You might also like
- Case 4Document5 pagesCase 4Bikash ShresthaNo ratings yet
- Morning Report: 2 March 2021 Night ShiftDocument16 pagesMorning Report: 2 March 2021 Night ShiftWilujeng AnggrainiNo ratings yet
- Anaest CWU ICUDocument13 pagesAnaest CWU ICUHana FauziNo ratings yet
- Case PresentationDocument40 pagesCase PresentationLaxman Lucky'sNo ratings yet
- 2nd Case Scenario BronchitisDocument5 pages2nd Case Scenario BronchitisKasandra Dawn Moquia BerisoNo ratings yet
- WR RSCM SaminemDocument23 pagesWR RSCM SaminemSyarief Mahmud MakkaNo ratings yet
- CopdDocument23 pagesCopdCt Miza100% (2)
- Case Scenario BronchitisDocument4 pagesCase Scenario BronchitisJamelyn AsuncionNo ratings yet
- Pulmonary Sequele After COVID-19Document61 pagesPulmonary Sequele After COVID-19Nandha KumarNo ratings yet
- Dengue FeverDocument46 pagesDengue FeverRohan Prem NairNo ratings yet
- Mesyuarat Teknikal Kematian Penyakit Berjangkit: Patient Name: Ic NoDocument30 pagesMesyuarat Teknikal Kematian Penyakit Berjangkit: Patient Name: Ic Nomatmin07No ratings yet
- Acfrogbrljfmls 12moh9g Xejuq8r Rvex-End2jznh-5pkfr7b6m2fqezl48rpy1sfxosstcb1h5bcgyhkyp0ykwz7qgz0m61cvrh7o Bfxu0wyxfblyh4m67kpjxl1zem4m3fdw4e-H012yimDocument2 pagesAcfrogbrljfmls 12moh9g Xejuq8r Rvex-End2jznh-5pkfr7b6m2fqezl48rpy1sfxosstcb1h5bcgyhkyp0ykwz7qgz0m61cvrh7o Bfxu0wyxfblyh4m67kpjxl1zem4m3fdw4e-H012yimJemy Tamaño MorongNo ratings yet
- Internal Medicine Case PresentationDocument114 pagesInternal Medicine Case PresentationAyen FornollesNo ratings yet
- Name-Age/Sex - MRD No. - Date of Admission - Ward - Address - Diagnosis - History Taking History of Present IllnessDocument17 pagesName-Age/Sex - MRD No. - Date of Admission - Ward - Address - Diagnosis - History Taking History of Present IllnessMeena KoushalNo ratings yet
- MR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDocument23 pagesMR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDr. Surya Abadi KristyoadiNo ratings yet
- Cardiogenic Shock Part 1Document36 pagesCardiogenic Shock Part 1Martin Miguel AmorNo ratings yet
- BOOP Grand발표Document41 pagesBOOP Grand발표ryushihyunNo ratings yet
- Residents Notes LumbaoDocument3 pagesResidents Notes LumbaoRizielle MendozaNo ratings yet
- MR Minggu Shift Pagi, 11 April 2021Document4 pagesMR Minggu Shift Pagi, 11 April 2021Adinda DianNo ratings yet
- Hayu 7Document20 pagesHayu 7abdimoh926No ratings yet
- Case 7 - (Muhamad Adi) FirehawkDocument11 pagesCase 7 - (Muhamad Adi) FirehawkMochamad Rizky HendiperdanaNo ratings yet
- Example of Clinical ReportDocument27 pagesExample of Clinical ReportTheva CharaanNo ratings yet
- Pedia NotesDocument4 pagesPedia NotesDana CastroNo ratings yet
- Phang Mooi CMEDocument35 pagesPhang Mooi CMERaju AjmeraNo ratings yet
- Disampaikan Pada Pemantapan Profesi KGD: Ns. Arcellia Farosyah P., S.Kep., MSCDocument18 pagesDisampaikan Pada Pemantapan Profesi KGD: Ns. Arcellia Farosyah P., S.Kep., MSCpriaji setiadaniNo ratings yet
- Neo Int 9 November 2021Document35 pagesNeo Int 9 November 2021Prima Hari NastitiNo ratings yet
- Case Presentation On Chronic BronchitisDocument20 pagesCase Presentation On Chronic BronchitisSafoora RafeeqNo ratings yet
- 12-04-2021 IGD ALO + CKD On HD + Ascites + CAPDocument4 pages12-04-2021 IGD ALO + CKD On HD + Ascites + CAPFirdha RositaNo ratings yet
- Indri Astutik CAPD Peritonitis RezdyDocument2 pagesIndri Astutik CAPD Peritonitis RezdyWilujeng AnggrainiNo ratings yet
- Cardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIDocument30 pagesCardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIFikriYTNo ratings yet
- Catatan Jaga 29 April 2019Document10 pagesCatatan Jaga 29 April 2019Frizky HapsariNo ratings yet
