You might also like
- Assessing The Utility of ChatGPT Throughout The Entire Clinical WorkflowDocument15 pagesAssessing The Utility of ChatGPT Throughout The Entire Clinical Workflowbeatzmine20No ratings yet
- AI Based Disease Predictor ModelDocument7 pagesAI Based Disease Predictor ModelIJRASETPublicationsNo ratings yet
- Faithful AI in Healthcare and MedicineDocument18 pagesFaithful AI in Healthcare and MedicineEjiofor ChibuikeNo ratings yet
- Disease Prediction and Diagnosis Using Machine LearningDocument6 pagesDisease Prediction and Diagnosis Using Machine LearningIJRASETPublicationsNo ratings yet
- Fin Irjmets1690118387Document4 pagesFin Irjmets1690118387kmp pssrNo ratings yet
- Multi-Disease Prediction Using Machine Learning AlgorithmDocument9 pagesMulti-Disease Prediction Using Machine Learning AlgorithmIJRASETPublicationsNo ratings yet
- Integration and Visualization of Gene Selection and Gene Regulatory Networks for Cancer GenomeFrom EverandIntegration and Visualization of Gene Selection and Gene Regulatory Networks for Cancer GenomeNo ratings yet
- Fin Irjmets1641707340Document5 pagesFin Irjmets1641707340anuradhakushawaha1144No ratings yet
- Combining Structured and Unstructured Data For Predictive Models: A Deep Learning ApproachDocument11 pagesCombining Structured and Unstructured Data For Predictive Models: A Deep Learning ApproachAbdelkader MEJDOUBNo ratings yet
- Human Disease Prediction SystemDocument24 pagesHuman Disease Prediction SystemAbhishek AkNo ratings yet
- Drug Recommendation System Based On Sentiment Analysis of Drug Reviews Using Machine LearningDocument8 pagesDrug Recommendation System Based On Sentiment Analysis of Drug Reviews Using Machine LearningIJRASETPublicationsNo ratings yet
- Garbage in - Out - JAMA - 2023Document3 pagesGarbage in - Out - JAMA - 2023Jose Antonio Tous OlagortaNo ratings yet
- Decision Tree Based Health Prediction SystemDocument8 pagesDecision Tree Based Health Prediction SystemIJRASETPublicationsNo ratings yet
- ChatGPT As A Medical Doctor A Diagnostic Accuracy Study On CommonDocument14 pagesChatGPT As A Medical Doctor A Diagnostic Accuracy Study On Commonagar agarNo ratings yet
- Tribhuvan University Faculty of Education Karve Multiple CampusDocument8 pagesTribhuvan University Faculty of Education Karve Multiple CampusShree krishana ShresthaNo ratings yet
- Machine Learning in Medicine - Jeff DeanDocument12 pagesMachine Learning in Medicine - Jeff DeanArun RaoNo ratings yet
- An Intelligent Disease Prediction and Drug Recommendation Prototype by Using Multiple Approaches ofDocument15 pagesAn Intelligent Disease Prediction and Drug Recommendation Prototype by Using Multiple Approaches ofkmp pssrNo ratings yet
- Human Symptoms Based On Diseases PredictorDocument7 pagesHuman Symptoms Based On Diseases PredictorIJRASETPublicationsNo ratings yet
- A Review of Common Ailments Possibility Using Machine LearningDocument6 pagesA Review of Common Ailments Possibility Using Machine LearningIJRASETPublicationsNo ratings yet
- 1 - Exemplo e Revisão SistemáticaDocument34 pages1 - Exemplo e Revisão SistemáticaRodrigo Cavalcante SabinoNo ratings yet
- Medical Report Translation System Using Artificial Intelligence Concept For Layman UnderstandingDocument5 pagesMedical Report Translation System Using Artificial Intelligence Concept For Layman UnderstandingBashir IdrisNo ratings yet
