You might also like
- Secrets To Wild Sex Special Report PDFDocument37 pagesSecrets To Wild Sex Special Report PDFLeon Dhanraj50% (10)
- Profile of A Treatment Plan:: Early Stage Middle Stage Late StageDocument37 pagesProfile of A Treatment Plan:: Early Stage Middle Stage Late StageLea Laura100% (1)
- Arthritis - BoronDocument18 pagesArthritis - BoronNatalia NeliNo ratings yet
- 12 Week Shred - Dieting - Low Carbohydrate Diet PDFDocument37 pages12 Week Shred - Dieting - Low Carbohydrate Diet PDFonslaughtilusNo ratings yet
- Feline Anemia Diagnostic AlgorithmDocument1 pageFeline Anemia Diagnostic AlgorithmEd BlackadderNo ratings yet
- Ventilation Rule of ThumbDocument22 pagesVentilation Rule of ThumbZawzaw LinNo ratings yet
- Gupy - Simulado1Document2 pagesGupy - Simulado1Agnes Moreti50% (6)
- Clinical Vs Actuarial Judgment Original ArticleDocument7 pagesClinical Vs Actuarial Judgment Original ArticlepaengerzieNo ratings yet
- A Universal Model of Diagnostic Reasoning.14Document7 pagesA Universal Model of Diagnostic Reasoning.14Emília SantocheNo ratings yet
- Methuselah-An Expert System For Diagnosis in Geriatric PsychiatryDocument12 pagesMethuselah-An Expert System For Diagnosis in Geriatric PsychiatryMilton MurilloNo ratings yet
- The Use of Clinical Trials in Comparative Effectiv PDFDocument9 pagesThe Use of Clinical Trials in Comparative Effectiv PDFSilverio CasillasNo ratings yet
- Clinical Reasoning 2Document10 pagesClinical Reasoning 2Phooi Yee LauNo ratings yet
- Clinical Reasoning in Manual TherapyDocument11 pagesClinical Reasoning in Manual TherapyKhushboo PakhraniNo ratings yet
- Week 1: Nature of BiostatisticsDocument6 pagesWeek 1: Nature of BiostatisticsNo OneNo ratings yet
- Clinical Versus Actuarial Judgment: Methods of Judgment and Means of ComparisonDocument19 pagesClinical Versus Actuarial Judgment: Methods of Judgment and Means of ComparisonanguschandlerNo ratings yet
- 11.1 Diagnostic Tests 1-S2.0-S0001299818300941-MainDocument7 pages11.1 Diagnostic Tests 1-S2.0-S0001299818300941-MainHelioPassulequeNo ratings yet
- FBC and MortalityDocument6 pagesFBC and MortalityFabiolaNo ratings yet
- RCT TipsDocument5 pagesRCT Tipsa1765874No ratings yet
- B Metris 2 - Summary Study DesignsDocument28 pagesB Metris 2 - Summary Study DesignsSawada TsunayoshiNo ratings yet
- He Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceDocument7 pagesHe Clinical Integrative Puzzle For Teaching and Assessing Clinical Reasoning Preliminary Feasibility, Reliability, and Validity EvidenceFrederico PóvoaNo ratings yet
- Theaching Clinicla Medicine The Key Principals. Q J Med. 2015Document8 pagesTheaching Clinicla Medicine The Key Principals. Q J Med. 2015Carolina Serna RojasNo ratings yet
- Learning The Art and Science of Diagnosis - JAMADocument2 pagesLearning The Art and Science of Diagnosis - JAMAJose Antonio Tous OlagortaNo ratings yet
- Clinicalresearchfocus: The Research QuestionDocument4 pagesClinicalresearchfocus: The Research QuestionNiputu CintyadewiNo ratings yet
- Neurosurgeons' Armamentarium For The Management of Refractory Postherpetic Neuralgia: A Systematic Literature ReviewDocument11 pagesNeurosurgeons' Armamentarium For The Management of Refractory Postherpetic Neuralgia: A Systematic Literature ReviewJaime XavierNo ratings yet
- Stat & ResearchDocument276 pagesStat & ResearchSYED ALI HUSSAINNo ratings yet
- Quasi-Experimentos Infect DeseaseDocument8 pagesQuasi-Experimentos Infect DeseaseAlan MoraesNo ratings yet
- Clinical Reasoning - Jones PDFDocument12 pagesClinical Reasoning - Jones PDFIsabelGuijarroMartinezNo ratings yet
- Group-3-Clustering PatientsDocument25 pagesGroup-3-Clustering Patientsቤኪ የአዲስ ልጅNo ratings yet
- Computer Assisted Diagnosis of Malformation Syndromes - An Evaluation of Three DatabasesDocument11 pagesComputer Assisted Diagnosis of Malformation Syndromes - An Evaluation of Three Databasesron potterNo ratings yet
- The Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Document14 pagesThe Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Cristian Steven Cabezas JoyaNo ratings yet
- 2 Rationament Clinic 2021Document48 pages2 Rationament Clinic 2021Catalina MusteațaNo ratings yet
