 19.
OCTOBER 2023 • www.ebmedicine.net 18 ©2023 EB MEDICINE
n References 9.* Loder E. Triptan therapy in migraine. N Engl J Med.
2010;363(1):63-70. (Review) DOI: 10.1056/NEJMct0910887
Evidence-based medicine requires a critical appraisal 10. Hoffmann J, May A. Diagnosis, pathophysiology, and
of the literature based upon study methodology and management of cluster headache. Lancet Neurol.
number of subjects. Not all references are equally 2018;17(1):75-83. (Review)
robust. The findings of a large, prospective, random 11. Ashina S, Terwindt GM, Steiner TJ, et al. Medication overuse
ized, and blinded trial should carry more weight than headache. Nat Rev Dis Primers. 2023;9(1):5. (Review)
a case report. 12. Friedman BW, Serrano D, Reed M, et al. Use of the emergency
To help the reader judge the strength of each department for severe headache. A population-based study.
Headache. 2009;49(1):21-30. (Population-based survey)
reference, pertinent information about the study will
13. American College of Emergency Physicians Clinical Policies
be included in bold type following the reference, Subcommittee on Acute Headache, Godwin SA, Cherkas
where available. In addition, the most informative DS, et al. Clinical Policy: critical issues in the evaluation and
references cited in this paper, as determined by the management of adult patients presenting to the emergency
author, are noted by an asterisk (*) next to the number department with acute headache. Ann Emerg Med.
of the reference. 2019;74(4):e41-e74. (Review)
14. Singhal AB, Maas MB, Goldstein JN, et al. High-flow oxy-
1. Friedman BW, West J, Vinson DR, et al. Current management gen therapy for treatment of acute migraine: a randomized
of migraine in US emergency departments: an analysis of crossover trial. Cephalalgia. 2017;37(8):730-736. (Randomized
the National Hospital Ambulatory Medical Care Survey. controlled study; 22 patients)
Cephalalgia. 2015;35(4):301-309. (Database analysis) 15. Kermani TA, Schmidt J, Crowson CS, et al. Utility of erythrocyte
2. Headache Classification Committee of the International sedimentation rate and C-reactive protein for the diagnosis of
Headache Society (IHS) the International Classification of giant cell arteritis. Semin Arthritis Rheum. 2012;41(6):866-871.
Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. (Retrospective analysis; 754 patients)
(Guideline) 16. Perry JJ, Stiell IG, Sivilotti ML, et al. Clinical decision rules to
3. Ashina S, Bendtsen L, Ashina M. Pathophysiology of tension- rule out subarachnoid hemorrhage for acute headache. JAMA.
type headache. Curr Pain Headache Rep. 2005;9(6):415-422. 2013;310(12):1248-1255. (Prospective cohort study; 2132
(Review) patients)
4. Friedman BW, Hochberg ML, Esses D, et al. Applying the 17.* Edlow JA, Panagos PD, Godwin SA, et al. Clinical Policy: critical
International Classification of Headache Disorders to the issues in the evaluation and management of adult patients
emergency department: an assessment of reproducibility and presenting to the emergency department with acute headache.
the frequency with which a unique diagnosis can be assigned Ann Emerg Med. 2008;52(4):407-436. (Research support, non-
to every acute headache presentation. Ann Emerg Med. United States government)
2007;49(4):409-419. (Prospective; 300 patients) DOI: 10.1016/j.jen.2008.12.009
5. Charbit AR, Akerman S, Goadsby PJ. Dopamine: what’s new in 18. Gilbert JW, Johnson KM, Larkin GL, et al. Atraumatic headache
migraine? Curr Opin Neurol. 2010;23(3):275-281. (Review) in US emergency departments: recent trends in CT/MRI utilisa-
tion and factors associated with severe intracranial pathology.
6. Latev A, Friedman BW, Irizarry E, et al. A randomized trial of
Emerg Med J. 2012;29(7):576-581. (National cross-sectional
a long-acting depot corticosteroid versus dexamethasone
study; 30,000 patients)
to prevent headache recurrence among patients with acute
migraine who are discharged from an emergency department. 19. Graziano M, Biondino D, Fioretto I, et al. Optic nerve sheath
Ann Emerg Med. 2019;73(2):141-149. (Randomized controlled diameter measurement by ultrasound after moderate traumatic
trial; 220 patients) brain injury. Clin Exp Emerg Med. 2023;10(2):249-250. (Review)
7. Goadsby PJ, Holland PR. An update: pathophysiology of mi- 20. Aspide R, Bertolini G, Belotti LMB, et al. Magnetic resonance-
graine. Neurol Clin. 2019;37(4):651-671. (Review) based assessment of optic nerve sheath diameter: a
prospective observational cohort study on inter- and intra-rater
8. Santos-Lasaosa S, Belvis R, Cuadrado ML, et al. Calcitonin
agreement. J Clin Med. 2023;12(7):2713. (Prospective cohort
gene-related peptide in migraine: from pathophysiology to
study; 50 patients)
treatment. Neurologia (Engl Ed). 2022;37(5):390-402. (Review)
Class of Evidence Definitions
Each action in the clinical pathways section of Emergency Medicine Practice receives a score based on the following definitions.
