You might also like
- Epilepsy in ChildhoodDocument20 pagesEpilepsy in ChildhoodRizky Indah SorayaNo ratings yet
- A Case of Refractory EpilepsyDocument57 pagesA Case of Refractory EpilepsyAdela OkaforNo ratings yet
- Genitourinary TuberculosisDocument16 pagesGenitourinary Tuberculosisdokter.kicikNo ratings yet
- Atypical Absence Seizure Case ReportDocument25 pagesAtypical Absence Seizure Case ReportsyongebobNo ratings yet
- Paleracio Case StudyDocument18 pagesPaleracio Case StudySONY MANDAPNo ratings yet
- Case Presentation 2Document11 pagesCase Presentation 2Angel Jonele ManongsongNo ratings yet
- SEIZURE CASE PROTOCOLDocument1 pageSEIZURE CASE PROTOCOLMarco Paulo Reyes NaoeNo ratings yet
- Case Study On CVADocument54 pagesCase Study On CVAmolukas10186% (7)
- Somnambulism Diagnosis and TreatmentDocument4 pagesSomnambulism Diagnosis and TreatmentfairuzfauziaNo ratings yet
- Grand Rounds Case PresentationDocument13 pagesGrand Rounds Case PresentationMaurice OballoNo ratings yet
- Gouty Arthritis Case PresentationDocument75 pagesGouty Arthritis Case PresentationVan Talawec100% (2)
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- Seizure Disorders in ChildrenDocument18 pagesSeizure Disorders in ChildrenWan AklimaNo ratings yet
- Care Study Chapter 1Document49 pagesCare Study Chapter 1bose olajuyinNo ratings yet
- Pedia Grand CAsEDocument33 pagesPedia Grand CAsEMichael Donn Bulic ApostolNo ratings yet
- Difficulty in Speech After StrokeDocument6 pagesDifficulty in Speech After StrokeAJ RegaladoNo ratings yet
- Hypoglycemia in Children Taking Propranolol For The Treatment of Infantile HemangiomaDocument4 pagesHypoglycemia in Children Taking Propranolol For The Treatment of Infantile HemangiomaAnnisaa RizqiyanaNo ratings yet
- Huma Mir-1Document51 pagesHuma Mir-1drw72409No ratings yet
- Child Hood Seizuer ManagmantDocument78 pagesChild Hood Seizuer Managmantsentayehu siyumNo ratings yet
- Case Study On Scarlet Fever12Document36 pagesCase Study On Scarlet Fever12Mark Sherwin LazoNo ratings yet
- Congenital Hypothyroidism Follow Up of A Case For 13 Years PDFDocument14 pagesCongenital Hypothyroidism Follow Up of A Case For 13 Years PDFMeutia sariNo ratings yet
- Guide to Diagnosing and Treating Neonatal ConvulsionsDocument42 pagesGuide to Diagnosing and Treating Neonatal ConvulsionsG Venkatesh100% (1)
- AANP PRACTICE QUESTIONS AND ANSWERSDocument32 pagesAANP PRACTICE QUESTIONS AND ANSWERSanahmburu966No ratings yet
- Thornton 2016Document5 pagesThornton 2016AfdhalRuslanNo ratings yet
- 631-Article Text-2378-1-10-20180830Document6 pages631-Article Text-2378-1-10-20180830azizhamoudNo ratings yet
- Post-op Care Pituitary TumorDocument4 pagesPost-op Care Pituitary TumorAbdul Hamid NoorNo ratings yet
- Simple Febrile SeizureDocument63 pagesSimple Febrile SeizureMary Ann SacramentoNo ratings yet
- Case History The Chief Complaint (CC)Document18 pagesCase History The Chief Complaint (CC)21912664No ratings yet
