You might also like
- Physicians 10-2023Document27 pagesPhysicians 10-2023PRC Baguio100% (1)
- Cranial Nerves AssessmentDocument3 pagesCranial Nerves AssessmentNursesLabs.comNo ratings yet
- List of Nursing OrganizationsDocument3 pagesList of Nursing OrganizationsShehada Marcos BondadNo ratings yet
- Sasaran & Program Kerja K3L 2018 PT. HOCO (Rev.1)Document1 pageSasaran & Program Kerja K3L 2018 PT. HOCO (Rev.1)dennisjuntakNo ratings yet
- Sleep Deprivation and School QuestionnaireDocument2 pagesSleep Deprivation and School Questionnairethe-big-g92% (25)
- Diagnostic Accuracy of Zero-Echo Time MRI For The Evaluation of Cervical Neural Foraminal StenosisDocument20 pagesDiagnostic Accuracy of Zero-Echo Time MRI For The Evaluation of Cervical Neural Foraminal StenosisThiago Astil RizzettoNo ratings yet
- CT MRI TBsadadDocument5 pagesCT MRI TBsadadArief RachmanNo ratings yet
- Angioleiomyoma in Soft Tissue of Extremities: MRI FindingsDocument4 pagesAngioleiomyoma in Soft Tissue of Extremities: MRI FindingsLuis Javier del PozoNo ratings yet
- 1369 Full PDFDocument9 pages1369 Full PDFIqbal AbdillahNo ratings yet
- Spec MRI Distinguish Acue TM of NMOSD N Infarction. Kister Et Al 2015Document21 pagesSpec MRI Distinguish Acue TM of NMOSD N Infarction. Kister Et Al 2015Ido BramantyaNo ratings yet
- Displasia Cortical de TaylorDocument11 pagesDisplasia Cortical de TaylorOscar F. Ochoa RuizNo ratings yet
- Incidental Findings of The Lumbar Spine at MRI During Herniated Intervertebral Disk Disease EvaluationDocument5 pagesIncidental Findings of The Lumbar Spine at MRI During Herniated Intervertebral Disk Disease EvaluationDyah Gaby KesumaNo ratings yet
- Seguridad Social en AlemaniaDocument8 pagesSeguridad Social en AlemaniaMichael RojasNo ratings yet
- Jms 21041483Document28 pagesJms 21041483Afra Eslis NoatoNo ratings yet
- Magnetic Resonance Imaging For The Detection of Nasopharyngeal CarcinomaDocument4 pagesMagnetic Resonance Imaging For The Detection of Nasopharyngeal CarcinomaFebri W FinisiaNo ratings yet
- Tumores en CuelloDocument6 pagesTumores en CuellokalixinNo ratings yet
- Primitive Neuroectodermal Tumors: A Clinical and Radiological Analysis of Six CasesDocument8 pagesPrimitive Neuroectodermal Tumors: A Clinical and Radiological Analysis of Six CasestaufikolingNo ratings yet
- Fibrosing Inflammatory Pseudotumors Involving The Skull Base: MR and CT Manifestations With Histopathologic ComparisonDocument7 pagesFibrosing Inflammatory Pseudotumors Involving The Skull Base: MR and CT Manifestations With Histopathologic ComparisonNicolas SaputraNo ratings yet
- CT and MR Imaging Features of Primary Central Nervous System Lymphoma in Norway, 1989-2003Document8 pagesCT and MR Imaging Features of Primary Central Nervous System Lymphoma in Norway, 1989-2003Alfina RahmiNo ratings yet
- Neurol J Southeast Asia 1999 4: 83 - 88: LCS Tan, YY Sitoh, HTL TjiaDocument6 pagesNeurol J Southeast Asia 1999 4: 83 - 88: LCS Tan, YY Sitoh, HTL Tjiarani suwadjiNo ratings yet
- Bone Marrow Edema Syndrome 1Document8 pagesBone Marrow Edema Syndrome 1drbane123No ratings yet
- Diagnosis and Classification in MRI of Brucellar SpondylitisDocument6 pagesDiagnosis and Classification in MRI of Brucellar SpondylitisMANGNo ratings yet
