You might also like
- AUH Travel Declaration FormDocument2 pagesAUH Travel Declaration FormAbdul RahmanNo ratings yet
- Self-Declaration Form For Abu DhabiDocument2 pagesSelf-Declaration Form For Abu DhabitravelobizNo ratings yet
- Manship App FormDocument4 pagesManship App Formjonheric2009No ratings yet
- NTT Application Form (APAC)Document3 pagesNTT Application Form (APAC)RahulNo ratings yet
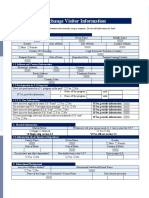
- Exchange Visitor InformationDocument3 pagesExchange Visitor InformationPrathamesh ParabNo ratings yet
- Protect your health by completing this contact tracing formDocument2 pagesProtect your health by completing this contact tracing formIrfan MustafaiNo ratings yet
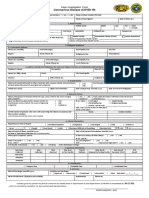
- CIF (For BMDL PhilHealth Purposes Only)Document1 pageCIF (For BMDL PhilHealth Purposes Only)BALIUAG DISTRICT LABORATORYNo ratings yet
- Philippine COVID-19 Case Investigation FormDocument1 pagePhilippine COVID-19 Case Investigation FormmaelisaNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Employee Personal Information Form - Onjoining: Please Complete All Section in FullDocument2 pagesEmployee Personal Information Form - Onjoining: Please Complete All Section in FullSarah DaviesNo ratings yet
- UK Visa FormDocument5 pagesUK Visa FormJofrey FurigayNo ratings yet
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- Ca Potential Client Intake FormDocument5 pagesCa Potential Client Intake Formbash shangNo ratings yet
- Victim Informatio N Form - For "Complaina NT" or "Civil Party" (English)Document5 pagesVictim Informatio N Form - For "Complaina NT" or "Civil Party" (English)kilettersNo ratings yet
- Holmesglen App FormDocument8 pagesHolmesglen App FormssshalNo ratings yet
- Self Declaration Form MeluhaDocument1 pageSelf Declaration Form MeluhaSandy BergerNo ratings yet
- AGWM Claim Form & Authorization Filing Instructions: PART A. To Be Completed by The Claimant For All ClaimsDocument5 pagesAGWM Claim Form & Authorization Filing Instructions: PART A. To Be Completed by The Claimant For All ClaimsCreations CloverNo ratings yet
- Heath Secure Application Form: Only For: Bahrain, Qatar, Oman, Northern Emirates Except AUHDocument2 pagesHeath Secure Application Form: Only For: Bahrain, Qatar, Oman, Northern Emirates Except AUHRey GitganoNo ratings yet
- Health Decleration PDFDocument1 pageHealth Decleration PDFNithinKallayilNo ratings yet
- Case Management Assessment FormDocument13 pagesCase Management Assessment FormDiksha PadamNo ratings yet
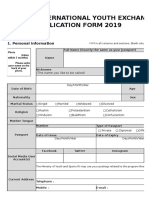
- International Youth Exchange Aplication Form 2019Document8 pagesInternational Youth Exchange Aplication Form 2019Abiyyu PrayogaNo ratings yet
- Registration Form: (Private and Confidential Once Completed)Document7 pagesRegistration Form: (Private and Confidential Once Completed)Gideon AffleckNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- Pre-Interview QuestionnaireDocument5 pagesPre-Interview Questionnairebishirmuhammadyuda2140No ratings yet
- WAS Co5 ApplicationDocument4 pagesWAS Co5 ApplicationWaterfordFireDepartmentNo ratings yet
- Draft of Online Us Nonimmigrant Visa FormDocument4 pagesDraft of Online Us Nonimmigrant Visa Formjobert de jesusNo ratings yet
- Employment Application Form-DASSDocument2 pagesEmployment Application Form-DASSnavin212No ratings yet
- Pacific Labour Scheme Application: Secretariat of State For Vocational Training and EmploymentDocument4 pagesPacific Labour Scheme Application: Secretariat of State For Vocational Training and Employmentjeme jesemNo ratings yet
- Application For Visa or Transit VisaDocument3 pagesApplication For Visa or Transit VisamagretNo ratings yet
- Write Clearly and in Block Letters: Personal DataDocument2 pagesWrite Clearly and in Block Letters: Personal Datanahian bd100% (1)
- Reca DW Claim Form 12-11-0Document25 pagesReca DW Claim Form 12-11-0Ehren OertellNo ratings yet