- Case #1: Current Visit: 23 Year Old Man Returns For Follow Up Having Been Last Seen Six Months Ago. He Reports No ChangeDocument11 pagesCase #1: Current Visit: 23 Year Old Man Returns For Follow Up Having Been Last Seen Six Months Ago. He Reports No ChangeRehan SaleemNo ratings yet
- Case Report: Adolescent Catatonia Successfully Treated With Lorazepam and AripiprazoleDocument5 pagesCase Report: Adolescent Catatonia Successfully Treated With Lorazepam and AripiprazoleTarraNo ratings yet
- Neonatal Seizures and Management: Dhaka Sishu Hospital BangladeshDocument19 pagesNeonatal Seizures and Management: Dhaka Sishu Hospital BangladeshGoha BashaNo ratings yet
- Neurology History and ExaminationDocument35 pagesNeurology History and ExaminationPhilemon ChizororoNo ratings yet
- Case Scenario No.11 Acetaminophen PoisoningDocument2 pagesCase Scenario No.11 Acetaminophen PoisoningKiara Denise TamayoNo ratings yet
- CP PPT 10-11-11Document49 pagesCP PPT 10-11-11Eaht QuirongNo ratings yet
- Epilepsy Presentation1Document19 pagesEpilepsy Presentation1Daneshwari SahuNo ratings yet
- Case Scenario For Different Groups PDFDocument8 pagesCase Scenario For Different Groups PDFWallen Jey VelascoNo ratings yet
- 28099453C Case Study 3Document27 pages28099453C Case Study 3Alice HuiiNo ratings yet
- SeizuresDocument7 pagesSeizuresSaf Tanggo DiampuanNo ratings yet
- Case PresentatipnDocument58 pagesCase PresentatipnBryan Anthony Boyer ElepanoNo ratings yet
- Massive Lamotrigine Poisoning. A Case ReportDocument3 pagesMassive Lamotrigine Poisoning. A Case ReportDel Rio LauraNo ratings yet
- Case Study 3Document27 pagesCase Study 3jazmae100% (2)
- Case Study Uro FinalDocument44 pagesCase Study Uro FinalDan Ataniel EnsaladaNo ratings yet
- Hypoxic-Ischemic Encephalopathy: DR Mohammad Al-Maghayreh Princess Rahma Teaching HospitalDocument44 pagesHypoxic-Ischemic Encephalopathy: DR Mohammad Al-Maghayreh Princess Rahma Teaching HospitalmohdmaghyrehNo ratings yet
- STROKE RISK FACTORSDocument16 pagesSTROKE RISK FACTORSEmuelle GanNo ratings yet
- PEDIATRICSDocument14 pagesPEDIATRICSbefibo6221No ratings yet
- Cim Adem Rough DraftDocument88 pagesCim Adem Rough DraftKurt CabahugNo ratings yet
- Case English 1 - NDI Edit 220419Document24 pagesCase English 1 - NDI Edit 220419syongebobNo ratings yet
- AmiodaroneDocument2 pagesAmiodaronematin5No ratings yet
- Case Study SlideshowDocument48 pagesCase Study Slideshowapi-3342471330% (1)
- Status EpilepticusDocument21 pagesStatus EpilepticusbushraNo ratings yet
- CBD NeuropediatriDocument34 pagesCBD NeuropediatriyayanaryanNo ratings yet
- 05 Central Nervous SystemDocument70 pages05 Central Nervous SystemThetnaungsoeNo ratings yet
- Drugs For Epilepsy: Subgroup 6Document31 pagesDrugs For Epilepsy: Subgroup 6Kwadwo Sarpong JnrNo ratings yet
- Neonatal SeizuresDocument12 pagesNeonatal Seizuresneeta rajesh bhide100% (2)
- Seminar On SEDocument49 pagesSeminar On SEmubarak abdulkadirNo ratings yet
- 1311 IjirmsDocument4 pages1311 Ijirmsbayekha04No ratings yet