- Distinguishing Benign Notochordal Cell Tumors From Vertebral ChordomaDocument9 pagesDistinguishing Benign Notochordal Cell Tumors From Vertebral ChordomaOM JHANo ratings yet
- MR IntracranIal menIngIomas!!! Vazno!!!Document5 pagesMR IntracranIal menIngIomas!!! Vazno!!!StefanNo ratings yet
- Imaging of The Scrotum: Beyond SonographyDocument12 pagesImaging of The Scrotum: Beyond Sonographyasriani DewiNo ratings yet
- Primary Extraskeletal Ewing Sarcoma of The Sinonasal Tract - A Rare Case Report and Review of The LiteratureDocument7 pagesPrimary Extraskeletal Ewing Sarcoma of The Sinonasal Tract - A Rare Case Report and Review of The LiteraturemohammadsayfooNo ratings yet
- Pulsed Electromagnetic Field in Patients With Shoulder Impingement SyndromeDocument6 pagesPulsed Electromagnetic Field in Patients With Shoulder Impingement SyndromeHanna RikaswaniNo ratings yet
- The Diagnostic Relationship With Clinical and Neuroimaging Studies of Patients With Back PainDocument5 pagesThe Diagnostic Relationship With Clinical and Neuroimaging Studies of Patients With Back PainCentral Asian StudiesNo ratings yet
- Imaging in RadiculopathyDocument17 pagesImaging in RadiculopathyFerdy DamaraNo ratings yet
- Bone MarrowDocument5 pagesBone MarrowDanaAmaranducaiNo ratings yet
- Sipola. Detection and Quantification of Rotator Cuff Tears With Ultrasonography and Magnetic Resonance Imaging - A ProsDocument9 pagesSipola. Detection and Quantification of Rotator Cuff Tears With Ultrasonography and Magnetic Resonance Imaging - A Prossteven saputraNo ratings yet
- Spinal Tuberculosis: Imaging Features On MRIDocument6 pagesSpinal Tuberculosis: Imaging Features On MRIEster JuanitaNo ratings yet
- Scientific Abstracts Friday, 14 June 2019 1015Document1 pageScientific Abstracts Friday, 14 June 2019 1015حسام الدين إسماعيلNo ratings yet
- Proton Magnetic Resonance Spectroscopy MRS of Metastatic Brain TumorsDocument10 pagesProton Magnetic Resonance Spectroscopy MRS of Metastatic Brain TumorsolgaNo ratings yet
- Kiuru 2002Document6 pagesKiuru 2002Laraib KanwalNo ratings yet
- Space Occupying Lesions of Central Nervous System: A Radiological and Histopathological CorrelationDocument6 pagesSpace Occupying Lesions of Central Nervous System: A Radiological and Histopathological CorrelationRaja WartegNo ratings yet
- Payer 2015Document10 pagesPayer 2015esinsubozatliNo ratings yet
- Vertebral Endplate Change As A Feature of Intervertebral Disc Degeneration: A Heritability StudyDocument7 pagesVertebral Endplate Change As A Feature of Intervertebral Disc Degeneration: A Heritability StudySitti Hajar ArdasNo ratings yet
- SAVULESCU Et Al 2021 Rpms of Lumbar Area Effective On Radiculopathy PainDocument5 pagesSAVULESCU Et Al 2021 Rpms of Lumbar Area Effective On Radiculopathy PainperruchoudNo ratings yet
- Osteoradionecrosis of The Subaxial Cervical Spine Following Treatment For Head and Neck CarcinomasDocument8 pagesOsteoradionecrosis of The Subaxial Cervical Spine Following Treatment For Head and Neck CarcinomasakreditasiNo ratings yet
- Keller Et Al 2011 EpilepsiaDocument10 pagesKeller Et Al 2011 EpilepsiaLaura Gonzalez TamayoNo ratings yet
- Ewing'S Sarcoma: Imaging FeaturesDocument9 pagesEwing'S Sarcoma: Imaging FeaturesRachelMayaMalauNo ratings yet