Class I Class II
• Always acceptable, safe • Safe, acceptable Class III Indeterminate
• Definitely useful • Probably useful • May be acceptable • Continuing area of research
• Proven in both efficacy and effectiveness • Possibly useful • No recommendations until further
Level of Evidence: • Considered optional or alternative research
Level of Evidence: • Generally higher levels of evidence treatments
• One or more large prospective studies • Nonrandomized or retrospective stud- Level of Evidence:
are present (with rare exceptions) ies: historic, cohort, or case control Level of Evidence: • Evidence not available
• High-quality meta-analyses studies • Generally lower or intermediate levels • Higher studies in progress
• Study results consistently positive and • Less robust randomized controlled trials of evidence • Results inconsistent, contradictory
compelling • Results consistently positive • Case series, animal studies, • Results not compelling
consensus panels
• Occasionally positive results
This clinical pathway is intended to supplement, rather than substitute for, professional judgment and may be changed depending upon a patient’s individual
needs. Failure to comply with this pathway does not represent a breach of the standard of care.
Copyright © 2023 EB Medicine. www.ebmedicine.net. No part of this publication may be reproduced in any format without written consent of EB Medicine.
OCTOBER 2023 • www.ebmedicine.net 19 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
21.* Friedman BW. Managing migraine. Ann Emerg Med. dexamethasone for acute severe migraine headache:
2017;69(2):202-207. (Review) meta-analysis of randomised controlled trials for preventing
DOI: 10.1016/j.annemergmed.2016.06.023 recurrence. BMJ. 2008;336(7657):1359-1361. (Meta-analysis; 7
22. Friedman BW, Mulvey L, Esses D, et al. Metoclopramide for studies, 738 patients)
acute migraine: a dose-finding randomized clinical trial. Ann 37. Friedman BW, Hochberg ML, Esses D, et al. Recurrence of
Emerg Med. 2011;57(5):475-482. (Randomized controlled primary headache disorders after emergency department
trial; 356 patients) discharge: frequency and predictors of poor pain and functional
23. Golikhatir I, Cheraghmakani H, Bozorgi F, et al. The efficacy outcomes. Ann Emerg Med. 2008;52(6):696-704. (Observa-
and safety of prochlorperazine in patients with acute mi- tional study; 309 patients)
graine: a systematic review and meta-analysis. Headache. 38. Raskin NH. Repetitive intravenous dihydroergotamine as
2019;59(5):682-700. (Meta-analysis; 11 studies, 771 patients) therapy for intractable migraine. Neurology. 1986;36(7):995-
24. Miner JR, Fish SJ, Smith SW, et al. Droperidol vs. 997. (Clinical trial; 55 patients)
prochlorperazine for benign headaches in the emergency de- 39. Friedman BW, Kapoor A, Friedman MS, et al. The relative
partment. Acad Emerg Med. 2001;8(9):873-879. (Clinical trial; efficacy of meperidine for the treatment of acute migraine: a
168 patients) meta-analysis of randomized controlled trials. Ann Emerg Med.
25. Gaffigan ME, Bruner DI, Wason C, et al. A randomized 2008;52(6):705-713. (Meta-analysis; 4 studies)
controlled trial of intravenous haloperidol vs. intravenous 40. Carleton SC, Shesser RF, Pietrzak MP, et al. Double-blind,
metoclopramide for acute migraine therapy in the emergency multicenter trial to compare the efficacy of intramuscular
department. J Emerg Med. 2015;49(3):326-334. (Randomized dihydroergotamine plus hydroxyzine versus intramuscular
controlled trial; 64 patients) meperidine plus hydroxyzine for the emergency department
26. Hill CH, Miner JR, Martel ML. Olanzapine versus droperidol for treatment of acute migraine headache. Ann Emerg Med.
the treatment of primary headache in the emergency depart- 1998;32(2):129-138. (Randomized controlled trial; 172
ment. Acad Emerg Med. 2008;15(9):806-811. (Randomized patients)
controlled trial; 100 patients) 41. Kelly AM, Ardagh M, Curry C, et al. Intravenous chlorpromazine
27. Colman I, Brown MD, Innes GD, et al. Parenteral versus intramuscular sumatriptan for acute migraine. J Accid
metoclopramide for acute migraine: meta-analysis of ran- Emerg Med. 1997;14(4):209-211. Randomized controlled trial;
domised controlled trials. BMJ. 2004;329(7479):1369-1373. 43 patients)
(Meta-analysis; 13 studies; 185 patients) 42. Friedman BW, Corbo J, Lipton RB, et al. A trial of
28. Kelly AM, Walcynski T, Gunn B. The relative efficacy of metoclopramide vs sumatriptan for the emergency depart-
phenothiazines for the treatment of acute migraine: a meta- ment treatment of migraines. Neurology. 2005;64(3):463-468.
analysis. Headache. 2009;49(9):1324-1332. (Meta-analysis; 13 (Randomized controlled trial; 80 patients)
studies) 43. Talabi S, Masoumi B, Azizkhani R, et al. Metoclopramide versus
29.* Orr SL, Friedman BW, Christie S, et al. Management of adults sumatriptan for treatment of migraine headache: a randomized
with acute migraine in the emergency department: the Ameri- clinical trial. J Res Med Sci. 2013;18(8):695-698. (Randomized
can Headache Society evidence assessment of parenteral controlled trial; 124 patients)
pharmacotherapies. Headache. 2016;56(6):911-940. (Review) 44. Kostic MA, Gutierrez FJ, Rieg TS, et al. A prospective, random-
DOI: 10.1111/head.12835 ized trial of intravenous prochlorperazine versus subcutane-
30. Friedman BW, Bender B, Davitt M, et al. A randomized trial ous sumatriptan in acute migraine therapy in the emergency
of diphenhydramine as prophylaxis against metoclopramide- department. Ann Emerg Med. 2010;56(1):1-6. (Randomized
induced akathisia in nauseated emergency department controlled trial; 68 patients)
patients. Ann Emerg Med. 2009;53(3):379-385. (Randomized 45. United States Food and Drug Administration. Lasmiditan
controlled trial; 286 patients) package insert: Reference ID: 4505262. 2019. (Drug package
31. Friedman BW, Mulvey L, Esses D, et al. Metoclopramide for insert)
acute migraine: a dose-finding randomized clinical trial. Ann 46. Maiti R, Mishra A, Puliappadamb HM, et al. Efficacy and
Emerg Med. 2011;57(5):475-482 (Randomized controlled trial; safety of lasmiditan for acute treatment of migraine in adults:
356 patients) a meta-analysis. J Clin Pharmacol. 2021;61(12):1534-1544.