- Erythropoietin Monotherapy in Perinatal Asphyxia With Moderate To Severe Encephalopathy: A Randomized Placebo-Controlled TrialDocument25 pagesErythropoietin Monotherapy in Perinatal Asphyxia With Moderate To Severe Encephalopathy: A Randomized Placebo-Controlled TrialSuci PurnamaNo ratings yet
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- Bertamino2017. Hemophilia Care in The Pediatric AgeDocument13 pagesBertamino2017. Hemophilia Care in The Pediatric AgebobkevinNo ratings yet
- Parenteral Nutrition 280308 PDFDocument18 pagesParenteral Nutrition 280308 PDFBojan BjelajacNo ratings yet
- Higiene Sanitasi Pangan Dit Gizi1Document96 pagesHigiene Sanitasi Pangan Dit Gizi1Sri WidyaNo ratings yet
- Breastfeeding Faqs HivDocument6 pagesBreastfeeding Faqs HivbobkevinNo ratings yet
- MGT of MalnutritionDocument50 pagesMGT of MalnutritionadekjimNo ratings yet
- Suplemen ZN FeDocument6 pagesSuplemen ZN FebobkevinNo ratings yet
- Suplemen FeDocument9 pagesSuplemen FebobkevinNo ratings yet
- Efect of Metformin On Vascular Function in Children With Type 1 Diabetes A Twelve Month RCT 2017Document9 pagesEfect of Metformin On Vascular Function in Children With Type 1 Diabetes A Twelve Month RCT 2017bobkevinNo ratings yet
- Nagel 2013Document5 pagesNagel 2013bobkevinNo ratings yet
- Revel-Vilk 2004. Efect On Intracranial Bleeds and Quality Life of Boys With HemofiliaDocument6 pagesRevel-Vilk 2004. Efect On Intracranial Bleeds and Quality Life of Boys With HemofiliabobkevinNo ratings yet
- JCM 06 00054 v2Document13 pagesJCM 06 00054 v2Yuliawati HarunaNo ratings yet
- Guideline Who2004Document52 pagesGuideline Who2004bobkevinNo ratings yet
- Grafik CDCDocument10 pagesGrafik CDCArief Budi LesmanaNo ratings yet
- Kumar2018 Comparison Persepsin, PCT and CRPDocument3 pagesKumar2018 Comparison Persepsin, PCT and CRPbobkevinNo ratings yet
- PneumothoraxDocument6 pagesPneumothoraxbobkevinNo ratings yet
- 10.1542@Peds.2012-0764.PDF Junal Nutrition 1Document9 pages10.1542@Peds.2012-0764.PDF Junal Nutrition 1bobkevinNo ratings yet
- Kumar2018 Comparison Persepsin, PCT and CRPDocument3 pagesKumar2018 Comparison Persepsin, PCT and CRPbobkevinNo ratings yet
- Early Assessment of Ambiguous GenitaliaDocument7 pagesEarly Assessment of Ambiguous Genitaliaduicu carmenNo ratings yet
- Genetik Konseling Pada PJBDocument26 pagesGenetik Konseling Pada PJBbobkevinNo ratings yet
- GL Paed Renogram 2011Document14 pagesGL Paed Renogram 2011bobkevinNo ratings yet
- Cah PDFDocument13 pagesCah PDFbobkevinNo ratings yet
- Cah PDFDocument13 pagesCah PDFbobkevinNo ratings yet
- Cough Pathophysiology: Pediatric Respirology Working GroupDocument27 pagesCough Pathophysiology: Pediatric Respirology Working GroupbobkevinNo ratings yet
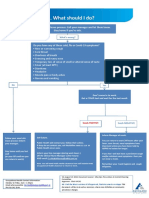
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Chronic Lower Extremity Lymphedema EvaluationDocument2 pagesChronic Lower Extremity Lymphedema Evaluation832000No ratings yet
- 1-Dengue Antigen NS1, IgG & IgM - PO1576121305-961 PDFDocument16 pages1-Dengue Antigen NS1, IgG & IgM - PO1576121305-961 PDFArijit GoraiNo ratings yet
