You might also like
- Nordic Musculoskeletal Questionnaire Form PDFDocument1 pageNordic Musculoskeletal Questionnaire Form PDFkhaista bachaNo ratings yet
- Nordic Musculoskeletal QuestionnaireDocument4 pagesNordic Musculoskeletal Questionnaireحنيف سجد67% (3)
- Rom PDFDocument4 pagesRom PDFenzoNo ratings yet
- Attachment E - Modified Barthel Index - April 2007Document11 pagesAttachment E - Modified Barthel Index - April 2007WasemBhatNo ratings yet
- Range of Motion Exercises: General InstructionsDocument4 pagesRange of Motion Exercises: General InstructionsEma JeffersNo ratings yet
- Forms ErgoMine2.0Document14 pagesForms ErgoMine2.0trevorhutNo ratings yet
- Daily Covid - 19 Symptoms Monitoring Day 2Document2 pagesDaily Covid - 19 Symptoms Monitoring Day 2Rodolf Gerone G. MacahilosNo ratings yet
- Stepladder Inspection LogDocument1 pageStepladder Inspection Logrodolfo rodríguezNo ratings yet
- Standardized Nordic Musculoskeletal Questionnaires (SNMQ) ENGDocument2 pagesStandardized Nordic Musculoskeletal Questionnaires (SNMQ) ENG2021862304No ratings yet
- Cacho Med 1Document3 pagesCacho Med 1Roseann ReyesNo ratings yet
- NCD Risk Assessment FormDocument1 pageNCD Risk Assessment Formruiza corcino100% (4)
- 2021-2022 COVID - 19 Symptom Monitoring Log Revised (1) - Sheet1Document1 page2021-2022 COVID - 19 Symptom Monitoring Log Revised (1) - Sheet1MEGAN RAPHAELA DIRIGENo ratings yet
- Calalas Med 12Document3 pagesCalalas Med 12Roseann ReyesNo ratings yet
- AguilarDocument1 pageAguilarRonald GedorNo ratings yet
- Spine Questionnaire 2020Document5 pagesSpine Questionnaire 2020roxieNo ratings yet
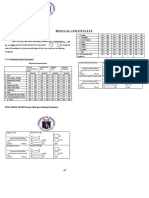
- Medical For Athletes 1 - RevisedDocument2 pagesMedical For Athletes 1 - RevisedRanDave TVNo ratings yet
- Lesson PlanDocument5 pagesLesson Planmaris tulNo ratings yet
- Product Research SpreadsheetDocument7 pagesProduct Research SpreadsheetCharlie ElmesNo ratings yet
- Jesús - Grammar. 1º Eso: English Spanish TO BE - PresentDocument6 pagesJesús - Grammar. 1º Eso: English Spanish TO BE - PresentRosaNo ratings yet
- Mimay MimaropaDocument1 pageMimay MimaropaErrol LlanesNo ratings yet
- Wellness Monitoring Form 1Document1 pageWellness Monitoring Form 1ADRIAN TIMBANCAYA AVILANo ratings yet
- TemplateDocument2 pagesTemplateapi-344149486No ratings yet
- Annex E. Schools Data Summary Template 02.03.23Document4 pagesAnnex E. Schools Data Summary Template 02.03.23Julieta Aragos PingcaNo ratings yet
- Eating Too Match Yes NoDocument1 pageEating Too Match Yes NoJonbert AndamNo ratings yet
- Ehs Weekly Report - Byagwat Raichur - 14.08.2017Document5 pagesEhs Weekly Report - Byagwat Raichur - 14.08.2017nazi1945No ratings yet
- Ambulatory Care Suite PDocument18 pagesAmbulatory Care Suite PKhilmi MaghfuriNo ratings yet
- Reproducible EE (Example)Document1 pageReproducible EE (Example)Daniel KKKNo ratings yet
- Medicalhistoryformpg 1Document2 pagesMedicalhistoryformpg 1reynanfrancebernabeNo ratings yet
- Myelopathy Disability IndexDocument1 pageMyelopathy Disability IndexGabriela Herrera MorenoNo ratings yet
- Medical For Athletes 1Document1 pageMedical For Athletes 1Raymund SuaybaguioNo ratings yet
- Medical For JournalismDocument2 pagesMedical For Journalismarnellloyd.sarabia88No ratings yet
- Facility Risk Assessement Form 2016Document1 pageFacility Risk Assessement Form 2016kojiki67% (3)