- Transdisciplinary Approaches Enhance The Production of Translational KnowledgeDocument12 pagesTransdisciplinary Approaches Enhance The Production of Translational KnowledgereneNo ratings yet
- Kanfer 1965Document10 pagesKanfer 1965Erika Lorena Soto PadillaNo ratings yet
- The Meta-Analysis in Evidence-Based Medicine: High-Quality Research When Properly PerformedDocument3 pagesThe Meta-Analysis in Evidence-Based Medicine: High-Quality Research When Properly PerformedAdin SuryaNo ratings yet
- Effective Psychological Interventions For RelapseDocument2 pagesEffective Psychological Interventions For RelapseRicardo EscNo ratings yet
- 01 - Youngstrom2015 Clinical Guide To The Evidence-Based Assessment Approach To Diagnosis and Treatment.Document16 pages01 - Youngstrom2015 Clinical Guide To The Evidence-Based Assessment Approach To Diagnosis and Treatment.Ionela BărbosNo ratings yet
- Considerations For Planning and Designing Meta-Analysis in Oral MedicineDocument9 pagesConsiderations For Planning and Designing Meta-Analysis in Oral Medicinedrvivek reddyNo ratings yet
- Ethics in Research: Historical OverviewDocument9 pagesEthics in Research: Historical OverviewJmarie Brillantes PopiocoNo ratings yet
- Analisis RCT Continuous Outcome - Google SearchDocument13 pagesAnalisis RCT Continuous Outcome - Google SearchRaudhatulAisyFachrudinNo ratings yet
- (10920684 - Neurosurgical Focus) Informed Consent in Neurosurgery - A Systematic ReviewDocument10 pages(10920684 - Neurosurgical Focus) Informed Consent in Neurosurgery - A Systematic ReviewOnilis RiveraNo ratings yet
- 1 - Outcomes ResearchDocument12 pages1 - Outcomes ResearchMauricio Ruiz MoralesNo ratings yet
- How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyDocument17 pagesHow Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyAlexNo ratings yet
- Lindsay Nat Rev DD 2003Document8 pagesLindsay Nat Rev DD 2003douniahamouda87No ratings yet
- TMP A447Document14 pagesTMP A447FrontiersNo ratings yet
- Lessons in Uncertainty and Humility - Clinical Trials Involving HypertensionDocument11 pagesLessons in Uncertainty and Humility - Clinical Trials Involving HypertensionGustian Satria PratamaNo ratings yet
- Best Practice & Research Clinical RheumatologyDocument13 pagesBest Practice & Research Clinical RheumatologydrharivadanNo ratings yet
- Nihms 741059Document16 pagesNihms 741059Panagiotis MisthosNo ratings yet
- Clinical Observation of Treatment Efficacy in Sepsis: A Prospective StudyDocument7 pagesClinical Observation of Treatment Efficacy in Sepsis: A Prospective StudyIJAR JOURNALNo ratings yet
- Schwartz, Dell - 2010 - Case Series Investigations in Cognitive NeuropsychologyDocument22 pagesSchwartz, Dell - 2010 - Case Series Investigations in Cognitive NeuropsychologyCamilla OelfeldNo ratings yet
- Evidence-Based Medicine: David L. SackettDocument3 pagesEvidence-Based Medicine: David L. SackettNicolas MarinNo ratings yet
- R Brain Activity and Medical Diagnosis ADocument15 pagesR Brain Activity and Medical Diagnosis AkhadirNo ratings yet
- An Equation For Excellence in Clinical Reasoning: Editorial Taro Shimizu and Mark L. GraberDocument3 pagesAn Equation For Excellence in Clinical Reasoning: Editorial Taro Shimizu and Mark L. GraberFrederico PóvoaNo ratings yet
- Martino, D. (2023) - Treatment Failure in Persisten Tic Disorders...Document15 pagesMartino, D. (2023) - Treatment Failure in Persisten Tic Disorders...cuautzinNo ratings yet
- Clinical and Research Applications of A Brain Tumor Tissue Bank in The Age of Precision MedicineDocument12 pagesClinical and Research Applications of A Brain Tumor Tissue Bank in The Age of Precision MedicineSandra Milena Sanabria BarreraNo ratings yet
- Study Designs: Shraddha Parab, Supriya BhaleraoDocument5 pagesStudy Designs: Shraddha Parab, Supriya BhaleraoPavithra balasubramaniNo ratings yet
- Bliss 2015Document5 pagesBliss 2015Dii ScottouNo ratings yet
- Fuzzy Logic in MedicineDocument4 pagesFuzzy Logic in MedicinepierreNo ratings yet
- Perspective: New England Journal MedicineDocument4 pagesPerspective: New England Journal MedicineYRHLI7389No ratings yet