- Common ICD 10 CodesDocument2 pagesCommon ICD 10 CodesAhmadNo ratings yet
- Faduma Case Study - Child with Pneumonia, Dehydration, Ear Infection & MalnutritionDocument16 pagesFaduma Case Study - Child with Pneumonia, Dehydration, Ear Infection & MalnutritionKhyla ValenzuelaNo ratings yet
- Prodige 23Document14 pagesProdige 23josebaNo ratings yet
- The Different Perspectives of DisasterDocument27 pagesThe Different Perspectives of DisasterWincer CaballesNo ratings yet
- WK6 Asthma Assignment Student VersionDocument8 pagesWK6 Asthma Assignment Student Versionnalit1985No ratings yet
- SEMINARDocument31 pagesSEMINARDeveshNo ratings yet
- Ringworm in CatsDocument4 pagesRingworm in CatsZain AsifNo ratings yet
- J Jacc 2023 02 011Document3 pagesJ Jacc 2023 02 011Evania BeatriceNo ratings yet
- The Influence of Spleen On Portal HemodynamicsDocument1 pageThe Influence of Spleen On Portal HemodynamicsdenisegmeloNo ratings yet
- Iub 9999 0Document13 pagesIub 9999 0Simona VisanNo ratings yet
- Effect of Constraint Induced Movement Therapy Versus Motor Relearning Programme To Enhance Upper Limb Motor Function in Stroke Patients: A Quasi Experimental StudyDocument7 pagesEffect of Constraint Induced Movement Therapy Versus Motor Relearning Programme To Enhance Upper Limb Motor Function in Stroke Patients: A Quasi Experimental StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ais Student Medical and Health Declaration Form 2023-24Document7 pagesAis Student Medical and Health Declaration Form 2023-24hafizvy6No ratings yet
- Topic 3 - Microbial DIsease of Digestive SystemDocument106 pagesTopic 3 - Microbial DIsease of Digestive SystemJewel YvonneNo ratings yet
- Ziprasidone Drug StudyDocument4 pagesZiprasidone Drug Studyshadow gonzalez100% (1)
- Lecture 1 Cancer IntroductionDocument18 pagesLecture 1 Cancer IntroductionShreeyaNo ratings yet
- The Acute Hemoabdomen: Topic OverviewDocument23 pagesThe Acute Hemoabdomen: Topic OverviewWeiwei CierraNo ratings yet
- ATI RN Mental Health Online Practice BDocument38 pagesATI RN Mental Health Online Practice Bseansdrew2No ratings yet
- Pandemic ExpressDocument3 pagesPandemic ExpressGabriel KawaiNo ratings yet
- MahamTahir PDFDocument6 pagesMahamTahir PDFAdeel AizadNo ratings yet
- First Aid & Bandaging Techniques GuideDocument35 pagesFirst Aid & Bandaging Techniques GuideJoel VelasquezNo ratings yet
- CA CervixDocument54 pagesCA CervixsesiaNo ratings yet
- P.A. Tool (Case Pres FINAL.)Document23 pagesP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonNo ratings yet
- Argumentitive Essay About Bariatric SurgeryDocument2 pagesArgumentitive Essay About Bariatric SurgeryNourNo ratings yet
- Chap 26 - Assessing Male Genitalia (Interview Guide)Document3 pagesChap 26 - Assessing Male Genitalia (Interview Guide)Mary Cielo DomagasNo ratings yet
- About Cervical Cancer: Overview and TypesDocument9 pagesAbout Cervical Cancer: Overview and TypesAlexa jaye BalinoNo ratings yet
- 99 Series QueDocument9 pages99 Series QueVijay UNo ratings yet
- Topic 2Document2 pagesTopic 2Joshua PanganNo ratings yet