- Remon CovidDocument13 pagesRemon CovidJuli2022 Semnol-SemsaNo ratings yet
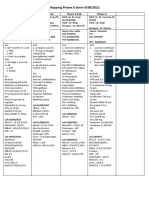
- Mapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Document2 pagesMapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Rina SyafritaNo ratings yet
- IGD BAR Confirmed CovidDocument4 pagesIGD BAR Confirmed CovidWilujeng AnggrainiNo ratings yet
- A Case Report On Multisystemic Inflammatory Syndrome - Children How The Diagnosis and Treatment Could Be ChallengingDocument5 pagesA Case Report On Multisystemic Inflammatory Syndrome - Children How The Diagnosis and Treatment Could Be ChallengingIJAR JOURNALNo ratings yet
- Nursing ProgressDocument7 pagesNursing ProgressNajib ZulkifliNo ratings yet
- The PatientDocument9 pagesThe PatientJan Crizza Dale R. FrancoNo ratings yet
- Apat 2Document4 pagesApat 2rendererichmadarangNo ratings yet
- Laporan Kematian Pang Kim ChoonDocument17 pagesLaporan Kematian Pang Kim ChoonAfifah SelamatNo ratings yet
- COVID-19 Protocol KGMU Version 6.0 17-4-21Document34 pagesCOVID-19 Protocol KGMU Version 6.0 17-4-21Kirtivaan MishraNo ratings yet
- Morbidity Meeting CT Icu (1) (1) - 2 3Document33 pagesMorbidity Meeting CT Icu (1) (1) - 2 3evaNo ratings yet
- S/B DR - Ang SH: General Clerking Note Location:EDRZDocument10 pagesS/B DR - Ang SH: General Clerking Note Location:EDRZbYm456No ratings yet
- Practical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingDocument24 pagesPractical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingyusNo ratings yet
- 29-04-2021 Uremic + Severe Asidosis + CKD + Probable Pneumonia Covid-19Document3 pages29-04-2021 Uremic + Severe Asidosis + CKD + Probable Pneumonia Covid-19Firdha RositaNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument2 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaHelsa EldatarinaNo ratings yet
- Patient Profile Form 1&2-1Document4 pagesPatient Profile Form 1&2-1varishNo ratings yet
- Imam Sutanto Slade 2nefrolitiasis - TB Paru, Pneoumonie Covid 19Document21 pagesImam Sutanto Slade 2nefrolitiasis - TB Paru, Pneoumonie Covid 19dianarahimmNo ratings yet
- Pinere 1 30 Juli 2021Document1 pagePinere 1 30 Juli 2021Rina SyafritaNo ratings yet
- KARDEX Case 3Document3 pagesKARDEX Case 3Juviely PremacioNo ratings yet
- COVID-19 Dengan HipertensiDocument30 pagesCOVID-19 Dengan HipertensifeliNo ratings yet
- Day 1 Day 9Document1 pageDay 1 Day 9abdul hamidNo ratings yet
- Course in The Ward H.InjuryDocument9 pagesCourse in The Ward H.InjuryAllisson BeckersNo ratings yet
- Picu 301Document42 pagesPicu 301I Made DuniaNo ratings yet
- Final Hypertesiion Case For Pharmacotherapycourse WorkDocument37 pagesFinal Hypertesiion Case For Pharmacotherapycourse WorkBhavatharini ArunNo ratings yet
- Mapping Aqsha 3 Senin, 14 Maret 2022Document3 pagesMapping Aqsha 3 Senin, 14 Maret 2022Satrya DitaNo ratings yet
- Type Ii Diabetes: Presented by Thomas Eipe Pharmd InternDocument31 pagesType Ii Diabetes: Presented by Thomas Eipe Pharmd InternThomas EipeNo ratings yet
- Morning: Friday, 6 March 2020Document17 pagesMorning: Friday, 6 March 2020Herka PutraNo ratings yet
- Nursing Care Plan: Student: PhạM Thu QuỳNh Group: 41 Class: Y4QDocument14 pagesNursing Care Plan: Student: PhạM Thu QuỳNh Group: 41 Class: Y4QThảo LÊNo ratings yet
- REV MRJagaTengah - MEDCON - ANI - hyperbilirubinemia+transaminitis+AKIDocument22 pagesREV MRJagaTengah - MEDCON - ANI - hyperbilirubinemia+transaminitis+AKILilik AndayatiNo ratings yet
- Pulmonary Arterial Hypertension: Diagnosis and Evidence-Based TreatmentFrom EverandPulmonary Arterial Hypertension: Diagnosis and Evidence-Based TreatmentRobyn BarstNo ratings yet