32. Mokhtari A, Yip O, Alain J, et al. Prophylactic administration (Meta-analysis; 4 studies)
of diphenhydramine to reduce neuroleptic side effects in the 47. Yang CP, Liang CS, Chang CM, et al. Comparison of new
acute care setting: a systematic review and meta-analysis. J pharmacologic agents with triptans for treatment of migraine:
Emerg Med. 2021;60(2):165-174. (Meta-analysis; 9 studies, a systematic review and meta-analysis. JAMA Netw Open.
1648 total paatients) 2021;4(10):e2128544. (Meta-analysis; 64 trials)
33. Tura P, Erdur B, Aydin B, et al. Slow infusion metoclopramide 48. Friedman BW, Vinson DR. Convincing the skeptic. How to fix
does not affect the improvement rate of nausea while re- emergency department headache management. Cephalalgia.
ducing akathisia and sedation incidence. Emerg Med J. 2014;35(8):641-643. (Editorial)
2012;29(2):108-112. (Randomized controlled trial; 140 pa- 49. Friedman BW, Irizarry E, Solorzano C, et al. Randomized study of
tients) IV prochlorperazine plus diphenhydramine vs IV hydromorphone
34. Egerton-Warburton D, Povey K. Administration of for migraine. Neurology. 2017;89(20):2075-2082. (Randomized
metoclopramide by infusion or bolus does not affect the controlled trial; 126 patients)
incidence of drug-induced akathisia. Emerg Med Australas. 50.* Patel D, Yadav K, Taljaard M, et al. Effectiveness of peripheral
2013;25(3):207-212. (Randomized controlled trial; 205 nerve blocks for the treatment of primary headache disor-
patients) ders: a systematic review and meta-analysis. Ann Emerg Med.
35. Erdur B, Tura P, Aydin B, et al. A trial of midazolam vs 2022;79(3):251-261. (Meta-analysis; 9 studies)
diphenhydramine in prophylaxis of metoclopramide-induced DOI: 10.1016/j.annemergmed.2021.08.007
akathisia. Am J Emerg Med. 2012;30(1):84-91. (Randomized 51. Tang Y, Kang J, Zhang Y, et al. Influence of greater occipital
controlled trial; 160 patients) nerve block on pain severity in migraine patients: a systematic
36. Colman I, Friedman BW, Brown MD, et al. Parenteral review and meta-analysis. Am J Emerg Med. 2017;35(11):1750-
OCTOBER 2023 • www.ebmedicine.net 20 ©2023 EB MEDICINE
1754. (Meta-analysis; 6 studies) 68. Friedman BW, Adewunmi V, Campbell C, et al. A randomized
52. Perry MC, Yaeger SK, Toto RL, et al. A modern epidemic: trial of intravenous ketorolac versus intravenous metoclopramide
increasing pediatric emergency department visits and admis- plus diphenhydramine for tension-type and all nonmigraine, non-
sions for headache. Pediatr Neurol. 2018;89:19-25. (Database cluster recurrent headaches. Ann Emerg Med. 2013;62(4):311-
analysis) 318. (Randomized controlled trial; 120 patients)
53. Richer LP, Laycock K, Millar K, et al. Treatment of children with 69. Caviness VS Jr, O’Brien P. Cluster headache: response to
migraine in emergency departments: national practice variation chlorpromazine. Headache. 1980;20(3):128-131. (Case series; 3
study. Pediatrics. 2010;126(1):e150-e155. (Retrospective analy- patients)
sis; 1694 visits) 70. Rozen TD. Olanzapine as an abortive agent for cluster head-
54. Tsze DS, Lubell TR, Carter RC, et al. Intranasal ketorolac versus ache. Headache. 2001;41(8):813-816. (Case series; 5 patients)
intravenous ketorolac for treatment of migraine headaches 71. Friedman BW, Solorzano C, Esses D, et al. Treating headache
in children: a randomized clinical trial. Acad Emerg Med. recurrence after emergency department discharge: a randomized
2022;29(4):465-475. (Randomized controlled trial; 60 controlled trial of naproxen versus sumatriptan. Ann Emerg Med.