- Intracranial Yolk Sac Tumor in An Adult Patient: MRI, Diffusion-Weighted Imaging and H MR Spectroscopy FeaturesDocument4 pagesIntracranial Yolk Sac Tumor in An Adult Patient: MRI, Diffusion-Weighted Imaging and H MR Spectroscopy FeaturestiaraNo ratings yet
- 2018 Ultrasonido Terapéutico Con Medición en Pacientes Con RadiculopatíaDocument8 pages2018 Ultrasonido Terapéutico Con Medición en Pacientes Con RadiculopatíaCarlos JaimeNo ratings yet
- Two Decades of Advances in Muscle Imaging in Children From P - 2021 - NeuromuscDocument13 pagesTwo Decades of Advances in Muscle Imaging in Children From P - 2021 - NeuromuscSuzie Simone Mardones SilvaNo ratings yet
- Primary Leiomyosarcoma of The Spine: An Analysis of Imaging Manifestations and Clinicopathological FindingsDocument9 pagesPrimary Leiomyosarcoma of The Spine: An Analysis of Imaging Manifestations and Clinicopathological Findingst7xs5mchfzNo ratings yet
- MRI Findings of 26 Patients With Parsonage-Turner SyndromeDocument6 pagesMRI Findings of 26 Patients With Parsonage-Turner SyndromeTopciu Mihaela FeliciaNo ratings yet
- MRI SeizuresDocument7 pagesMRI SeizuresMarco MalagaNo ratings yet
- Diagnosis of Carpal Tunnel SyndromeDocument11 pagesDiagnosis of Carpal Tunnel SyndromeMrAppleNo ratings yet
- Diagnostic Utility of Ultrasonography Versus Nerve Conduction Studies in Mild Carpal Tunnel SyndromeDocument10 pagesDiagnostic Utility of Ultrasonography Versus Nerve Conduction Studies in Mild Carpal Tunnel SyndromeJP ChenNo ratings yet
- Z Score SISCOMDocument9 pagesZ Score SISCOMAiswarya HariNo ratings yet
- Reliability of Diagnosis of Soft Cervical Disc Prolapse Using Spurling's TestDocument5 pagesReliability of Diagnosis of Soft Cervical Disc Prolapse Using Spurling's Testapi-479716004No ratings yet
- JournalDocument6 pagesJournalmandipNo ratings yet
- Kerasnoudis 2014Document10 pagesKerasnoudis 2014Laura A M MNo ratings yet
- 0040JKSMRM JKSMRM 17 8Document11 pages0040JKSMRM JKSMRM 17 8M P ChakravortyNo ratings yet
- Clavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseDocument6 pagesClavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseAngel IschiaNo ratings yet
- RNM Dinamica 2Document6 pagesRNM Dinamica 2Alfredo GuiroyNo ratings yet
- Radiol 2332031111Document8 pagesRadiol 2332031111nimaelhajjiNo ratings yet
- Clinical Neurophysiology: Yukiko Tsuji, Yu-Ichi Noto, Takamasa Kitaoji, Yuta Kojima, Toshiki MizunoDocument5 pagesClinical Neurophysiology: Yukiko Tsuji, Yu-Ichi Noto, Takamasa Kitaoji, Yuta Kojima, Toshiki MizunoSerque777No ratings yet
- Clinical Neurophysiology: Yukiko Tsuji, Yu-Ichi Noto, Takamasa Kitaoji, Yuta Kojima, Toshiki MizunoDocument5 pagesClinical Neurophysiology: Yukiko Tsuji, Yu-Ichi Noto, Takamasa Kitaoji, Yuta Kojima, Toshiki MizunoSerque777No ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)Document9 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 2000)zano_adamNo ratings yet
- SDRCIDocument7 pagesSDRCIRensoBerlangaNo ratings yet
- Abnormal Cerebral Structure in Juvenile Myoclonic Epilepsy Demonstrated With Voxel-Based Analysis of MRIDocument7 pagesAbnormal Cerebral Structure in Juvenile Myoclonic Epilepsy Demonstrated With Voxel-Based Analysis of MRIVj McNo ratings yet
