You might also like
- RLE 118 REVISED Case Scenario No. 10 Anaphylactic ShockDocument2 pagesRLE 118 REVISED Case Scenario No. 10 Anaphylactic ShockKiara Denise TamayoNo ratings yet
- AcetapoisoningDocument14 pagesAcetapoisoningKirstin del CarmenNo ratings yet
- Nursing Care of a Client with Gastrointestinal BleedingDocument3 pagesNursing Care of a Client with Gastrointestinal BleedingnicoleNo ratings yet
- 6 Ashkin 062012Document79 pages6 Ashkin 062012Anonymous QPXAgjBwNo ratings yet
- AANP PRACTICE QUESTIONS AND ANSWERSDocument32 pagesAANP PRACTICE QUESTIONS AND ANSWERSanahmburu966No ratings yet
- Thornton 2016Document5 pagesThornton 2016AfdhalRuslanNo ratings yet
- Cue Card Kevin 130920Document6 pagesCue Card Kevin 130920bobkevinNo ratings yet
- tmp2CD0 TMPDocument4 pagestmp2CD0 TMPFrontiersNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument4 pagesPregnancy Induced Hypertension Case StudyMae Arra Lecobu-anNo ratings yet
- Hypoglycemia in Children Taking Propranolol For The Treatment of Infantile HemangiomaDocument4 pagesHypoglycemia in Children Taking Propranolol For The Treatment of Infantile HemangiomaAnnisaa RizqiyanaNo ratings yet
- Pleural Effusion Case PresentationDocument78 pagesPleural Effusion Case PresentationAnie Zacarias100% (3)
- NCP PneumoniaDocument47 pagesNCP Pneumoniabhevpat251100% (1)
- Nursing Care Plan for Mrs. Yolanda Yambut BenavidezDocument8 pagesNursing Care Plan for Mrs. Yolanda Yambut BenavidezRafi LabNo ratings yet
- Chronic Renal Failure 7Document22 pagesChronic Renal Failure 7Madelyn SerneoNo ratings yet
- Pathology I Review 10Document30 pagesPathology I Review 10i_areinamoNo ratings yet
- Clinical ExemplarDocument5 pagesClinical Exemplarapi-371817203No ratings yet
- ALF 418RLE Group1Document22 pagesALF 418RLE Group1PAOLA LUZ CRUZNo ratings yet
- ALF 418RLE Group1Document21 pagesALF 418RLE Group1PAOLA LUZ CRUZNo ratings yet
- Patient Profile and Appendicitis ManagementDocument7 pagesPatient Profile and Appendicitis ManagementAiman ArifinNo ratings yet
- Tympanic Membrane and Thyroid GlandDocument9 pagesTympanic Membrane and Thyroid GlandSammy ChegeNo ratings yet
- Paleracio Case StudyDocument18 pagesPaleracio Case StudySONY MANDAPNo ratings yet
- MRCPCH Part Ii: Safdar Iqbal'sDocument5 pagesMRCPCH Part Ii: Safdar Iqbal'sGalaleldin AliNo ratings yet
- Danganan Protocol Ver 2Document7 pagesDanganan Protocol Ver 2FayeListancoNo ratings yet
- NCMB312 - : Bachelor of Science in Nursing: Communicable Disease NursingDocument7 pagesNCMB312 - : Bachelor of Science in Nursing: Communicable Disease NursingMichelle Gliselle Guinto MallareNo ratings yet
- FEB 2023Document11 pagesFEB 2023Parsaant SinghNo ratings yet
- Case Study: Obstructive JaundiceDocument11 pagesCase Study: Obstructive JaundiceZhy CaluzaNo ratings yet
- F2F MeaslesDocument7 pagesF2F MeaslesMichelle Gliselle Guinto MallareNo ratings yet
- Case English 1 - NDI Edit 220419Document24 pagesCase English 1 - NDI Edit 220419syongebobNo ratings yet
- Major Case 3Document3 pagesMajor Case 3Christine Evan HoNo ratings yet
- 10 1089@cap 2016 0178Document2 pages10 1089@cap 2016 0178Maria Helena Pedraza MNo ratings yet
- PBL WEEK 5 - SCDocument10 pagesPBL WEEK 5 - SCJesselyn ReginaNo ratings yet
- Genitourinary TuberculosisDocument16 pagesGenitourinary Tuberculosisdokter.kicikNo ratings yet
- Presentation of CaseDocument10 pagesPresentation of CaseAmazonJambiNo ratings yet
- Bank Manager's Gastritis CaseDocument4 pagesBank Manager's Gastritis CaseMarissa AsimNo ratings yet
- Tuberculosis and Nephrotic Syndrome in a ChildDocument34 pagesTuberculosis and Nephrotic Syndrome in a ChildAldo YustiantoNo ratings yet
- Empyema ThoracisDocument14 pagesEmpyema ThoracisMara AbantoNo ratings yet