patients) 2010;56(1):7-17. (Randomized controlled trial; 410 patients)
55. Hauser Chatterjee J, Hartford EA, Law E, et al. Sumatriptan as 72. Silberstein SD, Holland S, Freitag F, et al. Evidence-based
a first-line treatment for headache in the pediatric emergency guideline update: pharmacologic treatment for episodic
department. Pediatr Neurol. 2023;142:68-75. (Retrospective migraine prevention in adults: report of the Quality Standards
analysis; 558 patients) Subcommittee of the American Academy of Neurology and
56. Brousseau DC, Duffy SJ, Anderson AC, et al. Treatment of the American Headache Society. Neurology. 2012;78(17):1337-
pediatric migraine headaches: a randomized, double-blind 1345. (Guideline)
trial of prochlorperazine versus ketorolac. Ann Emerg Med. 73. Balbin JE, Nerenberg R, Baratloo A, et al. Intravenous fluids for
2004;43(2):256-262. (Randomized controlled trial; 62 pa- migraine: a post hoc analysis of clinical trial data. Am J Emerg
tients) Med. 2015. (Database analysis)
57. Werner K, Qaiser S, Kabbouche M, et al. Intravenous migraine
treatment in children and adolescents. Curr Pain Headache
Rep. 2020;24(8):45. (Review)
58. Richer LP, Ali S, Johnson DW, et al. A randomized trial of
ketorolac and metoclopramide for migraine in the emergency
department. Headache. 2022;62(6):681-689. (Randomized
controlled trial; 53 patients)
59. Richer L, Craig W, Rowe B. Randomized controlled trial of treat-
ment expectation and intravenous fluid in pediatric migraine.
Headache. 2014;54(9):1496-1505. (Randomized controlled
trial; 45 patients)
60. Victor TW, Hu X, Campbell JC, et al. Migraine prevalence by
age and sex in the United States: a life-span study. Cephalalgia.
2010;30(9):1065-1072. (National cross-sectional study)
61.* Robbins MS, Starling AJ, Pringsheim TM, et al. Treatment of
cluster headache: the American Headache Society evidence-
based guidelines. Headache. 2016;56(7):1093-1106. (Review)
DOI: 10.1111/head.12866
62.* Obermann M, Nagel S, Ose C, et al. Safety and efficacy of
prednisone versus placebo in short-term prevention of episodic
cluster headache: a multicentre, double-blind, randomised
controlled trial. Lancet Neurol. 2021;20(1):29-37. (Randomized
controlled trial; 118 patients)
DOI: 10.1016/S1474-4422(20)30363-X Stay up-to-date on the
63. Leone M, D’Amico D, Frediani F, et al. Verapamil in the prophy- most relevant topics in
laxis of episodic cluster headache: a double-blind study versus
placebo. Neurology. 2000;54(6):1382-1385. (Randomized emergency medicine with EMplify
controlled trial; 30 patients)
at www.ebmedicine.net/podcast
64. Carlsen LN, Rouw C, Westergaard ML, et al. Treatment of medi-
cation overuse headache: effect and predictors after 1 year--a
randomized controlled trial. Headache. 2021;61(7):1112-1122.
(Randomized controlled trial; 100 patients)
65. Silvestro M, Orologio I, Siciliano M, et al. Emerging drugs for
the preventive treatment of migraine: a review of CGRP mono-
clonal antibodies and gepants trials. Expert Opin Emerg Drugs.
2023;28(2):79-96. (Review)
66. Weinman D, Nicastro O, Akala O, et al. Parenteral treatment of
episodic tension-type headache: a systematic review. Head-
ache. 2014;54(2):260-268. (Review)
67. Friedman BW, Irizarry E, Cain D, et al. Randomized study of
metoclopramide plus diphenhydramine for acute posttraumatic
headache. Neurology. 2021;96(18):e2323-e2331. (Randomized
controlled trial; 160 patients)
OCTOBER 2023 • www.ebmedicine.net 21 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
n CME Questions 5. What outcomes are associated with the use of
Current subscribers receive CME credit opioids for migraine?
absolutely free by completing the a. More ED visits; transformation of episodic
following test. Each issue includes 4 AMA migraine to chronic migraine
PRA Category 1 CreditsTM, 4 ACEP b. Respiratory depression, hypoxia, and
Category I credits, 4 AAFP Prescribed bradycardia
credits, and 4 AOA Category 2-B credits. c. Shorter ED stays; increased patient
Online testing is available for current and archived satisfaction
issues. To receive your free CME credits for this d. Rapid relief of pain
issue, scan the QR code below with your
smartphone or visit www.ebmedicine.net/1023 6. What are the landmarks for the greater
occipital nerve block?
a. Use ultrasound to identify occipital artery;
greater occipital nerve can be found medial
to this
b. Occipital protuberance and mastoid process;
the greater occipital nerve can be found
one-third of the distance medial to lateral
1. What are the characteristics of tension-type between these structures
headache? c. Apply topical anesthetic to the medial surface
a. Muscular pain of the middle nasal turbinate
b. Lacrimation or conjunctival injection d. Supraorbital ridge
c. Photophobia and phonophobia
d. Bilateral headache without nausea or vomiting 7. What is the technique for administering the
sphenopalatine block?
2. What is chronic migraine? a. Inject bupivacaine supraorbitally
a. At least 1 episodic migraine attack monthly b. Atomize 4% lidocaine in a full face mask
for at least 5 years c. Inject bupivacaine 0.5% to the inferior
b. Migraine attacks of sufficient severity and occipital area
frequency to require preventive medication d. Place the patient supine with head tilted
c. Migraine characterized by headache on more laterally so that the topical anesthetic will
days than not for at least 3 months pool near the sphenopalatine fossa
d. A headache spiral that begins with increasing
use of medication for acute headache 8. What are the current Level A recommended
treatments for cluster headaches?