- SynopsisDocument6 pagesSynopsisVikas KumarNo ratings yet
- Chapter-3 Research Methodology: The Objective of The StudyDocument16 pagesChapter-3 Research Methodology: The Objective of The StudyRitika MishraNo ratings yet
- Mathematical Model of Classification of Human Genome Data For Breast CancerDocument12 pagesMathematical Model of Classification of Human Genome Data For Breast Cancersukanya samantaNo ratings yet
- A Machine Learning Based Healthcare Diagnostic ModelDocument7 pagesA Machine Learning Based Healthcare Diagnostic ModelIJRASETPublicationsNo ratings yet
- Top and Alternate Drug Recommendation SystemDocument3 pagesTop and Alternate Drug Recommendation SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JMDH 413470 Using Chatgpt in Medical Research Current Status and FutureDocument9 pagesJMDH 413470 Using Chatgpt in Medical Research Current Status and FutureGonzalo PontnauNo ratings yet
- Implementing Clinical Decision Support System Using Naïve Bayesian ClassifierDocument6 pagesImplementing Clinical Decision Support System Using Naïve Bayesian ClassifierEditor IJRITCCNo ratings yet
- Data Mining Applications in Healthcare Sector A StudyDocument7 pagesData Mining Applications in Healthcare Sector A StudyMuhja MufidahNo ratings yet
- (IJCST-V10I5P13) :mrs R Jhansi Rani, K Prem Kumar ReddyDocument7 pages(IJCST-V10I5P13) :mrs R Jhansi Rani, K Prem Kumar ReddyEighthSenseGroupNo ratings yet
- Application of Artificial Intelligence in Community-Based Primary Health Care - Systematic Scoping Review and Critical Appraisal - PMCDocument32 pagesApplication of Artificial Intelligence in Community-Based Primary Health Care - Systematic Scoping Review and Critical Appraisal - PMCPAULA REGINA TAVARES VIEIRANo ratings yet
- Artificial Intelligence in Healthcare: Opportunities and Risk For FutureDocument4 pagesArtificial Intelligence in Healthcare: Opportunities and Risk For FutureRetnoNo ratings yet
- Bridging Artificial Intelligence in Medicine With Generative Pre-Trained Transformer (GPT) TechnologyDocument6 pagesBridging Artificial Intelligence in Medicine With Generative Pre-Trained Transformer (GPT) Technologycerberus thanatosNo ratings yet
- Artificial Intelligence and Acute Appendicitis A Systematic Review of Diagnostic and Prognostic ModelsWorld Journal of Emergency SurgeryDocument31 pagesArtificial Intelligence and Acute Appendicitis A Systematic Review of Diagnostic and Prognostic ModelsWorld Journal of Emergency Surgeryoualid-kunNo ratings yet
- Disease Prediction and Treatment Recommendation Using Machine LearningDocument8 pagesDisease Prediction and Treatment Recommendation Using Machine LearningIJRASETPublicationsNo ratings yet
- Combining Structured and Unstructured Data Forpredictive Models A Deep Learning ApproachDocument10 pagesCombining Structured and Unstructured Data Forpredictive Models A Deep Learning ApproachSarmad N. MOHAMMEDNo ratings yet
- Every Bit Counts Using Deep Learning and Vectorization To Analyze Healthcare Big DataDocument24 pagesEvery Bit Counts Using Deep Learning and Vectorization To Analyze Healthcare Big DataFaraz KhanNo ratings yet
- Artificial Intelligence For Long-Term RespiratoryDocument6 pagesArtificial Intelligence For Long-Term Respiratorydrnasir31No ratings yet