- COVID Home CareDocument1 pageCOVID Home Carey2jr784qgsNo ratings yet
- Bultonoon PatDocument1 pageBultonoon PatErrol Llanes100% (1)
- Attachments ListDocument3 pagesAttachments ListDương LêNo ratings yet
- Adaboost: Let's Discuss This Algorithm in DetailDocument56 pagesAdaboost: Let's Discuss This Algorithm in DetailSahar SarrajNo ratings yet
- Untitled Form (Responses)Document3 pagesUntitled Form (Responses)jinkybohol2015No ratings yet
- Revised-PhilPEN-12 28 18Document1 pageRevised-PhilPEN-12 28 18Kristine TanNo ratings yet
- Health Declaration Form 1Document1 pageHealth Declaration Form 1April Mae O. MacalesNo ratings yet
- CVD NCD Risk Assessment FormDocument2 pagesCVD NCD Risk Assessment Formsmoothp3akNo ratings yet
- Ventilator Bundle Audit WPB VADocument1 pageVentilator Bundle Audit WPB VAppiNo ratings yet
- Annex EDocument4 pagesAnnex EMarvin Lou GanancialNo ratings yet
- Facility Risk Assessment Form v.2Document1 pageFacility Risk Assessment Form v.2Errol Llanes100% (1)
- Overall Neuropathy Limitations Scale (ONLS)Document2 pagesOverall Neuropathy Limitations Scale (ONLS)juan garcíaNo ratings yet
- Weefim Score Sheet: AmputationsDocument3 pagesWeefim Score Sheet: AmputationsDiedeeNo ratings yet
- S.No 1. Name 3. Age Group 4. Sex 5. Student 6.workingDocument5 pagesS.No 1. Name 3. Age Group 4. Sex 5. Student 6.workingParayulaNo ratings yet
- No. Last Name First Name Age Student/teacher Quality Taste Presentation 1 Dela Cruz Ninna 2 Mag Cammit Hyannis 3 Zeta Dia 4 Paras Odeine 5 D 6 7 8 9 10 11 12 13 14 15Document2 pagesNo. Last Name First Name Age Student/teacher Quality Taste Presentation 1 Dela Cruz Ninna 2 Mag Cammit Hyannis 3 Zeta Dia 4 Paras Odeine 5 D 6 7 8 9 10 11 12 13 14 15Edelyn Daria DollenteNo ratings yet
- 2ndQ Performance Task2 Pair Work Effect of Olfaction On GustationDocument2 pages2ndQ Performance Task2 Pair Work Effect of Olfaction On GustationmayasNo ratings yet
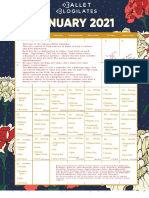
- January 2021 Calendar BalletDocument1 pageJanuary 2021 Calendar BalletzuilinhaNo ratings yet
- SSO Shoulder SLAP Surgery RehabilitationDocument10 pagesSSO Shoulder SLAP Surgery RehabilitationDruga DanutNo ratings yet
- Blanko WeeFIM-Brain-InjuryDocument3 pagesBlanko WeeFIM-Brain-InjuryYusrina RahmaNo ratings yet
- New Questions 1Document2 pagesNew Questions 1ShobhitNo ratings yet
- Daily Behavior Checklist: Student NameDocument4 pagesDaily Behavior Checklist: Student Nameapi-352462796No ratings yet
- Weefim BurnDocument3 pagesWeefim BurnDiedeeNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Edwin DagunotNo ratings yet
- Medical Certificate: To Whom It May Concern:, Daxx Raven L. AgeDocument2 pagesMedical Certificate: To Whom It May Concern:, Daxx Raven L. AgeRobbie Rose LavaNo ratings yet
- Lesson 1 PDFDocument4 pagesLesson 1 PDFLady PichilingueNo ratings yet
- Local Media5932551088838512655Document30 pagesLocal Media5932551088838512655Mariel AttosNo ratings yet
- Local Media5932551088838512655Document30 pagesLocal Media5932551088838512655Mariel AttosNo ratings yet
- 88 Yes-No-Questions US StudentDocument12 pages88 Yes-No-Questions US StudentJulie MulvanyNo ratings yet
- University of Dar Es Salaam: Faculty of Commerce and ManagementDocument37 pagesUniversity of Dar Es Salaam: Faculty of Commerce and ManagementEric MitegoNo ratings yet