3. Which medications are recommended by a. Dihydroergotamine
the American Headache Society emergency b. Corticosteroids
department migraine guidelines to treat the c. Metoclopramide + verapamil
acute headache? d. Subcutaneous sumatriptan + oxygen
a. Ketorolac, rimegepant, rizatriptan
b. Prochlorperazine, sumatriptan, and 9. What medication should be prescribed
metoclopramide for cluster headache to prevent headache
c. Dexamethasone recurrence the next day?
d. Dihydroergotamine, haloperidol, ketamine a. Corticosteroids
b. Subcutaneous sumatriptan + oxygen
4. Why should one consider corticosteroids for c. Diltiazem
migraine? d. Dihydroergotamine
a. They decrease the frequency of
extrapyramidal side effects 10. What is an effective treatment strategy for
b. They enhance the short-term efficacy of medication overuse headache?
primary abortive medications a. Administer oxygen >10 L/ min +
c. They decrease the frequency and severity of corticosteroids
post-discharge headaches b. Treat the acute headache with typical
d. They treat medication overuse headache migraine treatment; discontinue the overused
medication; initiate a preventive
c. Perform greater occipital nerve block
d. Administer nonsteroidal anti-inflammatory
drugs
OCTOBER 2023 • www.ebmedicine.net 22 ©2023 EB MEDICINE
The Emergency Medicine Practice Editorial Board
EDITOR-IN-CHIEF Daniel J. Egan, MD Charles V. Pollack Jr., MA, MD, CRITICAL CARE EDITORS
Andy Jagoda, MD, FACEP Harvard Affiliated Emergency FACEP, FAAEM, FAHA, FACC, William A. Knight IV, MD,
Professor and Chair Emeritus, Medicine Residency, FESC FACEP, FNCS
Department of Emergency Massachusetts General Hospital/ Clinician-Scientist, Department Associate Professor of
Medicine; Director, Center for Brigham and Women's Hospital, of Emergency Medicine, Emergency Medicine and
Emergency Medicine Education Boston, MA University of Mississippi School Neurosurgery, Medical Director,
and Research, Icahn School of of Medicine, Jackson MS EM Advanced Practice Provider
Marie-Carmelle Elie, MD
Medicine at Mount Sinai, New Professor and Chair, Department Ali S. Raja, MD, MBA, MPH Program; Associate Medical
York, NY of Emergency Medicine Executive Vice Chair, Emergency Director, Neuroscience ICU,
ASSOCIATE EDITOR-IN-CHIEF University of Alabama at Medicine, Massachusetts General University of Cincinnati,
Birmingham, Birmingham, AL Hospital; Professor of Emergency Cincinnati, OH
Kaushal Shah, MD, FACEP Medicine and Radiology, Harvard
Assistant Dean of Academic Nicholas Genes, MD, PhD Scott D. Weingart, MD, FCCM
Medical School, Boston, MA Editor-in-Chief, emCrit.org
Advising, Vice Chair of Clinical Assistant Professor,
Education, Professor of Ronald O. Perelman Department Robert L. Rogers, MD, FACEP, PHARMACOLOGY EDITOR
Clinical Emergency Medicine, of Emergency Medicine, NYU FAAEM, FACP
Grossman School of Medicine, Assistant Professor of Emergency Aimee Mishler, PharmD, BCPS
Department of Emergency
New York, NY Medicine, The University of Emergency Medicine Pharmacist,
Medicine, Weill Cornell School of
Maryland School of Medicine, St. Luke's Health System,
Medicine, New York, NY Michael A. Gibbs, MD, FACEP
Baltimore, MD Boise, ID
EDITORIAL BOARD Professor and Chair, Department
RESEARCH EDITOR
of Emergency Medicine, Alfred Sacchetti, MD, FACEP
Saadia Akhtar, MD, FACEP Carolinas Medical Center, Assistant Clinical Professor, Joseph D. Toscano, MD
Associate Professor, Department University of North Carolina Department of Emergency Chief, Department of Emergency
of Emergency Medicine, School of Medicine, Medicine, Thomas Jefferson Medicine, San Ramon Regional
Associate Dean for Graduate Chapel Hill, NC University, Philadelphia, PA Medical Center, San Ramon, CA
Medical Education, Program
Director, Emergency Medicine Steven A. Godwin, MD, FACEP Robert Schiller, MD INTERNATIONAL EDITORS
Residency, Mount Sinai Beth Professor and Chair, Department Chair, Department of Family
Peter Cameron, MD
Israel, New York, NY of Emergency Medicine, Medicine, Beth Israel Medical
Academic Director, The Alfred
Assistant Dean, Simulation Center; Senior Faculty, Family
William J. Brady, MD, FACEP, Emergency and Trauma Centre,
Education, University of Medicine and Community
FAAEM Monash University, Melbourne,
Florida COM-Jacksonville, Health, Icahn School of Medicine
Professor of Emergency Medicine Australia
Jacksonville, FL at Mount Sinai, New York, NY
and Medicine; Medical Director, Andrea Duca, MD
Emergency Management, Joseph Habboushe, MD MBA Scott Silvers, MD, FACEP
Attending Emergency Physician,
UVA Medical Center; Medical Assistant Professor of Clinical Associate Professor of
Ospedale Papa Giovanni XXIII,
Director, Albemarle County Fire Emergency Medicine, Emergency Medicine, Chair of
Bergamo, Italy
Rescue, Charlottesville, VA Department of Emergency Facilities and Planning, Mayo
Medicine, Weill Cornell School Clinic, Jacksonville, FL Suzanne Y.G. Peeters, MD
Calvin A. Brown III, MD of Medicine, New York, NY; Co- Attending Emergency Physician,
Chair of Emergency Medicine, Corey M. Slovis, MD, FACP,
founder and CEO, MDCalc Flevo Teaching Hospital, Almere,
Lahey Hospital and Medical FACEP