- Sheehan Syndrome Sarina SchragerDocument3 pagesSheehan Syndrome Sarina Schragerfreddyop72No ratings yet
- Shelf IM Patient NotesDocument6 pagesShelf IM Patient NotesRuth SanmooganNo ratings yet
- Grand Rounds Case PresentationDocument13 pagesGrand Rounds Case PresentationMaurice OballoNo ratings yet
- PCOS Patient with FatigueDocument9 pagesPCOS Patient with FatiguelorrainebarandonNo ratings yet
- Intestinal Amoebiasis CSDocument34 pagesIntestinal Amoebiasis CSabigailxDNo ratings yet
- Case Hernia2Document19 pagesCase Hernia2ejkohNo ratings yet
- Hydatidiform Mole With Hyperthyroidism - Perioperative ChallengesDocument2 pagesHydatidiform Mole With Hyperthyroidism - Perioperative ChallengesAl MubartaNo ratings yet
- Irene's Care StudyDocument68 pagesIrene's Care StudyLawrence AckahNo ratings yet
- Case Study On Scarlet Fever12Document36 pagesCase Study On Scarlet Fever12Mark Sherwin LazoNo ratings yet
- Complete SOAP Note for 39-Year-Old Female with Nausea and VomitingDocument6 pagesComplete SOAP Note for 39-Year-Old Female with Nausea and VomitingLorrie83% (6)
- Case Presentation 2Document11 pagesCase Presentation 2Angel Jonele ManongsongNo ratings yet
- Ectopic Pregnancy Nursing CareDocument27 pagesEctopic Pregnancy Nursing CareEduard GarchitorenaNo ratings yet
- 3 End of Life Gipsy GenesDocument2 pages3 End of Life Gipsy GenesADRIAN ISAAC GARZON PEREZNo ratings yet
- Case # 2Document3 pagesCase # 2Jay VillasotoNo ratings yet
- Case Study 2.2Document1 pageCase Study 2.2Elfira Wahyuningsih50% (2)
- Gastroenteritis Care StudyDocument13 pagesGastroenteritis Care StudyÄxxö Ahkö Hinoguin50% (2)
- Pathophysiology of Pituitary For StudentsDocument34 pagesPathophysiology of Pituitary For StudentsVisura PrabodNo ratings yet
- fped-09-655010Document4 pagesfped-09-655010dr.yogaNo ratings yet
- Nursing Care for Hepatic EncephalopathyDocument14 pagesNursing Care for Hepatic EncephalopathyClarisse AcacioNo ratings yet
- Case Study 8th July 2021Document1 pageCase Study 8th July 2021sivakamasundari pichaipillaiNo ratings yet
- 2019 IteDocument188 pages2019 IteBHNo ratings yet
- CS - UTI, Acute Bronchitis, Acute GastritisDocument39 pagesCS - UTI, Acute Bronchitis, Acute GastritisGrace BernadetteNo ratings yet
- Reye's Syndrome Case StudyDocument3 pagesReye's Syndrome Case Studyapi-591190687No ratings yet
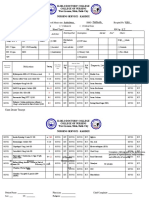
- Iloilo Doctors' College Nursing Service KardexDocument4 pagesIloilo Doctors' College Nursing Service KardexKiara Denise TamayoNo ratings yet
- Kardex - End Stage Renal FailureDocument5 pagesKardex - End Stage Renal FailureKiara Denise TamayoNo ratings yet
- Kardex - Traumatic Spine InjuryDocument5 pagesKardex - Traumatic Spine InjuryKiara Denise TamayoNo ratings yet
- Iloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City NURSING CARE PLAN - Acute PancreatitisDocument2 pagesIloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City NURSING CARE PLAN - Acute PancreatitisKiara Denise TamayoNo ratings yet
- Kardex - Acute PancreatitisDocument5 pagesKardex - Acute PancreatitisKiara Denise TamayoNo ratings yet
- Iloilo Doctors' College Nursing Finals Case on Gastric Outlet ObstructionDocument3 pagesIloilo Doctors' College Nursing Finals Case on Gastric Outlet ObstructionKiara Denise TamayoNo ratings yet
- Jenny Brown: Bowen Family Systems Theory and Practice: Illustration and CritiqueDocument10 pagesJenny Brown: Bowen Family Systems Theory and Practice: Illustration and CritiqueMari Forgach100% (1)
- Philippine school nutrition plan for 2020-2021Document4 pagesPhilippine school nutrition plan for 2020-2021Maeva LimbagaNo ratings yet
- Welfare and Development Section (WDS)Document6 pagesWelfare and Development Section (WDS)Darwin Patricio100% (1)