- Full Time Application Form SU2023Document6 pagesFull Time Application Form SU2023Mohamed ElsagerNo ratings yet
- INTERNATIONAL YOUTH EXCHANGE APPLICATIONDocument3 pagesINTERNATIONAL YOUTH EXCHANGE APPLICATIONAmii ThaytamiiNo ratings yet
- 2. Application for EmploymentDocument2 pages2. Application for Employmentrijwan.md1989No ratings yet
- EXIM Application FormDocument3 pagesEXIM Application Formchristian.gomez.gtNo ratings yet
- Asylum Support Application Form ASF1Document36 pagesAsylum Support Application Form ASF1cococatelulNo ratings yet
- 1.formal ApplicationDocument8 pages1.formal ApplicationNaturalBite ChefNo ratings yet
- Health Declaration Form (8th Edition)Document1 pageHealth Declaration Form (8th Edition)Car LynNo ratings yet
- Application Form TAG New - Fillable 161108 Punya AyyangDocument4 pagesApplication Form TAG New - Fillable 161108 Punya Ayyangervayeppoyo7No ratings yet
- Application For EmploymentDocument5 pagesApplication For EmploymentFennia Bintari PutriNo ratings yet
- msp12183 Critical Illness Ben Claim Form 420Document7 pagesmsp12183 Critical Illness Ben Claim Form 420Anush VedhNo ratings yet
- Application For ObserverDocument4 pagesApplication For Observerসোমনাথ মহাপাত্রNo ratings yet
- Employment ApplicationDocument2 pagesEmployment ApplicationdioneeNo ratings yet
- RM - Information of The Foreign Worker PDFDocument6 pagesRM - Information of The Foreign Worker PDFMelchor BacasenNo ratings yet
- Personal Details Update: Zurich International LifeDocument2 pagesPersonal Details Update: Zurich International LifeMuhammad Suhaib FaryadNo ratings yet
- Evergreen Habitat For Humanity: Program Eligibility Assessment For HousingDocument4 pagesEvergreen Habitat For Humanity: Program Eligibility Assessment For HousingJessica NulphNo ratings yet
- South African Visa Application FormDocument20 pagesSouth African Visa Application FormI QNo ratings yet
- Residential Lots Application Form: Section A: Main Applicant'S Personal InformationDocument2 pagesResidential Lots Application Form: Section A: Main Applicant'S Personal InformationAnthony BasantaNo ratings yet
- References From Family Members Are Not ValidDocument2 pagesReferences From Family Members Are Not ValidAlisha underwoodNo ratings yet
- Employment Application: - Please Answer Each Column Fully and Neatly in Your Own HandwritingDocument5 pagesEmployment Application: - Please Answer Each Column Fully and Neatly in Your Own Handwritingform centerNo ratings yet
- Case Management Assessment FormDocument13 pagesCase Management Assessment Formiman diarNo ratings yet
- Dublin Extra Questionnaire 2009Document4 pagesDublin Extra Questionnaire 2009bigacquayeNo ratings yet
- Disability Claim Form 7days Waiting EngDocument3 pagesDisability Claim Form 7days Waiting EngJonathan BorleyNo ratings yet
- Assessment form personal detailsDocument4 pagesAssessment form personal detailsAkash BodekarNo ratings yet
- Barrington Residential Prospective Resident Application ProcessDocument5 pagesBarrington Residential Prospective Resident Application Process568224736No ratings yet
- Applying To Become A Member of The Discovery Health Medical Scheme 2018Document15 pagesApplying To Become A Member of The Discovery Health Medical Scheme 2018simbamikeNo ratings yet
- Employee Application Form Secana R3Document5 pagesEmployee Application Form Secana R3TiawidyalestariNo ratings yet
- COVID19 TRAVEL SCREENING QUESTIONNAIREDocument1 pageCOVID19 TRAVEL SCREENING QUESTIONNAIREHouda BellaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formmatingin.aileen11No ratings yet
- Grade Thresholds - November 2018: Cambridge O Level Second Language Urdu (3248)Document1 pageGrade Thresholds - November 2018: Cambridge O Level Second Language Urdu (3248)Uzair KhanNo ratings yet
- YIFYStatus.comDocument1 pageYIFYStatus.comrishi reddyNo ratings yet