The Netherlands
Center, Burlington, MA Eric Legome, MD Professor and Chair Emeritus,
Chair, Emergency Medicine, Department of Emergency Edgardo Menendez, MD,
Peter DeBlieux, MD Mount Sinai West & Mount Sinai Medicine, Vanderbilt University FIFEM
Professor of Clinical Medicine, St. Luke's; Vice Chair, Academic Medical Center, Nashville, TN Professor in Medicine and
Louisiana State University School Affairs for Emergency Medicine, Emergency Medicine; Director of
of Medicine; Chief Experience Stephen H. Thomas, MD, MPH
Mount Sinai Health System, Icahn EM, Churruca Hospital of Buenos
Officer, University Medical Department of Emergency
School of Medicine at Mount Aires University, Buenos Aires,
Center, New Orleans, LA Medicine, Beth Israel Deaconess
Sinai, New York, NY Argentina
Medical Center and Harvard
Deborah Diercks, MD, MS, Keith A. Marill, MD, MS Medical School, Boston, MA Dhanadol Rojanasarntikul, MD
FACEP, FACC Associate Professor, Department Attending Physician, Emergency
Professor and Chair, Department Ron M. Walls, MD
of Emergency Medicine, Harvard Medicine, King Chulalongkorn
of Emergency Medicine, Professor and COO, Department
Medical School, Massachusetts Memorial Hospital; Faculty
University of Texas Southwestern of Emergency Medicine, Brigham
General Hospital, Boston, MA of Medicine, Chulalongkorn
Medical Center, Dallas, TX and Women's Hospital, Harvard
University, Thailand
Angela M. Mills, MD, FACEP Medical School, Boston, MA
Professor and Chair, Department Edin Zelihic, MD
of Emergency Medicine, Head, Department of Emergency
Columbia University Vagelos Medicine, Leopoldina Hospital,
College of Physicians & Schweinfurt, Germany
Surgeons, New York, NY
OCTOBER 2023 • www.ebmedicine.net 23 © 2023 EB MEDICINE. ALL RIGHTS RESERVED.
Points & Pearls
QUICK READ
Evidence-Based Emergency
Department Management
of Migraine and Other
OCTOBER 2023 | VOLUME 25 | ISSUE 10 Primary Headaches
Points
• ED evaluation of headache can be summarized
Pearls
by the OPQRSTU mnemonic. Query the patient • IV antidopaminergics are highly effective treat-
regarding: onset, provokes/palliates, quality, ment for migraine as monotherapy.21-26 See
radiates, severity, timing, and under treatment. Table 3 for drugs and dosages.
• The physical examination focuses on excluding • Opioids should be reserved for patients
secondary causes of the headache. The neuro- who do not respond to evidence-based
logic examination is most important, and particu- therapies, as they are not as effective as
lar attention should be paid to the eyes. antidopaminergic medications.13,29,49
• Results of the history and physical examination • Nerve blocks, including greater occipital nerve
will dictate the need for further workup. block (see Figure 2) and sphenopalatine gan-
• Headaches may be episodic (<15 days/month) or glion nerve block (see Figure 3) are easy to
chronic (≥15 days/month for 3 months). learn, effective, and generally well tolerated.
• Chronic migraine affects nearly 2% of the popula- • Subcutaneous sumatriptan is not as effica-
tion and is commonly seen in the ED.12 cious as metoclopramide and prochlorpera-
• Chronic headache may be caused by or exacer- zine,39,42-44 and patients who respond initially
bated by medication overuse headache (MOH), a may have a recurrence in 24 hours.
secondary headache disorder. • Oral triptans are appropriate in the ED for
• MOH is caused by consistent overuse of medica- patients not requiring parenteral therapy, have
tions (simple and combination analgesics and post discharge headache, or failed NSAIDs.
triptans) for >2 days every week for >2 months. • Postdrome “aftershock” headaches occur in
• Treatment of MOH includes cessation of use plus 50% of patients after ED discharge.37 Ad-
initiation of preventive treatment.64 Admission ministration of dexamethasone can decrease
for detoxification may be needed; however, most frequency.36
can be discharged for outpatient treatment.
• Because of the lack of systemic effects, nerve
blocks can be a good choice for patients who are
pregnant, elderly, or have contraindications. • For new-onset headache in patients aged ≥50
• Intranasal (IN) ketorolac and IN sumatriptan may years, neuroimaging is usually required.
be useful treatment options for pediatric patients • There are limitations with head CT, including: lower
when IV placement is not desired.54,55 sensitivity with smaller bleeds after ≥6 hours;13 el-
• Side effects of antidopaminergics can be treated evated intracranial pressure is often not seen; and
with diphenhydramine or midazolam.33-35 diagnosis of venous sinus thrombosis and cervical
• Cluster headache is characterized by severe, artery dissection may be missed.
unilateral pain, usually around the eye, temple, • Dihydroergotamine can be a second-line medica-
or forehead, occurring in cycles of 15 minutes tion to use prior to opioids or prior to admission.
to 3 hours for weeks or months. Because pain • Subcutaneous sumatriptans and dihydroergo-
may subside by ED evaluation, it is important to tamine should be avoided in pregnant patients or
recognize the cluster cycle. those with cardiovascular disease.