- Of Mice and MenDocument12 pagesOf Mice and MenAkshitaa PandeyNo ratings yet
- Course Outline PBH 101 MW 18Document7 pagesCourse Outline PBH 101 MW 18FAYAZ AHMEDNo ratings yet
- Practice Sheet Session 2 - 2021 - Student SheetDocument2 pagesPractice Sheet Session 2 - 2021 - Student SheetAlisa SayNo ratings yet
- State of Colorado: First Regular Session Seventy-Third General AssemblyDocument15 pagesState of Colorado: First Regular Session Seventy-Third General AssemblyMichael_Roberts2019No ratings yet
- Columbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeDocument1 pageColumbia-Suicide Severity Rating Scale (C-SSRS) : Past 3 Months LifetimeIzabel EstevamNo ratings yet
- Annual Record of Homœopathic Literature.1875Document395 pagesAnnual Record of Homœopathic Literature.1875GustavoMarceloDareNo ratings yet
- Lesbian Sex Tips and Sensual Lovemaking : Female Sexual Pleasure TipsDocument20 pagesLesbian Sex Tips and Sensual Lovemaking : Female Sexual Pleasure Tipslesbianlovemaking24% (42)
- Full Download Test Bank For The Sociology of Health Illness and Health Care A Critical Approach 7th Edition PDF Full ChapterDocument35 pagesFull Download Test Bank For The Sociology of Health Illness and Health Care A Critical Approach 7th Edition PDF Full Chapterforceepipubica61uxl95% (21)
- AugerTorque European Trencher Operators ManualDocument23 pagesAugerTorque European Trencher Operators ManualПавел ХромовNo ratings yet
- 10 Things I Would Do If I Were A CelebrityDocument3 pages10 Things I Would Do If I Were A CelebrityAnne Marian JosephNo ratings yet
- Cebu Doctors' University Intro to RT Program & Rehab SciencesDocument2 pagesCebu Doctors' University Intro to RT Program & Rehab SciencesMa.Emmagrace JaldonNo ratings yet
- Assessing Animal Housing and Management in a LaboratoryDocument22 pagesAssessing Animal Housing and Management in a Laboratoryrifky waskitoNo ratings yet
- (Lecture 2) Skin TestDocument31 pages(Lecture 2) Skin TestShubham KadiwalaNo ratings yet
- Effective Leadership Theory Cases and Applications 1st Edition Humphrey Test BankDocument9 pagesEffective Leadership Theory Cases and Applications 1st Edition Humphrey Test Bankhillyobsidian8hi42g100% (36)
- Planning ProcessDocument9 pagesPlanning ProcessSimran JosanNo ratings yet
- Power Point Consumer Health EducationDocument81 pagesPower Point Consumer Health EducationAlbert Ian CasugaNo ratings yet
- Differences and similarities among the three dopamine receptor partial agonistsDocument10 pagesDifferences and similarities among the three dopamine receptor partial agonistsolivukovic100% (1)
- Hope Week 2Document5 pagesHope Week 2Bea CabacunganNo ratings yet
- A Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItDocument1 pageA Quick Guide For Busy Parents: Connect and Re-Direct Name It To Tame ItSanjeev Sharma100% (2)
- Battery MSDSDocument3 pagesBattery MSDSAnkitNo ratings yet
- 1 Caixin Lei PSY 2012 General PsychologyDocument2 pages1 Caixin Lei PSY 2012 General PsychologyKaty LeiNo ratings yet
- Pestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementDocument15 pagesPestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementshubhamNo ratings yet
- TAROSANAN-Sub-Project-Completion-Report Dec. 20, 2023Document16 pagesTAROSANAN-Sub-Project-Completion-Report Dec. 20, 2023Mara Kenia BarcelonNo ratings yet
- MAPEH Daily Lesson LogDocument11 pagesMAPEH Daily Lesson LogMARTIN YUI LOPEZNo ratings yet
- Reducing AgeismDocument2 pagesReducing AgeismAntónio LealNo ratings yet
- BS BuzzDocument10 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- The Best Lifts For Real World Strength & Strongman CompetitionDocument3 pagesThe Best Lifts For Real World Strength & Strongman CompetitionIlijaNo ratings yet