- Cambridge IGCSE™: Accounting 0452/23 October/November 2020Document14 pagesCambridge IGCSE™: Accounting 0452/23 October/November 2020ATTIQ UR REHMANNo ratings yet
- CIE IGCSE Accounting Past PaperDocument12 pagesCIE IGCSE Accounting Past PaperHan Thi Win KoNo ratings yet
- Med - Surg Sample QuestionDocument55 pagesMed - Surg Sample QuestionCHARLYN DELOS REYESNo ratings yet
- Cossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberDocument2 pagesCossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberRocky BisNo ratings yet
- Alstom19475 Asbestos.Document4 pagesAlstom19475 Asbestos.MANOJ KUMARNo ratings yet
- Chronic Cough in Dogs: Published With The Permission of LAVC Close Window To Return To IVISDocument4 pagesChronic Cough in Dogs: Published With The Permission of LAVC Close Window To Return To IVISJuanEstebanOspinaNo ratings yet
- Gambaran Radiologi ThoraxDocument23 pagesGambaran Radiologi ThoraxAchmad MuhazirNo ratings yet
- Karnataka COVID-19 Media Bulletin Provides Latest Case UpdatesDocument14 pagesKarnataka COVID-19 Media Bulletin Provides Latest Case UpdatesKiran SNNo ratings yet
- First Aid Notes 2019Document84 pagesFirst Aid Notes 2019Fredrick WedderburnNo ratings yet
- User Manual: VT5230 VentilatorDocument183 pagesUser Manual: VT5230 VentilatorArtur FloriánNo ratings yet
- Chapter 2 EnglishDocument5 pagesChapter 2 EnglishdwiNo ratings yet
- Literature Review 1Document7 pagesLiterature Review 1api-549225118No ratings yet
- Gumarny Zubri OM 90 Mask SpecificationDocument3 pagesGumarny Zubri OM 90 Mask SpecificationCaramiafanNo ratings yet
- Pulmonary Edema Vs Pneumonia OrderDocument25 pagesPulmonary Edema Vs Pneumonia OrderRizqon RohmatussadeliNo ratings yet
- Laboratory Exercise 41 Respiratory SystemDocument1 pageLaboratory Exercise 41 Respiratory SystemNikki RodriguezNo ratings yet
- Group 2 Cardiovascular and Respiratory System of GymnastDocument19 pagesGroup 2 Cardiovascular and Respiratory System of GymnastSariephine Grace ArasNo ratings yet
- As An Airborne DiseaseDocument3 pagesAs An Airborne DiseaseGabby CabanesNo ratings yet
- Efects of Inspiratory Muscle Training in Older AdultsDocument10 pagesEfects of Inspiratory Muscle Training in Older AdultsMaría Camila Zuluaga AriasNo ratings yet
- G-9 Summative Test 1 (WK 1-2)Document2 pagesG-9 Summative Test 1 (WK 1-2)Colleen RubiaNo ratings yet
- MSDS SUN&RAIN ELASTOMERIC ColoredDocument3 pagesMSDS SUN&RAIN ELASTOMERIC ColoredLola Tesie0% (1)
- AclsDocument44 pagesAclsArchana GaonkarNo ratings yet
- Garcia NGT NCPDocument1 pageGarcia NGT NCPFrances Katherine GarciaNo ratings yet
- Nursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NDocument7 pagesNursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NNajla Kaye PerezNo ratings yet
- Ocm1 Confined SpaceDocument2 pagesOcm1 Confined SpacerapidsicuminteNo ratings yet
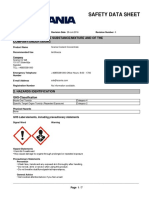
- Safety Data Sheet: 1. Identification of The Substance/Mixture and of The Company/UndertakingDocument7 pagesSafety Data Sheet: 1. Identification of The Substance/Mixture and of The Company/UndertakingСергій БоженкоNo ratings yet
- Measurements of The Respiratory SystemDocument36 pagesMeasurements of The Respiratory SystemKrishnaswamy RajaNo ratings yet
- Jurnal Silikosis Dengan Pneumothorax PDFDocument6 pagesJurnal Silikosis Dengan Pneumothorax PDFfalisNo ratings yet
- Community Service ReportDocument5 pagesCommunity Service Reportkmkk advocacycooperativeNo ratings yet
- Anaesthetic Machine ScbaileyDocument57 pagesAnaesthetic Machine ScbaileyOğuzhan AltıparmakNo ratings yet
- Lampiran Peraturan Kepala Desa Bulusulur Nomor TanggalDocument8 pagesLampiran Peraturan Kepala Desa Bulusulur Nomor TanggalSita SidhartaNo ratings yet
- 1 s2.0 S1836955322001199 MainDocument8 pages1 s2.0 S1836955322001199 MainMarcin BystrowskiNo ratings yet
- Module 4 Electrical SafetyDocument12 pagesModule 4 Electrical SafetyNaveen S BasandiNo ratings yet