• Treatment for cluster headache is oxygen and • The novel treatments, anticalcitonin gene-related
subcutaneous sumatriptan.61,62 Nerve blocks may peptide (CGRP) drug and lasmiditan (serotonin
be effective.61 5-HT1F receptor agonist), have shown promising
• For new-onset headache in patients aged <50 results, but are expensive and have not had exten-
years, imaging is usually not required. Use the sive use in the ED.
Ottawa subarachnoid hemorrhage (SAH) rule.16
(See Table 2.) Online calculators are available.
OCTOBER 2023 • www.ebmedicine.net 24 ©2023 EB MEDICINE
You might also like
- Gastroenterology Clinical Focus, 3eDocument350 pagesGastroenterology Clinical Focus, 3edoctorali1995No ratings yet
- Case-Based Pace, ICDs, and CRT Volume 1Document234 pagesCase-Based Pace, ICDs, and CRT Volume 1oxequlalisNo ratings yet
- Miller's Anesthesia, 8th Edition: Anesthesiology April 2016Document3 pagesMiller's Anesthesia, 8th Edition: Anesthesiology April 2016Sabbir AhammedNo ratings yet
- OSCE For The Final FFICMDocument318 pagesOSCE For The Final FFICMMohd Saif KhanNo ratings yet
- Anesthesiology Core Review 1st EditionDocument588 pagesAnesthesiology Core Review 1st EditionVeronica ChavezNo ratings yet
- Management of Status Epilepticus, Refractory Status Epilepticus, and Super-Refractory Status EpilepticusDocument44 pagesManagement of Status Epilepticus, Refractory Status Epilepticus, and Super-Refractory Status EpilepticusAndrej TNo ratings yet
- TIVA Part I - Pharmacokinetic Principles and Methods of Delivery PDFDocument56 pagesTIVA Part I - Pharmacokinetic Principles and Methods of Delivery PDFMaria José RecheNo ratings yet
- CV - David Gozal M.D. (USA)Document87 pagesCV - David Gozal M.D. (USA)MSKCNo ratings yet
- ACS NSQIP Geriatric 2016 Guidelines PDFDocument65 pagesACS NSQIP Geriatric 2016 Guidelines PDFWayan Sutresna YasaNo ratings yet
- Hypertensive EmergenciesDocument28 pagesHypertensive EmergenciesluonganhsiNo ratings yet
- Management of Allergic Reactions and Anaphylaxis in The EmergencyDocument23 pagesManagement of Allergic Reactions and Anaphylaxis in The EmergencyAna Belén Viteri luzuriagaNo ratings yet
- Toxic Ingestions Pediatric EmergencyDocument24 pagesToxic Ingestions Pediatric EmergencyXimenaEspinaNo ratings yet
- AngioedemaDocument24 pagesAngioedemaMed. TrackNo ratings yet
- Pulmonary EmbolismDocument28 pagesPulmonary EmbolismMaNiaaa LoxONo ratings yet
- Community Acquired Pneumonia 2Document22 pagesCommunity Acquired Pneumonia 2carosegurallNo ratings yet
- Surgical AirwaysDocument24 pagesSurgical AirwaysMed. TrackNo ratings yet
- Procedural Sedation AnalgesiaDocument24 pagesProcedural Sedation Analgesiabenitez1228No ratings yet
- Advances in Cardiac Resuscitation in The Emergency Department 1Document24 pagesAdvances in Cardiac Resuscitation in The Emergency Department 1Jhon Bayron Muñoz QuinteroNo ratings yet
- 0221 Community-Acquired-PneumoniaDocument29 pages0221 Community-Acquired-PneumoniaDiego YanezNo ratings yet
- 0221 Ocular ConditionsDocument28 pages0221 Ocular ConditionsDiego YanezNo ratings yet
- Diabetic EmergenciesDocument24 pagesDiabetic EmergencieshabibfmNo ratings yet
- 0115 Seizures and SEDocument28 pages0115 Seizures and SEGavin TexeirraNo ratings yet
- 0822 Cardiac Valve EmergenciesDocument23 pages0822 Cardiac Valve EmergenciessarahmacielNo ratings yet
- Stoelting Anasthesia and Co Existing Disease PDFDocument28 pagesStoelting Anasthesia and Co Existing Disease PDFEgidia SetyaNo ratings yet
- Diagnosis and Management of Headache A ReviewDocument12 pagesDiagnosis and Management of Headache A ReviewAlicia GarcíaNo ratings yet
- Elsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFDocument230 pagesElsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFMila KarmilaNo ratings yet
- Management of Deep Vein Thrombosis in The Emergency DepartmentDocument24 pagesManagement of Deep Vein Thrombosis in The Emergency Departmentmundode paisajes100% (1)
- Anesthesia: A Comprehensive Review (5th Edition)Document1 pageAnesthesia: A Comprehensive Review (5th Edition)brakim23No ratings yet
- Avinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006Document29 pagesAvinash B Kumar MD Assistant Professor Anesthesiology and Critical Care Dec 2006sgod34No ratings yet
- MONA BASH C Morphine (Venodilates, Helps Nitrates) + O2 + Nitrates + ASA + BB (Carvedilol) + ACE Inhibitor + Statins..Document6 pagesMONA BASH C Morphine (Venodilates, Helps Nitrates) + O2 + Nitrates + ASA + BB (Carvedilol) + ACE Inhibitor + Statins..Daniel RNo ratings yet