- Cultivation and Horticulture of SandalwoodDocument2 pagesCultivation and Horticulture of SandalwoodAnkitha goriNo ratings yet
- Graphs in ChemDocument10 pagesGraphs in Chemzhaney0625No ratings yet
- Nur Syamimi - Noor Nasruddin - Presentation - 1002 - 1010 - 1024Document14 pagesNur Syamimi - Noor Nasruddin - Presentation - 1002 - 1010 - 1024abdulhasnalNo ratings yet
- Agriculture: PAPER 3 Practical TestDocument8 pagesAgriculture: PAPER 3 Practical Testmstudy123456No ratings yet
- IGCSE Religious Studies (Edexcel - 2009 - Be Careful Not To Choose The New' IGCSE)Document8 pagesIGCSE Religious Studies (Edexcel - 2009 - Be Careful Not To Choose The New' IGCSE)Robbie TurnerNo ratings yet
- Historic Trial of Ali Brothers and Shankaracharya-1921Document276 pagesHistoric Trial of Ali Brothers and Shankaracharya-1921Sampath Bulusu100% (3)
- A Person On A Position of Air Traffic ControllerDocument7 pagesA Person On A Position of Air Traffic ControllerMUHAMMAD RAMZANNo ratings yet
- New Life in Christ - Vol05 - Engl - Teacher GuideDocument29 pagesNew Life in Christ - Vol05 - Engl - Teacher GuideOliver Angus100% (1)
- Angelic Spirit Work in The Hoodoo TraditionDocument6 pagesAngelic Spirit Work in The Hoodoo TraditionDaniel Sampaio100% (1)
- Structure of An Atom Revision PaperDocument5 pagesStructure of An Atom Revision PaperZoe Kim ChinguwaNo ratings yet
- PTPL Ir 2018Document383 pagesPTPL Ir 2018Guan WenhaiNo ratings yet
- Competency #14 Ay 2022-2023 Social StudiesDocument22 pagesCompetency #14 Ay 2022-2023 Social StudiesCharis RebanalNo ratings yet
- Organization of Production: Test IiDocument7 pagesOrganization of Production: Test IiKamarul NizamNo ratings yet
- Commissioning 1. Commissioning: ES200 EasyDocument4 pagesCommissioning 1. Commissioning: ES200 EasyMamdoh EshahatNo ratings yet
- UntitledDocument45 pagesUntitledjemNo ratings yet
- Binary To DecimalDocument8 pagesBinary To DecimalEmmanuel JoshuaNo ratings yet
- ns2 LectureDocument34 pagesns2 LecturedhurgadeviNo ratings yet
- Itf EssayDocument18 pagesItf EssayTharshiNo ratings yet
- Unit 8 Atomic Fluorescence Spectrometry PDFDocument23 pagesUnit 8 Atomic Fluorescence Spectrometry PDFCh AswadNo ratings yet
- Satellite Value Chain: Snapshot 2017Document13 pagesSatellite Value Chain: Snapshot 2017syrijal26No ratings yet
- Dania - 22 - 12363 - 1-Lecture 2 Coordinate System-Fall 2015Document34 pagesDania - 22 - 12363 - 1-Lecture 2 Coordinate System-Fall 2015erwin100% (1)
- Dry Docking QuotationDocument4 pagesDry Docking Quotationboen jayme100% (1)
- Liebherr PR 712 Litronic Final DrivesDocument8 pagesLiebherr PR 712 Litronic Final DrivesLiebherr75% (4)
- LP Addition of PolynomialsDocument5 pagesLP Addition of PolynomialsJolina Bagwisa LptNo ratings yet
- Bashar CitateDocument7 pagesBashar CitateCristiana ProtopopescuNo ratings yet
- Marketing Research Completed RevisedDocument70 pagesMarketing Research Completed RevisedJodel DagoroNo ratings yet
- Repeater Panel User GuideDocument24 pagesRepeater Panel User Guideamartins1974No ratings yet
- Thetford c250 InstallationDocument19 pagesThetford c250 InstallationCatalin Bejan100% (1)
- Kalbelia Dance Rajasthan - Kalbelia Rajasthani Folk Dance KalbeliaDocument6 pagesKalbelia Dance Rajasthan - Kalbelia Rajasthani Folk Dance KalbeliarahulgabdaNo ratings yet