- Popdx: An Automated Framework For Patient Phenotyping Across 392 246 Individuals in The Uk Biobank StudyDocument11 pagesPopdx: An Automated Framework For Patient Phenotyping Across 392 246 Individuals in The Uk Biobank StudysubaNo ratings yet
- Intelligent Mining For Disease Prediction Using Short TextsDocument4 pagesIntelligent Mining For Disease Prediction Using Short TextsShubhamNo ratings yet
- Application of Artificial Intelligence I1Document13 pagesApplication of Artificial Intelligence I1Tolosa TafeseNo ratings yet
- Deep Learning Architectures For Multi-Label Classification of Intelligent Health Risk Prediction - BMC Bioinformatics - Full TextDocument40 pagesDeep Learning Architectures For Multi-Label Classification of Intelligent Health Risk Prediction - BMC Bioinformatics - Full TextBk RayenNo ratings yet
- Nejme 2206291 T 999 T 99 T 9Document2 pagesNejme 2206291 T 999 T 99 T 9Adrian Dacosta LazeraNo ratings yet
- 10.1177 20552076221147423Document8 pages10.1177 20552076221147423Monica CabaNo ratings yet
- Medical Disease Prediction Using Machine Learning AlgorithmsDocument10 pagesMedical Disease Prediction Using Machine Learning AlgorithmsIJRASETPublicationsNo ratings yet
- Disease Prediction Using Machine LearningDocument9 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- AI in MedicineDocument4 pagesAI in MedicinemjNo ratings yet
- Algorithms For Rapid Digitzation of PrescriptionsDocument16 pagesAlgorithms For Rapid Digitzation of PrescriptionsATHARVA INAMDARNo ratings yet
- Disease Prediction Using Machine LearningDocument6 pagesDisease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Digital Prescription and Disease Prediction Using Machine LearningDocument8 pagesDigital Prescription and Disease Prediction Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2023 03 08 23286976 FullDocument48 pages2023 03 08 23286976 FullAnandhu GNo ratings yet
- Disease Prediction Application Using Machine LearningDocument12 pagesDisease Prediction Application Using Machine LearningIJRASETPublicationsNo ratings yet
- Automating Medical Data and Using Data Science For Heart Disease PredictionDocument6 pagesAutomating Medical Data and Using Data Science For Heart Disease PredictionIJRASETPublicationsNo ratings yet
- Materials Today: Proceedings: Ravisankar Malladi, Prashanthi Vempaty, Goutham Raju K, Vyshnavi PogakuDocument6 pagesMaterials Today: Proceedings: Ravisankar Malladi, Prashanthi Vempaty, Goutham Raju K, Vyshnavi PogakuSrinivas KanakalaNo ratings yet
- Plagiarism Checker X Originality Report: Similarity Found: 12%Document10 pagesPlagiarism Checker X Originality Report: Similarity Found: 12%Project DevelopmentNo ratings yet
- Medicine Prescription Using Machine LearningDocument6 pagesMedicine Prescription Using Machine LearningGRD JournalsNo ratings yet
- Computerized Provider Order Entry (CPOE) System - EditedDocument7 pagesComputerized Provider Order Entry (CPOE) System - Editedmutisya johnboscoNo ratings yet
- Predicting Clinically Promising Therapeutic Hypotheses Using Tensor FactorizationDocument12 pagesPredicting Clinically Promising Therapeutic Hypotheses Using Tensor FactorizationKarl GemayelNo ratings yet
- Clinical Decision Support System: Fundamentals and ApplicationsFrom EverandClinical Decision Support System: Fundamentals and ApplicationsNo ratings yet
- MINIMAR (MINimum Information For Medical AI)Document5 pagesMINIMAR (MINimum Information For Medical AI)sbutelli.almawaveNo ratings yet