- MEDECIELO MELO - Chapter 5 SummaryDocument12 pagesMEDECIELO MELO - Chapter 5 SummaryMelo MedecieloNo ratings yet
- Context and Clinical ReasoningDocument8 pagesContext and Clinical ReasoningFrederico PóvoaNo ratings yet
- Pharmaceutical Sciences: Cognitive Schemes For Clinical Diagnostic Reasoning by Medical StudentsDocument8 pagesPharmaceutical Sciences: Cognitive Schemes For Clinical Diagnostic Reasoning by Medical StudentsiajpsNo ratings yet
- Systematic Reviews and Meta-And Pooled AnalysesDocument11 pagesSystematic Reviews and Meta-And Pooled AnalysesVictor abramonteNo ratings yet
- Part 17 PDFDocument6 pagesPart 17 PDFKarolina PolskaNo ratings yet
- Dimensional PsychopathologyFrom EverandDimensional PsychopathologyMassimo BiondiNo ratings yet
- Practical Gynecologic Pathology: Frequently Asked QuestionsFrom EverandPractical Gynecologic Pathology: Frequently Asked QuestionsJian-Jun WeiNo ratings yet
- Practical Oncologic Molecular Pathology: Frequently Asked QuestionsFrom EverandPractical Oncologic Molecular Pathology: Frequently Asked QuestionsNo ratings yet
- Perceived Stress Scale Tip SheetDocument3 pagesPerceived Stress Scale Tip SheetAilynne Joy Rojas LimNo ratings yet
- Hospitalization Reimbursement Claim Form - Part ADocument1 pageHospitalization Reimbursement Claim Form - Part AFahad MehmoodNo ratings yet
- Rebecca Jud - Literature Review 4Document7 pagesRebecca Jud - Literature Review 4api-548795337No ratings yet
- Good Health Is Your BirthrightDocument16 pagesGood Health Is Your BirthrightRamosNo ratings yet
- 1 The Hospital Team: LanguageDocument3 pages1 The Hospital Team: Languagewidya tirtaNo ratings yet
- Healthy Habits PPT Grade 11Document20 pagesHealthy Habits PPT Grade 11Alex ValdecañasNo ratings yet
- Gs RecommendationDocument2 pagesGs RecommendationEvangeline Layug-MartinezNo ratings yet
- A Good Doctor: "In Nothing Do Men More Nearly Approach The Gods Than in Giving Health To Men". (Cicero)Document26 pagesA Good Doctor: "In Nothing Do Men More Nearly Approach The Gods Than in Giving Health To Men". (Cicero)Ioana Alexandra TrifNo ratings yet
- Impact of Covid 19 On E-Marketing in Pharmaceutical IndustryDocument4 pagesImpact of Covid 19 On E-Marketing in Pharmaceutical Industryamit singhNo ratings yet
- Lipids: TEST(s) Normal UNIT(s)Document1 pageLipids: TEST(s) Normal UNIT(s)usman noorNo ratings yet
- LifespanDevelopment 05 EarlyChildhoodDocument38 pagesLifespanDevelopment 05 EarlyChildhoodjapstudyaccNo ratings yet
- '-Daftar Harga Reagen LabtestDocument1 page'-Daftar Harga Reagen LabtestUPT Labkes R/LNo ratings yet
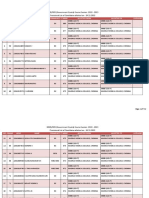
- MBBS/BDS (Government Quota) Course Session:2022 - 2023 Provisional List of Candidates Allotted On - 24.11.2022Document732 pagesMBBS/BDS (Government Quota) Course Session:2022 - 2023 Provisional List of Candidates Allotted On - 24.11.2022AKSHRAA K VNo ratings yet
- Justin Daniel NG Suy Physical Fitness 1 GE11 Activity 1: Exercise Is MedicineDocument2 pagesJustin Daniel NG Suy Physical Fitness 1 GE11 Activity 1: Exercise Is MedicineJustin Daniel L. Ng SuyNo ratings yet
- Mental Health Atlas India-WhoDocument1 pageMental Health Atlas India-WhoReach ManamNo ratings yet
- Does The Positive Psychology Movement Have Legs?Document11 pagesDoes The Positive Psychology Movement Have Legs?nolightxNo ratings yet
- Case Study of Lgu-Po Partnership in Pangantucan, BukidnonDocument23 pagesCase Study of Lgu-Po Partnership in Pangantucan, BukidnonRyan john DanluyanNo ratings yet
- Applied Statistics Basic ConceptsDocument28 pagesApplied Statistics Basic ConceptsYousra OsmanNo ratings yet
- DRRM Research InstrumentDocument5 pagesDRRM Research InstrumentFloribeth PatanganNo ratings yet
- Lecture-3-Fhn-Prelim (1) (20230928161420)Document29 pagesLecture-3-Fhn-Prelim (1) (20230928161420)TEACHERNo ratings yet
- B5 Communicable Diseases Student BookletDocument41 pagesB5 Communicable Diseases Student Booklet2026h.nyamhungaNo ratings yet
- En ProgramDocument13 pagesEn Programghitasenhaji88No ratings yet
- TJ Carrie Workout Guide PowerDocument2 pagesTJ Carrie Workout Guide PowerJacob BanfieldNo ratings yet