- 2016 5 Focus16163 PDFDocument10 pages2016 5 Focus16163 PDFLuwiNo ratings yet
- JBH5 HiccupsDocument5 pagesJBH5 HiccupsAstrid GayatriNo ratings yet
- Berlin QuestionnaireDocument1 pageBerlin QuestionnaireAstrid GayatriNo ratings yet
- Vitamin D and Living in Northern Latitudes An Endemic Risk Area For Vitamin D DeficiencyDocument16 pagesVitamin D and Living in Northern Latitudes An Endemic Risk Area For Vitamin D DeficiencyJu RiNo ratings yet
- 10 1111-cpr 12915figure129150001Document1 page10 1111-cpr 12915figure129150001Astrid GayatriNo ratings yet
- Contoh Pico Terbaru-Blok EndokrinDocument3 pagesContoh Pico Terbaru-Blok EndokrinIndra ArdiansyahNo ratings yet
- Learning Guide 03Document28 pagesLearning Guide 03Mulugeta GirmaNo ratings yet
- Daftar Obat IntersipDocument15 pagesDaftar Obat Intersipleno voNo ratings yet
- Clinic ListDocument34 pagesClinic Listrayd667No ratings yet
- Rekapan Diah Ayu-UHAMKA-DM Tipe 2Document185 pagesRekapan Diah Ayu-UHAMKA-DM Tipe 2DevinaNo ratings yet
- Dt. 02.04.2023 YMA TlangauDocument4 pagesDt. 02.04.2023 YMA TlangaupatsyNo ratings yet
- Npi-Family Case StudyDocument12 pagesNpi-Family Case StudyGayLah MomblancoNo ratings yet
- Daily Undulating Periodisation Plan TemplateDocument6 pagesDaily Undulating Periodisation Plan TemplateJaron KungNo ratings yet
- University of Makati: J.P. Rizal West Rembo Makati CityDocument3 pagesUniversity of Makati: J.P. Rizal West Rembo Makati Citywheng0814No ratings yet
- Peritonitis Et Causa Demam Typhoid: Kelompok D6Document21 pagesPeritonitis Et Causa Demam Typhoid: Kelompok D6Anjas PrabowoNo ratings yet
- TOPIC 10 - 1019031146 UbaidillahDocument8 pagesTOPIC 10 - 1019031146 UbaidillahUbay SegaNo ratings yet
- Assessment Sheet: Critical Care Patient (Icu / Ccu)Document5 pagesAssessment Sheet: Critical Care Patient (Icu / Ccu)Barrak AldosaryNo ratings yet
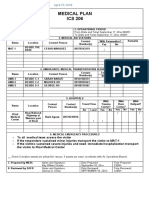
- Ics 206Document1 pageIcs 206Ldrrmo RamonNo ratings yet
- Nonextraction Treatment With Begg TechniqueDocument14 pagesNonextraction Treatment With Begg TechniqueSyed Mohammad Osama AhsanNo ratings yet
- PGM CET 2015 First Round Selection List Dated 30.03.2015Document34 pagesPGM CET 2015 First Round Selection List Dated 30.03.2015Shruthi ShenoyNo ratings yet
- Bowel Prep PresentationDocument14 pagesBowel Prep PresentationnadiarosmanNo ratings yet
- Billing Template and Opd Health PackageDocument8 pagesBilling Template and Opd Health Packagepranit.gumgaonkarNo ratings yet
- Quality Health Services: A Planning GuideDocument64 pagesQuality Health Services: A Planning GuideEdwar RusdiantoNo ratings yet
- Nausea and VomitingDocument3 pagesNausea and VomitingAlthea AlbaniaNo ratings yet
- Presentation IresDocument30 pagesPresentation IresPriyanka Sharma100% (1)
- Sistema ABO, Parte 2Document25 pagesSistema ABO, Parte 2juan pablo padgetNo ratings yet
- Merancang Klinik Kedokteran KeluargaDocument29 pagesMerancang Klinik Kedokteran KeluargaLuthfiyah SalsabillaNo ratings yet
- Annexure Panchkarma - 1st EditionDocument228 pagesAnnexure Panchkarma - 1st EditionSmita SaxenaNo ratings yet
- Dade InnovinDocument7 pagesDade InnovinchaiNo ratings yet
- Rubrics For Triangular Bandaging TechniqueDocument1 pageRubrics For Triangular Bandaging TechniqueBulan A'tin0% (2)