- Work Based Assessment A Practical GuideDocument38 pagesWork Based Assessment A Practical GuideShajita DNo ratings yet
- 10th Grade Mural City Text - QuestionsDocument2 pages10th Grade Mural City Text - QuestionsMohammed YahyaNo ratings yet
- Pax Forecast Infographic 2020 FinalDocument1 pagePax Forecast Infographic 2020 Finallibardo silvaNo ratings yet
- Belinda Dwi Sukma Putri - ResumeDocument2 pagesBelinda Dwi Sukma Putri - ResumeDiah AyuNo ratings yet
- Valid Arguments For Tariffs or Export SubsidiDocument1 pageValid Arguments For Tariffs or Export SubsidiTrang Chử ThuNo ratings yet
- ChemistryDocument16 pagesChemistryShashank Dubey0% (1)
- Advanced Pricing in PurchasingDocument27 pagesAdvanced Pricing in PurchasingMohmed BadawyNo ratings yet
- Failure Modes For Trees and Related Criteria - Mattheck Et - Al. 2003Document12 pagesFailure Modes For Trees and Related Criteria - Mattheck Et - Al. 2003Chromaticghost2No ratings yet
- Microservice PatternDocument1 pageMicroservice PatternHari Haran M100% (1)
- Pickle Making 22 July 2019 Syllabus Niesbud NoidaDocument3 pagesPickle Making 22 July 2019 Syllabus Niesbud NoidaTouffiq SANo ratings yet
- Nature and Morphology of Ore DepositsDocument7 pagesNature and Morphology of Ore DepositsIrwan EP100% (3)
- Skill Trees 1-6-23 (40594786)Document21 pagesSkill Trees 1-6-23 (40594786)Scribble StixNo ratings yet
- PERICULUM Process BookDocument13 pagesPERICULUM Process BookZhao MingNo ratings yet
- RollPlayer FamiliarsDocument12 pagesRollPlayer FamiliarsХуан Брухо100% (1)
- Factors Affecting Online Buying BehaviorDocument17 pagesFactors Affecting Online Buying BehaviorJohn DoeNo ratings yet
- MLX91208 Datasheet Melexis PDFDocument19 pagesMLX91208 Datasheet Melexis PDFTrần LinhNo ratings yet
- Reading W1 SmokingDocument9 pagesReading W1 SmokingLinh Phương TrầnNo ratings yet
- General: Preferred Jobs To Work (Position(s) You Want To Apply For)Document4 pagesGeneral: Preferred Jobs To Work (Position(s) You Want To Apply For)voodoonsNo ratings yet
- Signaling Server: Installation and ConfigurationDocument118 pagesSignaling Server: Installation and Configurationwanriz1971No ratings yet
- 10G DWDM Linecard: 10G DWDM Linecard With Support For 10gbe and Oc192/Stm64 - XFP BasedDocument2 pages10G DWDM Linecard: 10G DWDM Linecard With Support For 10gbe and Oc192/Stm64 - XFP BasedMichele BrunelliNo ratings yet
- Problem StatementDocument2 pagesProblem StatementKanthan AmalNo ratings yet
- CimentacionDocument1 pageCimentacionLeonardo Ramirez GuzmanNo ratings yet
- Working in The Dark Understanding The Presuicide State of MindDocument8 pagesWorking in The Dark Understanding The Presuicide State of MindAntonia InaNo ratings yet
- Research Journal of Internatıonal StudıesDocument16 pagesResearch Journal of Internatıonal StudıesShamsher ShirazNo ratings yet
- Belt Conveyor Pulley DesignDocument11 pagesBelt Conveyor Pulley Designthakur_raghab100% (1)
- Nationwide Syntac CatalogDocument100 pagesNationwide Syntac Cataloglatina_sebastianNo ratings yet
- Terminating A Swap ContractDocument2 pagesTerminating A Swap Contractravi_nyseNo ratings yet
- Genetic EngineeringDocument35 pagesGenetic Engineeringjosh321No ratings yet
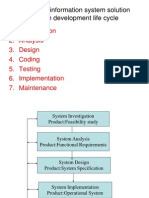
- Developing Information System SolutionDocument42 pagesDeveloping Information System SolutionAbhijeet Mahapatra71% (7)
- ZBBR 123Document11 pagesZBBR 123Tony Peterz Kurewa0% (1)