- Complication of Spina AnesthesiaDocument8 pagesComplication of Spina AnesthesiaSandroLaoNo ratings yet
- Emergency Medicine Practice MTBI Article With CMEDocument35 pagesEmergency Medicine Practice MTBI Article With CMEAnonymous 2ur6PyFNo ratings yet
- Infective EndocarditisDocument24 pagesInfective EndocarditisNicolás HonoresNo ratings yet
- Vol 20.2 - Cerebrovascular Disease.2014 PDFDocument229 pagesVol 20.2 - Cerebrovascular Disease.2014 PDFpuskesmas tarikNo ratings yet
- Antonio M. Esquinas - Teaching Pearls in Noninvasive Mechanical Ventilation - Key Practical Insights-Springer (2022)Document537 pagesAntonio M. Esquinas - Teaching Pearls in Noninvasive Mechanical Ventilation - Key Practical Insights-Springer (2022)Jose CastellonNo ratings yet
- Practical Emergency Resuscitation and Critical Care, 2nd Edition (Original PDF From Publisher)Document655 pagesPractical Emergency Resuscitation and Critical Care, 2nd Edition (Original PDF From Publisher)Duk Han KimNo ratings yet
- Acute Myocardial Ischaemia ESICMDocument76 pagesAcute Myocardial Ischaemia ESICMpaskariatne probo dewiNo ratings yet
- CCSAP 2017book3 Sample ChapterDocument20 pagesCCSAP 2017book3 Sample ChapterMohanBabuNo ratings yet
- Gunshot Wounds - Ballistic Trauma in The Emergency DepartmentDocument30 pagesGunshot Wounds - Ballistic Trauma in The Emergency DepartmentMulugeta DagneNo ratings yet
- Antrim ED Handbook 2019Document238 pagesAntrim ED Handbook 2019Chris Jardine LiNo ratings yet
- Sedatives in Neurocritical Care 2019 Curr Opin Crit CareDocument8 pagesSedatives in Neurocritical Care 2019 Curr Opin Crit CareCAMILO ERNESTO DAZA PERDOMONo ratings yet
- Regional Anesthesia and Acute Pain Medicine A Problem Based LearningDocument617 pagesRegional Anesthesia and Acute Pain Medicine A Problem Based LearningDAMIAN MERCADO BENTNo ratings yet
- Preoperative Assessment and Premedication - PACUDocument60 pagesPreoperative Assessment and Premedication - PACUTraceNo ratings yet
- 0712 StrokeDocument28 pages0712 Strokejkim2097No ratings yet
- Sepsis, Severe Sepsis, and Septic Shock: Current Evidence For Emergency Department ManagementDocument24 pagesSepsis, Severe Sepsis, and Septic Shock: Current Evidence For Emergency Department ManagementAdrianita0716No ratings yet
- Clasificacion de Tumores Cerebreales de La OMS 2016 Articulo de RevisionDocument17 pagesClasificacion de Tumores Cerebreales de La OMS 2016 Articulo de RevisionSebastian SalvadorNo ratings yet
- Weakness A Systematic Approach To Acute Non-Traumatic NDocument28 pagesWeakness A Systematic Approach To Acute Non-Traumatic Ncalmira3653No ratings yet
- Jama 2021 326 1840Document11 pagesJama 2021 326 1840silviaNo ratings yet
- Approach To The Adult Patient With Syncope in The Emergency DepartmentDocument26 pagesApproach To The Adult Patient With Syncope in The Emergency DepartmentVinicius DumontNo ratings yet
- The Difficult Airway (2639)Document207 pagesThe Difficult Airway (2639)Eduardo López de Castilla S.No ratings yet
- Epilepsy SleepDocument19 pagesEpilepsy SleepValois MartínezNo ratings yet
- Traumatic Brain InjuryDocument219 pagesTraumatic Brain InjuryDra Carolina Escalante Neurologa de AdultosNo ratings yet
- Vol 21.2 Neuro-Oncology.2015Document315 pagesVol 21.2 Neuro-Oncology.2015sammy_emerichNo ratings yet
- Keppra SAHDocument9 pagesKeppra SAHMonette Juinio CepedaNo ratings yet
- 0413 Massive Upper GI BleedingDocument12 pages0413 Massive Upper GI BleedingIsaura MendezNo ratings yet
- Emergency Room: Case Scenario (Group 1)Document40 pagesEmergency Room: Case Scenario (Group 1)Victoria Castillo TamayoNo ratings yet
- Emergency Manual Stanford Version 2022Document60 pagesEmergency Manual Stanford Version 2022cristian gutierrezNo ratings yet
- HFNC Noninvasive VentilationDocument24 pagesHFNC Noninvasive VentilationAbody MenaNo ratings yet
- Identifying Emergency Department Patients With Chest Pain Who Are at Low Risk For Acute Coronary SyndromesDocument24 pagesIdentifying Emergency Department Patients With Chest Pain Who Are at Low Risk For Acute Coronary SyndromesCarlos Alejandro Rojas CastellanosNo ratings yet
- Nonaccidental Trauma Pediatric Emergency MedicineDocument20 pagesNonaccidental Trauma Pediatric Emergency MedicineMohamed OsmanNo ratings yet
- Pediatric Orthopedic Injuries Urgent CareDocument33 pagesPediatric Orthopedic Injuries Urgent CareMohamed OsmanNo ratings yet
- Ocular Injuries Trauma EXTRADocument38 pagesOcular Injuries Trauma EXTRAMohamed OsmanNo ratings yet
- DR Ez ElarabDocument12 pagesDR Ez ElarabMohamed OsmanNo ratings yet
- KapilloDocument62 pagesKapilloMohamed OsmanNo ratings yet